Call for Panels
advertisement

Call for Panels Call for Panels HCUP: A National Information Resource to Support Children’s Health Care Research and to inform Health Care Policy and Practice Chair: Anne Elixhauser, Ph.D. Saturday, June 25 • 10:00 a.m. - 11:45 a.m. ● Hospitalization Rates Among Children and Adolescents in the U.S. Anne Elixhauser, Ph.D., Tamar Lasky, Ph.D., Robert Baskin, Ph.D. Presented by: Anne Elixhauser, Ph.D., Senior Research Scientist, Center for Delivery, Organization, and Markets, Agency for Healthcare Research and Quality, 540 Gaither Road, Rockville, MD 20850; Tel: (301) 427-1411; Fax: (301) 427-1430; E-mail: aelixhau@ahrq.gov Research Objective: Provide information on rates of hospitalization for children and adolescents to help with priority-setting under the Best Pharmaceuticals for Children Act (BPCA). Study Design: We conducted cross-sectional analysis of hospital administrative data from the Healthcare Cost and Utilization Project (HCUP) Kids' Inpatient Database (KID) for 2000. ICD-9-CM codes for principal diagnosis were categorized using the Clinical Classification Software. We calculated rates per 100,000 population (based on data from the Bureau of the Census), relative rates, and 95% confidence intervals around relative rates for 0-17 year olds, by age group (0-1, 2-4, 5-11, 12-17), by gender, and by primary expected payer private, Medicaid, other/uninsured). Population Studied: Hospital discharges for children 0-17 years. Principal Findings: The top three most common conditions in the hospital for all 0-17 year olds were pneumonia (227 discharges/100,000), asthma (211/100,000), and acute bronchitis/bronchiolitis (201/100,000). Fluid and electrolyte disorders (number 4 with 124/100,000) and intestinal infections (number 10, 66/100,000) also ranked in the top 10. The 6th most common condition for all children was mood disorders (103/100,000) and the 7th was maternal complications for pregnant adolescents (86/100,000). Appendicitis (number 5, 107/100,000), epilepsy/convulsions (number 8, 79/100,000), and urinary infections (68/100,000) were also high frequency conditions. Among 12-17 years olds, 5 of the top 10 conditions were related to adolescent pregnancy (e.g., early or threatened labor). All pregnancyrelated conditions, combined, are the most common reason for hospitalization among 12-17 year olds. Excluding pregnancy and childbirth, analyses by age group revealed some conditions that were common across multiple age groups. Asthma and pneumonia are top 10 conditions for every age group. Fluid/electrolyte disorders and UTI are top 10 conditions for 0-1, 2-4, and 5-11 year olds. Chemotherapy/radiation therapy is in the top 10 for 2-4, 5-11, and 12-17 year olds. Bronchitis/bronchiolitis, intestinal infection, and URI are in the top 10 for 0-1 and 2-4 year olds. Epilepsy/convulsions is in the top 10 for 2-4 year olds and 5-11 year olds. Appendicitis and mood disorders are top 10 conditions for 5-11 and 12-17 year olds. Birth complications, premature birth and low birth weight, and viral infections are the other top 10 conditions for 0-1 year olds. For 5-11 year olds, appendicitis, arm fracture, and skin infections are top 10 conditions. For 12-17 year olds brain injury, leg fracture, diabetes complications, poisoning by medications, and other mental disorders are top 10 conditions. For the top 10 conditions overall, males were more likely to be hospitalized than females except for maternal complications, mood disorders, and urinary infections (all more common in females). For the top 10 conditions, Medicaid patients were more likely to be hospitalized than privately insured patients. "Other" patients - primarily the uninsured - were less likely to be hospitalized. Conclusions: This study provides information on the most common reasons for hospitalization among children and adolescents and reveals variations by subgroup that are related to developmental stage and social differences. Implications for Policy, Delivery or Practice: These data are useful in understanding the distribution of diagnoses associated with pediatric hospitalization and variations by age, sex and payer status. Primary Funding Source: AHRQ, National Institute for Child Health and Human Development ● Population-Based Volumes, Rates and Resource Use for Pediatric Cardiac Procedures Darryl Gray, M.D., Sc.D. Presented by: Darryl Gray, M.D., Sc.D., Medical Officer, Center for Quality Improvement and Patient Safety, Agency for Healthcare Research and Quality, 540 Gaither Road, Rockville, MD 20850; Tel: (301) 427-1326; Fax: (301) 427-1341; E-mail: dgray@ahrq.gov Research Objective: Congenital malformations of the heart and great vessels affect roughly one million Americans. Acquired conditions (generally of infectious origin) add to the growing burden of pediatric heart disease seen in children and adults. While relevant diagnostic and therapeutic options are expanding, little is known in aggregate about the frequencies of procedures used to treat these conditions. Administrative data were used to estimate population-based volumes, rates, and resource use for the inpatient cases estimated to comprise ~90% of pediatric therapeutic cardiac procedures (PTCPs). Study Design: For a retrospective descriptive study, ICD-9CM procedure codes for discharges with PTCP performed via surgical or transcatheter approaches were determined. Based on the principal procedure coded, publicly-available, nationally extrapolated aggregate data on inpatient PTCPs were obtained from HCUPnet for HCUP’s Kids' Inpatient Database (KID) and the Nationwide Inpatient Sample (NIS). HCUPnet is an on-line query system that provides access to information on hospital stays based on HCUP data. Hospital charges, which exceed costs but exclude physician fees, were aggregated (mean charges X admission volumes) and expressed in 2002 dollars using the Consumer Price Index (CPI). Volumes were combined with Census data to generate population-based rates. Population Studied: Weighted, nationally representative samples of admissions of 0-17 year olds (YOs). Principal Findings: KID data from 1997 indicate that infant (< 1 YO) discharges with PTCPs accounted for 15,024 hospital discharges (384.6/100,000 infants). A mean length of stay (MLOS) of 23.0 days generated CPI-adjusted aggregate charges of $147,091/discharge. Among 1-17 YOs, KID estimated that 14,607 discharges with PTCP (21.9/100,000) had an MLOS of 6.1 days and charges averaging $61,458/discharge. Charges for 0-17 YOs totaled $3.1 billion. For 1997, NIS estimated that 12,827 infant discharges with PTCP generated a MLOS of 21.9 days, and charges averaging $128,359/discharge. For 1-17 YOs, 14,067 discharges averaging 6.4 days generated charges of $48,984/discharge. Charges for 0-17 YOs totaled $2.3 billion. MLOS figures and the relative contributions of infants versus older children to discharge volumes and to charges remained relatively stable over time and across databases. However, for all ages, NIS absolute volumes rose from 20,657 in 1998 to 32,368 in 1999, and dropped to 23,400 discharges in 2000. Aggregate charges were $1.6 billion, $3.0 billion and $2.3 billion respectively. In 2000, KID estimated that 30,861 discharges generated $2.4 billion in charges. For 2002, NIS estimated that 24,691 discharges generated $3.1 billion in charges. Conclusions: Nationwide PTCP volumes and resource use appear to exceed prior estimates. Infants (including newborns) account for roughly 1/2 of these discharges and >2/3 of associated charges. While NIS appears annually, its estimates for relatively rare procedures (PTCP’s) may fluctuate. KID (released for 1997 and 2000; 2003 pending) oversamples pediatrics discharges and may better capture such care. Implications for Policy, Delivery or Practice: The considerable volumes and costs associated with pediatric cardiac procedures indicate the societal importance of these interventions. These figures argue for increased populationbased research on care patterns and outcomes, especially for infants. Such research may use data from HCUP and other sources to distinguish the effects of sampling variation or artifact from those of major changes in actual procedure volumes and/or resource use. Primary Funding Source: Agency for Healthcare Research and Quality, National Heart, Lung and Blood Institute ● Hospitalizations for Children with Mental Health and Substance Abuse Conditions Pamela Owens, Ph.D., Anne Elixhauser, Ph.D. Presented by: Pamela Owens, Ph.D., Research Scientist, Center for Delivery, Organization, and Markets, Agency for Healthcare Research and Quality, 540 Gaither Road, Rockville, MD 20850; Tel: (301) 427-1438; Fax: (301) 427-1430; E-mail: powens@ahrq.gov Research Objective: To compare pediatric hospitalizations for mental health and substance abuse conditions (MHSA) to pediatric hospitalizations for general medical conditions. Study Design: A cross-sectional analysis of 2002 Healthcare Cost and Utilization Project (HCUP) Nationwide Inpatient Sample (NIS) was conducted. The NIS is a stratified probability sample of discharges from about 1,000 community hospitals in 36 States. The Clinical Classifications Software (CCS) and a new mental health substance abuse CCS supplement was used to classify ICD-9-CM principal and secondary diagnostic codes and identify three major subgroups of pediatric hospital stays: 1) children with a principal MHSA condition, 2) children with a secondary MHSA condition only, and 3) children with no MHSA condition. Age-specific national estimates of characteristics of pediatric