TO TEST OR NOT TO TEST?
advertisement

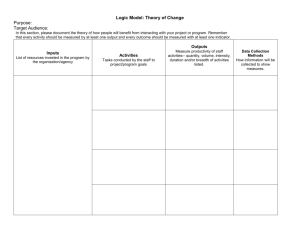
TO TEST OR NOT TO TEST? THE ROLE OF ATTITUDES, RELIGIOUS INVOLVEMENT, KNOWLEDGE AND PREVIOUS EXPERIENCE IN FORMING INTENT-TO-OBTAIN PREDICTIVE ADULT GENETIC TESTING – A STRUCTURAL EQUATION MODELING APPROACH Anda Botoseneanu, MD/MBA Jeffrey A. Alexander, Ph.D Jane Banaszak-Holl, Ph.D Health Management and Policy Department University of Michigan Background Genetic susceptibility testing: Cancers –breast, colon, prostate Other dx – SSA, cystic fibrosis, etc Risk: HNPCC genes – 70-80% early onset-cancer BRCA 1 and 2 – 85% breast Ca and 65% ovarian Ca by age 70y Risk-reduction surveillance and interventions: Prophylactic mastectomy – 80-90% risk-reduction BPO – 85-96% risk-reduction (Ackermann et al., 2006) Study Justification Uptake of genetic testing among low- and high-risk groups is low. Predictions on GT uptake intentions scanty (Li et al., 2004). Factors influencing consumers’ choices re: GT uptake ? (Ackermann et al., 2006). Model of Theory of Reasoned Action (TRA) & Objective • Attitudes/knowledge/beliefs behavioral intentions actual behaviors (Ajzen and Fishbein, 1980, 1985, 1991) • Sociodemographics, culture/religion/stereotypes & biases towards targets, psychological factors (social pressures) attitudes. (Fishbein and Yzer, 2003) Examine role of ATTITUDES, KNOWLEDGE, PREVIOUS EXPERIENCE, RELIGIOUS INVOLVEMENT for intent to obtain genetic testing O1: Test role of religion in forming intent-to-test. O2: Test model of direct and indirect (mediated) effects. MODEL Development - RELIGION Religion health outcomes (physical, mental, functional). (Koenig et al, 2001; Moreira-Almeida et al., 2006, Hummer et al., 2004) Religion lower utilization of hospital services BUT higher utilization of SOME preventive services. (Koenig et al., 2004, 1998; Benjamins and Brown, 2003 ) Religion GT interest, attitudes, knowledge (-) (Bowen, 2003; Chatters, 2000) Why religion? Faith-based venues for health prevention & screening adherence (Peterson et al., 2002) Importance of religion in life decisions (GSS findings) PROPOSED MODEL Religious Involvement (-) Knowledge on GT (-) (+) (-) Attitudes vs. GT (+) Previous Experience w. GT (+) (+) (+) Behavioral Intentions Data Source & Sample UNITED STATES PUBLIC KNOWLEDGE AND ATTITUDES ABOUT GENETIC TESTING, 2000 (Robert Wood Johnson Foundation, April 2000 to November 2000 (updated 2005) - ICPSR ). Cross-sectional. Sample: nationally representative sample of adult US population – 1,824 adults ages 18 and over. Analytic Approach SEM 2-step analysis (Loehlin, 2004): 1. 2. Confirmatory Factor Analysis (CFA) – test measurement model. Structural Equation Model (SEM) – test the paths (direct and indirect effects) model. M-plus software Robust WLS estimation method (asymptotically distribution-free estimation method), with FIML for missing data. Results – Final Model Results – Variance Variance explained (1-residual) : BEHINT 15.2% RelInv on ATT 1.7% MI – no modification warranted. Conclusions: 1. Attitudes (positive), experience (positive) and knowledge (negative) had DIRECT effects on Intention-to-Test. 2. Religious Involvement has INDIRECT effect (negative) via held attitudes. 3. 15% of the variance in intention-to-test explained other factors. Limitations 1. Measures have narrow theoretical boundaries: Attitudes not considered: (1) perceptions about personal risk for adult genetic disorders (Shiloh and Ilan, 2005), (2) attitudes about autonomy and confidentiality (Benkendorf et al., 1997), (3) attitudes towards uncertainty (Braithwaite et al., 2002), (4) beliefs about the normative expectations of others (family, friends, fellow church-goers, etc) (Ajzen, 2002) Religious involvement measure vs. denomination, vs. religious identification, vs. etc… Knowledge: accuracy of test results, complications/side effects, Tx options 2. Behavioral intentions predict actual behavior? 3. Causality Inference? Study Implications Understanding the mechanisms of GT behavioral intentions formation will help with: (1) Identifying groups (based on levels of religious involvement) which are more or less receptive to participation in cancer genetic testing. (2) Identifying attitudinal barriers to participation in GT and suggest ways to overcome them. (3) Allowing for tailoring genetic screening messages, information and interventions to address attitudinal barriers. Genetic Testing Behaviors: Where Do We (Hope to) Go from Here? Study 1: GENDER differences: Screening programs/policies for breast cancer (females mostly), prostate cancer (males-only) and colon cancer (both genders) should take into account gender differences in formation of behavioral intentions. Study 2: ATTITUDES: (1) Perceptions about personal risk for adult genetic disorders/Risk tolerance. (2) Attitudes about autonomy and confidentiality. (3) Attitudes towards uncertainty. (4) Beliefs about the normative expectations of others. Study 3: What is it about religion? Study 4: BEHAVIORAL INTENTIONS PREDICT ACTUAL BEHAVIOR?