hospitalizations (length of stay, expected payer, admission and discharge status and total charges) were examined for each of the three subgroups. Population Studied: U.S. community hospital stays for children ages 0-17 years. Principal Findings: Of the 1.7 million hospitalizations for children 1-17 in US community hospitals, 13.8% were for children with a principal or secondary MHSA condition. Of those hospitalizations for a principal MHSA condition, most were for mood disorders (54.1%), disruptive behavior disorders (14.4%), alcohol and substance abuse disorders (7.5%) and adjustment disorders (5.8%). Hospitalizations for MHSA conditions occurred more frequently among older children compared with younger children (3.1% of hospitalizations for 1-4 year olds (YO), 11.0% for 5-9 YO, 21.5% for 10-14 YO, and 21.7% for 15-17 YO, p<.001). Hospitalizations for children with a principal MHSA condition were likely to be longer (mean length of stay (LOS) = 9.4 days) compared with hospitalizations for children with comorbid MHSA conditions (mean LOS = 4.9 days) or no MHSA conditions (mean LOS = 3.2 days). Mean total charges of hospitalizations for principal MHSA conditions (mean: $14,000) were similar to total charges for hospitalizations unrelated to MHSA conditions (mean: $13,500), but significantly less than total charges for hospitalizations with comorbid MHSA conditions (mean: $21,300) (p< .001). Although no significant differences were noted in the aggregate, age stratified analyses revealed significant differences in expected source of payment for each of the three subgroups of hospitalizations. For example, hospitalizations for children ages 1-4, 5-9 and 10-14 for MHSA were more likely to be billed to Medicaid than hospitalizations for non-MHSA conditions (p<.05). Conclusions: MHSA conditions account for a large portion of hospital utilization for children, with over one-fifth of hospitalizations for children 10-17 YO being related to these conditions. Hospitalizations for MHSA conditions are longer than hospitalizations for other conditions. Comorbid MHSA conditions significantly increase the charges for hospital care. Hospitalizations for MHSA conditions for children 1-14 are more frequently billed to Medicaid than hospitalizations for other conditions. Implications for Policy, Delivery or Practice: These analyses reveal significant differences in hospitalization by expected payer, but further research is needed to determine if these differences are related to variations in prevalence, or need for care, versus variations in treatment setting, or system of care. Primary Funding Source: Agency for Healthcare Research and Quality (AHRQ) Call for Panels Quality Improvement in Medicaid: Using Research and Policy to Improve Preventive and Developmental Services for Your Children Chair: Melinda Abrams, M.A. Saturday, June 25 • 10:00 a.m. - 11:45 a.m. ● An Examination of Medicaid and SCHIP Coverage and Payment Policies Promoting Early Childhood Development Anne Markus, J.D., Ph.D., M.H.S., Sara Rosenbaum, J.D., Alexis Crumbley, J.D., Alexandra Stewart, J.D., Marisa Cox, M.A. Presented by: Anne Markus, J.D., Ph.D., M.H.S., Assistant Research Professor, School of Public Health and Health Sciences, Department of Health Policy, George Washington University, 2021 K Street, N.W., Washington, DC, DC 20006; Tel: (202) 530-2339; Fax: (202) 296-0025; E-mail: armarkus@gwu.edu Research Objective: Medicaid and SCHIP agencies play important roles in ensuring that children have access to quality care. Not only are they federally required to improve quality, but as the largest purchasers of health care for lowincome children, they possess the leverage needed to align coverage and payment policies to encourage adherence to professionally acceptable standards of care. Additionally, the implementation of HIPAA transaction standards in 2003, which required all payers to conform to nationally-recognized code sets, presents new opportunities and challenges for reforming state payment policies of early childhood preventive and developmental services to improve the quality of care for children. The research objectives are to (1) examine, within a HIPAA context, state coverage and payment policies of early childhood preventive and developmental services delivered in a primary care setting, and (2) compare these policies with (i) existing professional guidelines related to health care for young children and (ii) a typology of effective early childhood interventions grounded in the scientific literature. Study Design: Researchers used systematic documentary review to examine all 50 Medicaid and 35 separate SCHIP coverage and payment policies. Publicly-available state documents, including provider fee-for-service manuals, fee schedules, HIPAA crosswalks, managed care contracts, and other related documents were collected in 2004. The analysis focused on (i) coverage of assessment, intervention, education, and care coordination services promoting early childhood development and billable codes for each of these services, (ii) required or recommended standards of care, and (iii) general billing and payment requirements. Population Studied: State Medicaid and SCHIP programs. Principal Findings: (1) Even though states now use standardized code sets, state reimbursement policy remains extremely varied. (2) The majority of Medicaid fee-for-service programs clearly spell out coverage expectations of early childhood services, albeit with some variation in individual services covered, (3) The majority of Medicaid fee-for-service programs (n=41) have explicit payment policies for periodic comprehensive preventive visits that recognize almost uniformly the same billing codes; however, few programs specify other codes used for additional services provided in a primary care setting (e.g., developmental testing). (4) Medicaid programs are more specific than SCHIP programs in both their coverage and payment policies. (5) Both Medicaid and SCHIP managed care programs usually do not publicly list reimbursement codes. Conclusions: Preliminary findings suggest that a discrepancy exists between state promises of comprehensive preventive pediatric coverage in early childhood development and the services states actually reimburse. They also suggest that physicians may have to accept payment of the periodic visit as payment in full for all of the appropriate preventive and developmental services they are expected to furnish according to existing practice guidelines. Finally, they suggest that managed care may present a particular challenge in conveying coverage and payment expectations to plans and network providers. Implications for Policy, Delivery or Practice: HIPAA provides an opportunity to address payment policy reform for all payers, including Medicaid and SCHIP, to ensure actual availability of coverage at a professionally acceptable standard of care. This study provides the first step in understanding existing gaps in state payment policies and providing the knowledge base necessary to develop meaningful options for improvement. Primary Funding Source: CWF ● Using External Quality Review Organizations to Improve the Quality of Preventive and Developmental Services for Children Henry Ireys, Ph.D., Tara Krissik, M.P,P., James M. Verdier, J.D., Melissa Faux, B.A. Presented by: Henry Ireys, Ph.D., Senior Researcher, Mathematica Policy Research, 600 Maryland Avenue, S.W., Suite 550, Washington,DC 20024-2512; Tel: (202) 554-7536; Fax: (202) 863-1763; E-mail: hireys@mathematica-mpr.com Research Objective: Current federal regulations obligate states to assess the quality of services provided to Medicaid beneficiaries in managed care plans. State Medicaid agencies typically contract with external quality review organizations, EQROs, to review quality-of-care studies conducted by managed care plans and to implement quality-related studies focused on particular populations or services. Child health policymakers have registered interest in the extent to which states rely on EQROs to examine the quality of preventive and developmental services for Medicaid-enrolled children, but there has been no effort to gather systematic data on this topic. This research addressed the following questions: How many states have used or are planning to use EQROs to conduct studies of preventive and developmental services? When faced with many services for which quality-of-care studies are needed, what factors enhance the likelihood that states will examine this topic? What factors are shaping states’ capacity to conduct methodologically rigorous studies of these services? Study Design: This study used survey and qualitative methods. Of 51 surveys sent to state Medicaid directors (including the District of Columbia), 48 were returned (response rate of 94%) and 25 directors (49%) indicated they had commissioned EQRO work in this area. Of 25 states with completed work, 19 indicated that 32 EQRO reports had been completed. Of these 32 reports, 9 reports from 6 states included methodologically strong analyses. We developed case studies based on qualitative interviewing of staff in 5 states and conducted intensive reviews of 10 state RFPs and key federal regulations. Population Studied: State Medicaid agencies, selected EQROs, and selected managed care organizations. Principal Findings: In any one year, less than 10% of states use EQROs to conduct quality-of-care studies on preventive and developmental services for children in Medicaid; most studies are methodologically weak, but several examples demonstrate the potential impact of well-designed studies on quality improvement efforts. Two factors play critical roles in driving states to focus studies on preventive and developmental services: influential “champions” and attention-getting data demonstrating problems with these services. Current federal regulations are prompting states to expand research methods used in quality-of-care studies by adding analysis of claims and survey data to traditional chartreview methods. Conclusions: Improving the quality of preventive and developmental services for Medicaid-enrolled children requires a “champion” who can make a convincing case that this issue deserves attention in a state’s overall strategy for improving Medicaid services. A convincing case depends on methodologically strong data on gaps in the provision of preventive and developmental services, the cost of failure to provide them, or consumer demand for them. Staff in state Medicaid agencies need help in understanding how to apply contemporary research tools within a quality improvement framework. Implications for Policy, Delivery or Practice: Child health service researchers can offer assistance to state Medicaid agencies, managed care plans, and EQROs by helping to design methods for evaluating projects aimed at improving the quality of preventive and developmental services for Medicaid-enrolled children. These research designs could include newly-available measurement tools and policy-driven strategies for synthesizing findings from the analyses of administrative, claims, and survey data. Primary Funding Source: CWF ● Research’s Impact on Improving the Delivery of Developmental Services in Medicaid: Lessons Learned From Two State Collaboratives Neva Kaye, B.A. Presented by: Neva Kaye, B.A., Program Director, National Academy for State Health Policy, 50 Monument Square, Portland, ME 04101; Tel: (207) 874-6524; Fax: (207) 874-6527; E-mail: nkaye@nashp.org Research Objective: Enhance developmental services delivered to young children enrolled in Medicaid. Study Design: The National Academy for State Health Policy (NASHP), with funding the Commonwealth Fund, has managed two collaboratives witha total of eight states to improve the delivery of early childhood health and developmental services. Each state conducted an individual project with that goal. NASHP provided technical assistance to the state efforts and identified and disseminated lessons learned to a national audience. In each state research and evidence played an important role in project development, operation, and expansion. In this proposed presentation the current project director will review project experience to identify examples of the use of evidence in developing state health policies—and the factors that enabled the research to impact state policymaking. Population Studied: State Medicaid agencies in CA, IA, IL, MN, NC, UT, VT, and WA Principal Findings: 1. Medicaid is a key partner in improving the developmental services delivered to young children. Agencies can re-engineer the delivery of care through quality improvement, reimbursement and other strategies. Further, all Medicaid agencies studied relied, to some extent, on scientific evidence in policymaking. 2. The ABCD collaborative experience demonstrated that research and scientific evidence can play an important role in: identifying a need for policy change, developing and assessing an intervention, and evaluating whether the intervention should be continued or expanded. Two examples of specific policy changes made by states based on scientific evidence and/or their own research into an intervention’s effectiveness are: a) NC was interested in improving performance because research had shown that the majority of children who needed developmental services did not receive them. They selected a standardized screen and implemented an intervention designed to increase the number of children screened and referred. Data collected at the end of the pilot project showed significant improvement in performance and the screening guidelines and model has now been expanded statewide. b) Illinois submitted a state plan amendment to allow Medicaid providers to screen for maternal depression even in cases where the mother was not a Medicaid beneficiary. Scientific evidence about the impact of maternal depression on a young child’s development was instrumental to the justification of serving a mother under a benefit targeted to children. Conclusions: Research and evaluation can be valuable tools for state policymakers. But, state policymakers have little time to identify pertinent information and few resources for evaluation. Therefore it is critical that 1) Research be accessible—both in terms of identifying pertinent information and in being easy to understand; and 2) Measures that require minimal resources to produce be developed and tested. Implications for Policy, Delivery or Practice: Medicaid agencies can significantly influence the quality of health and developmental services provided to children and have great interest in basing polices on scientific evidence but, due to limited resources, they need assistance in translating research into practice. Primary Funding Source: CWF Call for Panels Using Medicaid Data to Optimize Child Health Policy Chair: Joseph Thompson, M.D., M.P.H. Saturday, June 25 • 11:45 a.m. - 1:45 p.m. ● Assessing the Potential Effect of Programmatic Changes in Medicaid and SCHIP on Children’s Uninsured Rates Matthew M. Davis, M.D., M.A.P.P., Rachel M. Quinn, M.P.P., M.P.H. Presented by: Matthew M. Davis, M.D., M.A.P.P, Assistant Professor, Child Health Evaluation and Research Unit, Division of General Pediatrics, University of Michigan, 300 NIB, 6D20, Ann Arbor, MI 48109-0456; Tel: (734) 614-3508; Fax: (734) 764-2599; Email: mattdav@med.umich.edu Research Objective: To estimate the potential effect on statelevel children’s uninsured rates of programmatic changes in Medicaid and SCHIP, adjusting for other state factors relevant to children’s insurance status. Study Design: We hypothesized that children’s uninsured rates at the state level are a function of sociodemographic and economic factors in combination with Medicaid and SCHIP programmatic decisions. The outcomes of interest were statelevel children’s uninsured rates for children overall and also for low-income children alone, based on data from the Current Population Survey (CPS) for the years 1999-2003 inclusive. We examined associations between uninsured rates and candidate concurrent state-level predictor variables; programmatic variables included income eligibility thresholds by age groups, asset tests, presumptive and continuous eligibility, type of SCHIP program and SCHIP implementation date, and premiums, copays, and enrollment fees for SCHIP. We analyzed these associations first in bivariate and then in multivariate time-series models. Given high collinearity between the Medicaid eligibility threshold variables within states, we ran separate models for eligibility thresholds for ages 0-1, 2-5, 6-16, and 17-19 years; mean coefficient values from these separate models are reported. All analyses controlled for state child population; models for all children also controlled for median income, and models for lowincome children controlled for type of SCHIP program. Population Studied: The US population, as characterized in CPS public use datasets. Principal Findings: All children – Higher SCHIP eligibility thresholds were associated with significantly lower uninsured rates (increase of 10 points in SCHIP thresholds associated with absolute decrease of .1% in the state uninsurance rate; P<.05). Higher state population proportions comprised by Hispanics were associated with significantly higher child uninsured rates (1% absolute increase in Hispanic proportion associated with .25% absolute increase in uninsured rate; P<.001), and higher proportions of state populations comprised by children were also associated with higher uninsured rate (1% absolute increase in child proportion associated with .35% absolute increase in uninsured rate; P<.001). Low-income children – The lack of a Medicaid asset test was strongly associated with lower uninsured rates (absolute decrease of 2.5%; P<.05). Higher Medicaid eligibility thresholds were associated with significantly lower uninsured rates (increase of 10 points in Medicaid thresholds associated with absolute decrease of .3% in uninsured rates; P<.05). Similar to patterns for children overall, among low-income children higher state proportions of Hispanics were associated with higher uninsured rates. Conclusions: Recent historical trends in uninsured rates underscore the critical role of Medicaid and SCHIP in providing insurance coverage to children. In addition, these analyses illustrate the potential benefits to states of improving outreach to their Hispanic populations, and to recognizing states’ limitations in providing coverage to disproportionately large populations of children. Implications for Policy, Delivery or Practice: This analysis may serve as a decision aid for policymakers considering potential effects of legislated changes in Medicaid and SCHIP eligibility thresholds for state child uninsured rates, and also suggests a rationale for adjustment of the federal matching rate to account for states with larger-than-average proportions of their populations comprised by children. Primary Funding Source: none ● Access to Specialty Care among Children with Chronic Conditions in Managed Care Elizabeth Shenkman, Ph.D., Lili Tian Ph.D., John Nackashi, M.D., Des Schatz, M.D. Presented by: Elizabeth A. Shenkman, Ph.D., Director, University of Florida, 1329 SW 16th Street, Room 5130, Gainesville, FL 32608; Tel: (352) 265-7220 x8633; Fax: (352) 265-7221; Email: eas@ichp.ufl.edu Research Objective: Access to specialty care for children with chronic conditions may be constrained within managed care environments. The purpose of our study was to examine the association between managed care organizational (MCO) characteristics and outpatient physician specialist use among children with chronic conditions who were 1) receiving care in MCOs where primary care providers (PCPs) serve as gatekeepers and 2) insured through a State Children’s Health Insurance Program (SCHIP) where all MCOs provided the same benefit package and co-payment structure but could use different strategies to deliver the children’s health care. None of the MCOs had financial penalties for specialty referrals. Study Design: Using person-level health care claims/encounter data and parent interview data, we identified 2,333 children with a chronic condition who had 1) functional limitations, 2) increased use of health care services, and/or 3) dependence on medications or equipment. Interviews were conducted with administrators of nine MCOs participating in SCHIP about MCO characteristics that might be associated with specialty care use including prior authorization procedures, the availability of PCPs who are pediatricians, PCP reimbursement, and the use of financial incentives to promote meeting pediatric quality of care standards. The odds of an outpatient physician specialist visit one year after study entry were examined as a function of child health and sociodemographic characteristics and prior specialty use, MCO characteristics, and provider availability in the MCO service delivery area. Population Studied: Children enrolled in Florida SCHIP in 2000. Principal Findings: Children cared for in MCOs 1) with lower percentages of PCPs paid fee-for-service (OR 0.60; 95% CI 0.43, 0.84), 2) with higher percentages of pediatricians in the PCP network (OR 1.17; 95% CI 1.07, 1.29), and 3) offering financial incentives for meeting quality of care standards (OR 1.71; 95% CI 1.28, 2.29), had higher odds of outpatient physician specialist visits. African-American children had odds of specialty care that were about one-half that of White children (p=0.005). Children with prior physician specialist use were 52% more likely to have a physician specialist visit in the year after study entry (p=0.005). Conclusions: A high percentage of pediatricians in the network, the use of fee-for-service, and financial incentives are associated with increased odds of specialty use. Implications for Policy, Delivery or Practice: PCPs paid on a capitated basis may be less willing to manage certain health problems when discretion exists regarding the necessity for a referral. Our findings suggest that blended payments combining elements of fee-for-service and capitation may be beneficial to promote access to care. Pediatricians may make more referrals due to their in-depth pediatric training and possibly greater awareness of potential complications when compared to family practitioners. Finally, the use of financial incentives focused on quality of care standards may foster an increased emphasis on meeting children’s health care needs, including the need for specialty referrals. Our study suggests that MCOs using these strategies may provide better specialty care access. However, further studies examining MCO characteristics and specialty care use in the context of specific clinical situations is needed. Primary Funding Source: Agency for Healthcare Research and Quality, and Health Resources and Services Administration ● Identifying Opportunities for Improvement in Pediatric Asthma Management Kevin J. Dombkowski, Dr.P.H., Lisa M. Cohn, M.S., Sarah J. Clark, M.P.H. Presented by: Kevin J. Dombkowski, Dr.P.H., Research Investigator, Child Health Evaluation and Research Unit Division of General Pediatrics, University of Michigan, 300 North Ingalls, Room 6C07, Ann Arbor, MI 48109; Tel: (734) 615-6758; Fax: (734) 764-2599; Email: kjd@med.umich.edu Research Objective: To assess opportunities for targeted interventions in pediatric asthma care for Medicaid beneficiaries by contrasting health plan performance within and between different geographic regions. Study Design: Retrospective analysis of administrative claims data for 18 state Medicaid health plans. The four main outcome measures were based on National Asthma Education and Prevention Program (NAEPP) recommendations for asthma management: annual outpatient visits; asthma emergency department (ED) visits; use of asthma controller medications; and influenza vaccination. Outcomes were contrasted within plan by geographic region. Population Studied: The study population was 3,970 children 5-18 years old with persistent asthma who were continuously enrolled in the same Michigan Medicaid health plan for 2002 and 2003, with no other source of health insurance. Principal Findings: Aggregate outcomes varied significantly (p • .05) between plans, e.g., the proportion of children with at least one long-term asthma controller prescription ranged from 66% to 88%, while the proportion of children with influenza vaccination ranged from 3% to 46%. Plan ranking varied depending upon the outcome measure used. Within plans, variations became evident when outcomes were stratified by geographic region. For example, the plan that was observed to have the lowest aggregate proportion of children with asthma controller prescriptions (66%) had regional proportions that ranged widely, from 44% to 72%. Another plan with an average proportion of asthma ED users (28%) had regional results that ranged from 9% to 39%. Some plans were observed to rank highly in one region and substantially lower in other regions; similar region-by-plan variation was found for each outcome measure. Conclusions: Asthma outcomes measures can be derived from administrative claims data to identify potential areas for quality improvement. Asthma management practices may vary for a given plan across geographic regions, and plan-level results within regions may reveal outcomes which differ substantially from statewide and regional averages. Assessment of multiple asthma outcomes measures may reveal health plan performance contrary to that suggested by a single measure. Health plans can identify opportunities for targeted intervention by assessing regional variations of asthma outcomes. Implications for Policy, Delivery or Practice: Aggregate assessments of Medicaid pediatric asthma management practices at the overall plan level may not be sufficient to identify opportunities for improvement. Profiles of plan performance that are sensitive to regional variations in plan characteristics may be particularly useful in isolating and prioritizing quality improvement opportunities. Medicaid plans can capitalize on this information to gauge the adequacy of existing provider networks in selected geographic areas and to target areas that would benefit most from more intensive intervention. Primary Funding Source: Michigan Department of Community Health ● Lack of Follow-up Testing Among Children with Elevated Screening Blood Lead Levels Alex R. Kemper, M.D., M.P.H., M.S., Lisa M. Cohn, M.S., Kathryn E. Fant, M.P.H., Kevin J. Dombkowski, Dr.P.H., Sharon R. Hudson, R.N., M.S.N., C.N.M. Presented by: Alex R. Kemper, M.D., M.P.H., M.S., Assistant Professor, University of Michigan, 300 North Ingalls, 6E08, Ann Arbor, MI 48109-0456; Tel: (734) 615-3508; Fax: (734) 764-2599; Email: kempera@med.umich.edu Research Objective: Children enrolled in Medicaid have a three-fold increased risk of lead poisoning. No data are available regarding the care that children with elevated blood lead levels receive. Follow-up testing after an abnormal screening blood lead level is a key component of lead poisoning prevention. Our objectives were to measure the proportion of children with elevated screening levels who have follow-up testing and to determine factors associated with such care. Study Design: We performed a retrospective observational cohort study. Population Studied: We included all Michigan Medicaidenrolled children <= 6 years who had an elevated blood lead level between January 1, 2002 and June 30, 2003 and who were continuously enrolled in Medicaid for the subsequent 6 months. Because we were interested in care for newly detected cases, we excluded children who had an elevated blood lead level in the previous 6 months. There were 3,682 children included in this analysis. Principal Findings Follow-up testing was received by 53.9% (95% Confidence Interval [CI]:52.2%-55.5%). In multivariate analysis adjusting for age, screening blood lead level results, and local health department catchment area, the relative risk of follow-up testing was lower for Hispanic or non-white children than non-Hispanic white children (0.91 [95% CI:0.87-0.94] vs. 1), for children living in urban compared to rural areas (0.92 [95% CI:0.89-0.99] vs. 1), and for children living in high compared to low lead risk areas (0.94 [95% CI:0.92-0.96] vs. 1). Among those who did not have followup testing, 58.6% (95% CI:56.3%-61.0%) had at least one medical encounter in the 6-month period following the elevated screening blood lead level, including for evaluation and management (39.3% [95% CI:36.9%-41.6%]) or preventive care (13.2% [95% CI:11.6%-14.8%]) visits. Conclusions: The rate of follow-up testing was low, and children with increased likelihood of lead poisoning were less likely to receive follow-up testing. At least half of the children had a missed opportunity for follow-up testing. Implications for Policy, Delivery or Practice: This is the first study to document the low rate of follow-up for children with elevated blood lead levels. Without follow-up, testing does not confer any benefit. New strategies are required to ensure optimal care. This study demonstrates the role of Medicaid administrative claims data in supporting the delivery of public health services. Primary Funding Source: Michigan Department of Community Health Call for Panels Caught in the Middle: Youth at the Intersection of the Mental Health and Juvenile Justice Systems Chair: Alison Cuellar, Ph.D. Saturday, June 25 • 11:45 a.m. - 1:15 p.m. ● How Do Youth with Emotional Disorders Fare in the Juvenile Justice System? Alison Cuellar, Ph.D., Pinka Chatterji, Ph.D. Presented by: Alison Cuellar, Ph.D., Assistant Professor, Health Policy & Management, Columbia University, 600 W. 168th Street, 6th Floor, New York, NY 10032; Tel: (646) 769-0542; E-mail: ac2068@columbia.edu Research Objective: Several studies have documented that youth with emotional and substance use disorders are overrepresented in the juvenile justice system. Whether the justice system is biased against these youth has been the subject of public policy concern, but there have been few systematic, empirical tests of this claim. Using data from a nationally representative sample of adolescents, this study assesses whether youth who use substances or have emotional disorders are sanctioned more heavily than other youth by the juvenile justice system, controlling for the youths’ crime and criminal history. Study Design: This study uses Wave III of the National Longitudinal Study of Adolescent Health (AddHealth) and offers several distinct advantages over existing research: First, it relies on data from a large, nationally representative sample of youth increasing the generalizability of the findings. Second, youth in the sample are first interviewed in the community rather than in institutions increasing the interpretability of the results and allowing us to address the question of bias in the juvenile justice system. Finally, AddHealth data allow for the inclusion of important control variables that are not present in previous studies. These variables include the nature of the delinquent act committed, delinquency history, emotional and substance abuse disorders, as well as demographic and community variables. This study uses multivariate regression where the unit of analysis is the individual. Key outcomes variables include the likelihood of being detained, the likelihood of conviction, the likelihood of community placement, and the likelihood of residential placement. The primary independent variable of interest is whether the youth has an emotional and/or substance abuse disorder. Other independent variables include whether youth was treated for an emotional disorder, demographic characteristics, family structure and living situation, local neighborhood and community characteristics, such as poverty, housing quality, and access to health care, charge at time of arrest, and history of delinquency. Population Studied: Add Health encompasses a nationally representative the sample of 15,197 youth living in the community who were interviewed in 2001/2002 Principal Findings: Early results of this study find evidence of bias in the justice system, particularly against youth with substance abuse and ADHD disorders. Conclusions: Results of this study have important implications for identifying a group of youth whose health needs are not being appropriately recognized and who face a greater likelihood of being punished as a result of their disorder. Implications for Policy, Delivery or Practice: If the justice system is biased, whether intentionally or not, against youth with emotional disorders then a concerted policy focus on changing the behaviors of key players in the justice and mental health systems is needed. Changes might include early access to mental health screening and treatment information for youth who become involved with the justice system; diversion of youth to appropriate treatment services rather than further court processing; or the development of more appropriate sanctions that include treatment components. Ultimately, this study has implications for outreach and education programs in the justice system, as well as the delivery system of public mental health services. Primary Funding Source: none, university grant ● Can Community Mental Health Services Reduce Juvenile Justice Involvement? E. Michael Foster, Ph.D., Damon Jones Presented by: E. Michael Foster, Ph.D., Professor, Health Policy & Administration, The Penn State University, 204 E. Calder Way, Suite 400, State College, PA 16801; Tel: (814) 865-1923; Fax: (866) 369-6737; E-mail: emfoster@psu.edu Research Objective: Using longitudinal data on a group of high-risk children and youth, examine the relationship between the use of mental health services and subsequent juvenile justice involvement. Study Design: The data for these analyses were collected as part of the Fast Track Project, a multi-cohort, multi-site longitudinal study of children who are at risk for emotional and/or behavioral problems. The project includes an intervention component designed to prevent long-term exacerbation of problems in children identified in kindergarten as “at risk” for such long-term problems; these individuals receiving such treatment are not included here. Rather, our focus is on subjects who were (a) screened into the high-risk comparison group, and (b) children not identified as at-risk, but recruited as part of a “normative” sample to allow for examination of outcomes in a representative group of youth. When analyzed with probability weights, the resulting sample from these combined groups is representative of children from low-SES neighborhoods in the four sites. Population Studied: The sample of 754 individuals are representative of children and youth living in four diverse areas—Nashville, TN; Seattle, WA, Durham, NC and rural Pennsylvania. Thirteen waves of data are available describing these youth’s experiences from kindergarten through the end of high school. Principal Findings: Since service use was determined by the families themselves (as one would expect in a community study), comparisons between youth who did and did not receive services need to be adjusted for any enabling, predisposing or need factors that otherwise will be confounded with the effect of service use. Initial analyses confirm this—simple comparisons between youth who do and do not use services suggest that services actually worsen mental health. However, we use propensity scores to adjust for differences between the two groups (involving key baseline characteristics, such parental education). Those adjustments reveal that mental health services have small benefits. In particular, these findings suggest that use of mental health services reduces the likelihood of subsequent juvenile justice involvement. Conclusions: The costs of mental health services may be partially offset by reductions in expenditures in other childserving sectors. Implications for Policy, Delivery or Practice: Blended funding may be a better way to deal with the needs of children with emotional and behavioral problems. Primary Funding Source: Other Govt, NIMH ● A National Assessment of Youth Involved with Child Welfare: Prevalence of Emotional, Behavioral and Substance Use Problems, Access to Specialty Treatment, and the Role of Court Involvement Anne Libby, Ph.D., Heather D. Orton, M.S., Richard P. Barth, Ph.D., William Jones, J.D., John Landsverk, Ph.D. Presented by: Anne Libby, Ph.D., Assistant Professor, University of Colorado at Denver and Health Sciences Center, School of Medicine, Nighthorse Campbell Native Health Building, P.O. Box 6508, Mail Stop F800, Aurora, CO 80045; Tel: (303) 724-1451; Fax: 303) 724-1474; E-mail: anne.libby@uchsc.edu Research Objective: Estimate the prevalence of emotional, behavioral and substance use problems for adolescents involved with child welfare, comparing in and out-of-home cases. Measure access to specialty mental health and substance abuse treatment, and the influence of court involvement on referrals to treatment over time. Study Design: Secondary data come from the National Study of Child and Adolescent Well-Being (NSCAW), a three-year longitudinal study of a nationally representative sample of youth, their parents and caretakers who came into contact with child welfare systems. Data include baseline, 18-month and 36-month follow-up about the need for emotional and substance abuse services and access to services, and court involvement during that time period and whether such services were mandated by the court. Youth and placement characteristics are available at each wave to compare youth with and without health insurance to assess the importance of court involvement for service receipt. Population Studied: Youth aged 11-14 at baseline who had come into contact with child welfare systems via an investigation of abuse or neglect. The complex sample and survey design is weighted to create nationally representative estimates of the U.S. population of children and adolescents involved with child welfare. Principal Findings: Nearly two-thirds of these youth were assessed as having emotional or behavioral problems, and nearly one-half with substance use problems. The majority (roughly 85%) remained in-home compared to out-of-home foster care cases. At 18 months, approximately 20% of youth had come into contact with the court for a behavior offense, and one-third of these were court-ordered to specialty mental health or substance abuse treatment. Service referral and utilization varies dramatically by type of need, health insurance and court contact. Conclusions: This study provides unique information about the relationships between multiple youth-serving systems and the role of the courts in getting access to emotional and substance use treatment. Implications for Policy, Delivery or Practice: These results highlight the importance of understanding the interactions between systems that come into contact with youth with emotional, behavioral or substance use problems. Opportunities for getting these youth into treatment before delinquency is a factor is critical, and points of intervention for prevention appear plentiful. Child welfare systems and specialty treatment systems, in collaboration with state and county administrators, can use this information to find ways to improve efficiency and reduce system and human costs by providing timely access to care with the goal of avoiding court involvement for these youth. Primary Funding Source: RWJF ● Experiences of Latino Juvenile Offenders in Seeking Behavioral Health Care Lisa Fortuna, M.D., M.P.H., Norah Mulvaney-Day, Ph.D, Helena Hansen, M.D., Ph.D. Presented by: Lisa Fortuna, M.D., M.P.H., Staff Psychiatrist, Center for Multicultural Mental Health Research, Cambridge Health Alliance, 120 Beacon Street, 4th Floor, Somerville, MA 02431; Tel: (617) 503-8485; Fax: (617) 503-8430; E-mail: lfortuna@charesearch.org Research Objective: This paper is about the perceptions of mental health services among a sample of young adult Latinos with a history of juvenile justice involvement and who are in the process of community reentry. While a variety of factors continue to produce mental health services inequalities for this population, this paper reports on an investigation which focuses on: 1) the mental health experiences of Latino young adult ex-offenders and attitudes towards care and help seeking and 2) how experiences of social support may relate to improved mental health services for these young adults. Study Design: We used a purposive sampling design at a community based agency. We completed in-depth interviews with Latino juvenile ex-offenders, community providers and families. We employed ethnographic methods including participatory observation at the community agency serving this population over a one year period. Population Studied: The study population consists of 20 young adult Latinos ages 18-26 years with a history of juvenile detention, variable levels of mental health services experiences and in the process of community reentry, living in the Boston, MA area of the United States. Principal Findings: We find that social exclusion and perceived irrelevance of mental health services to personal experiences comprise an explanatory framework which is repeatedly invoked by these youth in describing their interaction with the mental health and substance abuse services system. Experience and expectations of mistreatment, clinical stereotyping and coercion by mental health providers are key factors discouraging accessing mental health services for assessment and treatment, and thereby perpetuating mental health care inequalities. In contrast, young people assert that supportive and sustained relationships with adults in the community are essential, because they provide the basic relational context that is necessary for psychological well-being, healing, identity development and successful community inclusion. Narratives point to young people’s desires to work through their difficulties with the support of others who understand the process of community reentry, community life, and their trajectory as young Latinos who have faced difficulties, losses, isolation and disappointments. However, they also long to have support from those who see their potential and care about what they can contribute to community. Conclusions: We conclude that participation and partnership with the community are vital means by which to generate both the objective and subjective inclusion. These are requirements for accessible and appropriate mental health and substance abuse services for young Latino ex-offenders returning home. Healing and psychological development for these young people is fundamentally relational and necessarily occurs through continuous engagement and mutual participation with others. Implications for Policy, Delivery or Practice: These results have implications for improving therapeutic alliance and culturally appropriate treatment options for Latino juvenile exoffenders. With this information the mental health system can consider ways to integrate services in cooperation with culturally appropriate community based programs and improve entry and retention of Latino ex-offending youth in treatment. Primary Funding Source: Other Govt, NIMH Call for Panels Maximizing the Use of the New National Survey Data Sets Providing Information on Children and Youth with Special Health Care Needs Chair: Christina Bethell, Ph.D. Saturday, June 25 • 2:30 p.m. – 4:15 p.m. ● Comparing and Interpreting Findings on the Prevalence and Health and Health Care Service Need Characteristics of Children and Youth with Special Health Care Needs (CYSHCN) Across Three New National Data Sets Christina Bethell, Ph.D., M.P.H., M.B.A., Debra Read, M.P.H., Paul Newacheck Presented by: Christina Bethell, Ph.D., M.P.H., M.B.A., Director, Oregon Health and Science University, Mail Code CDRCP, 707 S.W. Gaines Road, Portland, OR 97239-2998; Tel: (503) 494-1892; Fax: (503) 494-2475; Email: bethellc@ohsu.edu Research Objective: To compare findings on the prevalence and health and health care service need characteristics of children and youth with special health care needs identified using the same screening method (CSHCN Screener) in the 2001 National Survey on Children with Special Health Care Needs (NS-CSHCN), the 2000 Medical Expenditures Panel Survey (MEPS) and the 2003-2004 National Survey on Children Health (NSCH). Study Design: Data from the NS-CSHCN, MEPS and NSCH are used to calculate the proportion of children meeting criteria for having one or more type of special health care need using the standardized CSHCN Screener. Child health and health care service needs as well as sociodemographic characteristics of CYSHCN are compared to further understand similarities and differences in the prevalence and profile of CYSHCN provided by each of these datasets. Several analyses consider whether differences observed may be due to variations across surveys in (1) sampling (random vs. over sampling; household vs. target child interview; English vs. Non-English language), (2) administration (survey introduction, order of items, incentives, survey length) and (3) weighting. Differences in shifts in practice patterns between survey years (2000 to 2004), such as increased use of prescription medication among children and higher rates of provider identification of children with mental or behavioral health problems (e.g. ADHD), are also considered. In addition, differences in characteristics of CYSHCN identified using alternative methods (CSHCN Screener vs. condition checklists) are also compared to further understand the overall performance of the non-condition specific, consequences-based CSHCN Screener across these three new national data sets. Comparisons are made to the historically used methods in the National Health Interview Survey. Population Studied: Children age 0-17 who met standardized parent-reported criteria for having a special health care need in the NS-CSHCN, MEPS and the NSCH. (N= 68,217). Principal Findings: The rate of CYSCHN in the NS-CSHCN is 13.6 (13.4-13.9) vs. 16.2 (14.7-17.7) for MEPS for English language cases (MEPS English only). Once identified, CYSHCN identified in each survey do not vary dramatically in the health and health care service need consequences they experience. We hypothesize higher rates of identification for the NSCH due to variations in sampling and administration of this survey compared to the NS-CSHCN and real shifts in practice patterns in recent years. Results from this hypothesis testing will be finalized when the NSCH becomes publicly available in March 2005. We also hypothesize that significantly fewer children will be identified using the CSHCN Screener vs. a chronic condition check-list in both MEPS and the NSCH and that these children experience more functioning and health service need consequences compared to children only identified using a condition check-list. Conclusions: Important differences in the profile of CSHCN provided across the new national data sets exist and involve differences in methodology as well as potentially real differences shifts in practice patterns and epidemiology of CSHCN between survey years. Implications for Policy, Delivery or Practice: Users of the new national data sets need to understand differences in methods used across surveys in order to validly interpret findings on CYSHCN emerging from the NS-CSHCN, MEPS and the soon to be released NSCH. Primary Funding Source: none ● Maximizing the Use of the New National Data Sets for Assessing Children and Youth with Special Health Care Needs: An Evaluation of Alternative Subgroups for Risk Adjustment Models Matthew Bramlett, Debra Read, M.P.H., Christina Bethell, Ph.D., M.P.H., M.B.A., Stephen Blumberg Presented by: Debra Read, M.P.H., Oregon Health and Science University, 3181 SW Sam Jackson Park Road, CB 669, Portland, OR 97201-3098; Tel: (206) 494-2555; Fax: (503) 494-4981; Email: readd@ohsu.edu Research Objective: To identify and test alternative models for discriminating among children with special health care needs (CSHCN) identified using the non-condition-specific CSHCN Screener. Study Design: Two alternative models for identifying subgroups of CSHCN identified in the NS-CSHCN and MEPS were developed to address different research and policy applications of these data sets. The Frequency Grouping model assigns CSHCN to subgroups based solely on the number of screening criteria met (1-5), whereas the Clinical Grouping model assigns CSHCN to one of four mutually exclusive subgroups: those whose conditions lead to ongoing functioning limitations, those whose conditions result primarily in a need for prescription medication, those whose conditions result primarily in an increased need for medical and community-based services, and those who require both services and prescription medications. The ability of these models to discriminate between groups of CSHCN was explored using the NS-CSHCN and MEPS data sets. Population Studied: Children age 0-17 years with special health care needs, as determined by the CSHCN Screener. The CSHCN Screener includes five questions on general health care needs that could be the consequence of chronic health conditions (e.g., need for special therapies, or need for prescription medications); along with follow-up questions to determine if the health care need is due to a chronic medical, behavioral, or other health condition. Principal Findings: Children’s health status, health care service needs, and medical expenditures vary dramatically across different robust sub-groupings of CSHCN for each of the models tested. The Clinical Grouping model is most discriminating for purposes of interpreting health care needs for clinically meaningful groups of CSHCN, such as those who require multiple medical and community based services or whose primary health need is related to emotional, developmental or behavioral issues only. The Frequency Grouping model discriminates among children with higher versus lower level of severity. Both models predict medical expenditures and may be particularly useful for purposes of risk adjustment in multivariate analyses. Conclusions: When CSHCN are considered as a homogenous population, many critical variations in health, health care service need, and healthcare system performance can be overlooked and can lead to erroneous conclusions and recommendations for policy and practice. Implications for Policy, Delivery or Practice: Users of the new national data sets need to understand differences in methods used across surveys in order to validly interpret findings on CYSHCN emerging from the NS-CSHCN, MEPS and the soon to be released NSCH. Primary Funding Source: none ● User-Friendly Strategies to Expand the use of New National Data Sets on Children's Health by Policymakers and Consumer and Health Care System Leaders Christina Bethell, Ph.D., M.P.H., M.B.A., Debra Read, M.P.H., Nora Wells Presented by: Nora Wells, Director, Federation For Children With Special Needs, 1135 Tremont Street, Suite 420, Boston, MA 02120-2140; Tel: (617) 236-7210; Fax: (617) 572-2094; Email: nwells@fcsn.org Research Objective: To develop and evaluate the use of an online data query tool to expand the use of the National Survey on Children with Special Health Care Needs (NSCSHCN)and the 2003-2004 National Survey on Children's Health among federal and state policymakers and program leaders and family and health care system leaders. Study Design: Federal and state policymakers and program administrators and family leaders across the US were engaged in a five phase process to assess interest, capacity and support needed to use data resulting from the NS-CSHCN and other similar data sets (n= 72 representing 36 states). Phases included (1) in-person focus groups, (2)a standardized self-reported survey, (3) in-depth structured interviews to identify preferred features and content for an online data query tool and resource center and (4) a workshop to further discuss needs and options for designing the Data Resource Center (DRC) and (5) an in-person website demonstration and evaluation session. Input obtained during ten in-person educational workshops on the DRC and the use of the DRC by over 12,000 users (65,000 hits) was evaluated to assess the usability and value of the DRC in expanding the use of national data sets by non-research audiences essential to engage in the use of data to inform and stimulate the design of health care programs and policies for children and youth. Population Studied: Federal and state Title V leaders in the area of children and youth with special health care needs (CYSHCN) and family CYSHCN leaders participating in the Family Voices consortium. (N = 72 for pretest; N = approx. 12,000 for beta test). Principal Findings: Over 85% of participants indicated that they were "extremely interested" in being able learn about and directly access and query national and state level child health and health care quality data sets. Over 83% indicated that they would be "extremely likely" to routinely use a Data Resource Center website designed to assist them in learning about and easily using this data. Over 60,000 hits to the DRC were recorded during the nine month start up period of the DRC. The vast majority of visits were to use the online interactive data query tool. Examples of uses of data findings derived from the DRC include grant applications, legislative testimony, popular press public education, stakeholder education and engagement and state block grant needs and performance assessments as well as many other applications. E-mail and telephone technical assistance are central to the success of any DRC-like effort as well as in-person and other more indepth trainings on how to think about, query and communicate data findings in a scientifically valid and effective manner. Conclusions: State and federal policymakers and health care program leaders as well as family/consumer leaders have a strong interest in being able to directly access and validly use data findings from national and state surveys on child and adolescent health and health care. Implications for Policy, Delivery or Practice: Without a DRC-like resource it is unlikely that essential policy, consumer and health system leaders will make use of the new national and state data on child and adolescent health and health care will. Design of any DRC-like resource must be developed with ongoing and in-depth input from target users. If US health care policy continues to emphasize consumer engagement it will be even more important to provide publicly available, nonproprietary DRC-like resources to assist consumers, policymakers and others to easily access data they would otherwise not have the skills, capacity or resources to use Primary Funding Source: HRSA ● Methods for Evaluating Within-State Variation Using the National Survey of Children with Special Health Care Needs Virginia Sharp, M.A. Presented by: Virginia Sharp, M.A., Senior Research Associate, Seattle Children's Hospital & Regional Medical Center, 1100 Olive Way, Suite 500, MPW5-2, Seattle, WA 98101; Tel: (206) 527-5709 x2; Fax: (206) 527-5705; Email: virginia.sharp@seattlechildrens.org Research Objective: The primary objectives of this research project were to (1) develop and test a methodology for identifying rural-urban differences in access to care for children and youth with special health care need (CYSHCN) using the National Survey of Children with Special Health Care Needs (NS-CSHCN), and (2) evaluate rural-urban differences in access to care for CYSHCN between two seemingly similar states, Oregon and Washington. Study Design: Zip code level Rural Urban Commuting Area (RUCA) codes were linked to zip code of residence recorded for all Washington and Oregon respondents to the NSCSHCN and grouped into four categories--urban, suburban, large town, small town/rural. These RUCA groupings were used to analyze variables related to access to care and unmet service needs in the NS-CSHCN. Population Studied: The population included all children identified as CYSHCN in the NS-CSHCN residing in Washington (n=746) and Oregon (n=745). CYSHCN were identified using the CSHCN Screener, a set of five multi-part questions that identify children as having special health care needs based on the consequences of their health condition, rather than a list of specific diagnoses. Principal Findings: The NS-CSHCN includes information on need for and receipt of 14 types of child services and 4 family support services. At the state level, Oregon and Washington look very similar, with no statistically significant differences between the states for any of these 36 variables. However, when the RUCA codes are used to disaggregate each state’s data, different patterns of access to care and unmet needs appear for the two states. For child services generally, in Oregon children living in suburban areas tend to be less likely to receive all needed routine preventive care, dental care and vision services; in Washington, children residing in large towns are more likely to have unmet needs, especially for dental care, specialized therapies, mental health care, and vision services. These same patterns also hold true for family services. In Oregon, suburban families have more unmet needs, while in Washington, families living in large towns have more unmet family service needs. Comparing RUCA categories across the two states uncovers additional interesting differences in CYSHCN care needs and patterns of care. Conclusions: Even though Oregon and Washington are generally perceived to be very similar socially, politically, geographically and in other ways, they are not similar in terms of rural-urban disparities in access to care for CYSHCN. While the state sample sizes in the NS-CSHCN were too small to produce statistically significant differences for most access to care variables, those rural-urban disparities that were significant exhibited distinctly different patterns in the two states. Implications for Policy, Delivery or Practice: This analysis highlights the need for more research on both intra- and interstate patterns of health care resource distribution. Primary Funding Source: none Call for Panels Providing Continuity of Coverage to Low-Income Children: Policy and Program Impacts Chair: Susan Haber, Sc.D. Saturday, June 25 • 2:30 p.m. – 4:15 p.m. ● What Happens to Children Who Lose Coverage from SCHIP or Premium Assistance Programs? Janet B. Mitchell, Ph.D., Susan G. Haber, Sc..D., Sonja Hoover, M.P.P. Presented by: Janet B. Mitchell, Ph.D., Director, Division for Health Services and Social Policy Research, RTI International, 411 Waverley Oaks Road, Suite 330, Waltham, MA 02452; Tel: (781) 788-8100 x 135; Fax: (781) 788-8101; E-mail: jmitchell@rti.org Research Objective: Evaluate health insurance coverage and access to care for low-income children who have disenrolled from Oregon’s SCHIP and premium assistance programs, and compare differences between the two programs. Income eligibility requirements are identical for these two state programs (170% of FPL or less). Study Design: Telephone interviews were conducted in 2002 with the parents of children who had recently disenrolled from Oregon’s SCHIP and the state’s premium assistance program. Population Studied: Children who have recently disenrolled from Oregon’s SCHIP program or the state’s premium assistance program (n=505). Children transitioning to Medicaid were excluded. Principal Findings: The most common reasons for loss of coverage was that parents no longer met, or believed they would no longer meet, the income eligibility requirements. While almost all children (85%) had at least one parent who worked, few had access to employer-sponsored insurance. The majority of children were uninsured at the time of the interview, with SCHIP children significantly more likely to be uninsured than those who had received premium assistance (67% vs 47%). Uninsured children were more likely to have lost their usual source of care, to have not seen a physician since disenrolling, and to report unmet need for care. Controlling for demographics and health status, there were no differences between SCHIP and premium assistance disenrollees in usual source of care, physician visits, or unmet need; whether the child was currently insured was the most important predictor. Conclusions: SCHIP and other public programs for low income children were intended to serve as a bridge between Medicaid and private health insurance, particularly as parents moved into the workforce. Prior studies have documented high rates of disenrollment from these programs, but little has been known about outcomes for these children. This study shows that many of these children have become uninsured. Although their families’ incomes have increased, they are still unable to afford insurance. With the loss of coverage, these children also lose their attachment to a usual source of care and access to physician services. Implications for Policy, Delivery or Practice: SCHIP provides health insurance coverage to children whose family incomes are too high for Medicaid. Given the high cost of premiums and lack of access to employer-sponsored insurance for many working families, however, SCHIP and other program income eligibility ceilings may be too low. Policymakers may want to consider either raising the limits or introducing a graduated premium assistance program (e.g., where the size of the premium subsidy declines as income rises). Primary Funding Source: AHRQ, David and Lucile Packard Foundation, HRSA ● Dynamics of Children’s Enrollment in Public Health Insurance: A Three-State Comparison Susan G. Haber, Sc.D., Andrew Allison, Ph.D., Elizabeth Shenkman, Ph.D. Presented by: Susan G. Haber, Sc.D., Senior Economist, Division for Health Services and Social Policy Research, RTI International, 411 Waverley Oaks Road, Suite 330, Waltham, MA 02452; Tel: (781) 788-8100 x 152; Fax: (781) 788-8101; E-mail: shaber@rti.org Research Objective: Although Medicaid and SCHIP can be viewed as complementary programs as families’ incomes fluctuate, few studies have looked at enrollment in public health insurance (PHI) generally. Previous studies have mainly looked at Medicaid and SCHIP separately and have found that many children receive only episodic coverage through these programs. We examine children’s patterns of coverage in PHI to understand the relationship between SCHIP and Medicaid, and to compare children’s coverage based on type of eligibility (SCHIP, TANF, and poverty-level Medicaid). Study Design: We linked SCHIP and Medicaid eligibility records for children in Kansas, Oregon, and Texas to create complete records of enrollment in PHI. Transitions between different types of eligibility, as well as patterns of enrollment in and disenrollment from PHI, are analyzed using descriptive and multivariate methods. Population Studied: Children in Kansas, Oregon, and Texas enrolled in SCHIP or in Medicaid through TANF or povertylevel eligibility during the first 3-4 years of SCHIP operation. Principal Findings: A large proportion of SCHIP children in Kansas and Oregon move directly between SCHIP and Medicaid eligibility. One-third of SCHIP children in Kansas and two-fifths in Oregon move directly into Medicaid when they leave SCHIP. Although only 11% of SCHIP children in Texas move immediately into Medicaid when they disenroll, a large proportion re-joins PHI after a 1-3 month break in coverage. Most children in all three states are continuously covered by PHI for relatively brief periods of time. Less than 60% of the children in Kansas and less than half in Oregon were still covered by some type of PHI 12 months after their initial enrollment. In Texas, less than 30% of Medicaid children and 55% of SCHIP children still had PHI after 12 months. However, children in Texas are far more likely than those in Oregon and Kansas to re-enroll after a brief lapse in eligibility. Within a year after their initial enrollment, 49% of TANF children and 38% of poverty-level Medicaid children in Texas have disenrolled from PHI and subsequently reenrolled, compared to 15% or less of the children in Oregon and Kansas. Conclusions: There are considerable differences in continuity of PHI coverage among the states in our study, which may be related to administrative procedures. Unlike the free-standing programs in Texas and Kansas, Oregon’s SCHIP is fully integrated with Medicaid. This likely explains the high rate of transition between programs in Oregon. The large numbers of children in Texas who re-enroll in PHI after a brief break in eligibility suggests that children may be disenrolled for administrative reasons rather than true changes in eligibility status. Implications for Policy, Delivery or Practice: Policymakers need to understand the extent to which SCHIP operates as a complement to Medicaid, both to accurately assess the continuity of PHI coverage provided to low-income children and to design appropriate policies to educate families and coordinate coverage as they move between programs and across eligibility categories. Further work is needed to understand the impact of brief disruptions in eligibility on continuity of coverage. Primary Funding Source: Other Foundation, David and Lucile Packard Foundation ● Increased Family Cost-Sharing in SCHIP: How Much Can Families Afford? Elizabeth Shenkman, Ph.D., Bruce Vogel, Ph.D. Presented by: Elizabeth Shenkman, Ph.D., Professor, Department of Epidemiology and Health Policy Research and the Institute for Child Health Policy, University of Florida, 1329 SW 16th Street, Room 5130, Gainesville, FL 32608; Tel: (352) 265-7220, ext. 86333; Fax: (352) 265-7221; E-mail: eas@ichp.ufl.edu Research Objective: In July 2003, Florida increased the premium for families from $15 per-family-per-month to $20 per-family-per-month for those receiving subsidized premiums. The Centers for Medicare and Medicaid Services later determined that $20 per-family-per-month exceeded federal cost-sharing limits (5% of family income) for some families at or below 150% of the federal poverty level (FPL). In October 2003, Florida reduced the premiums to $15 for those at or below 150% FPL and kept the premiums at $20 for those above 150% FPL. During the 2005 session, the Florida Legislature will consider increasing premiums up to 4% of the family income effective July 1, 2005. The purpose of our analyses were to examine the impact of the 2003 premium increases on children’s disenrollment and to use this information to estimate the potential impact of the proposed premium increases on families. Study Design: We used SCHIP enrollment files and health care claims/encounter data provided by the state for 2000 through 2004. The Clinical Risk Groups (CRGs) were used to classify children into health status categories using diagnostic information found in the claims/encounter data. Cox proportional hazards models were used to estimate the responsiveness of disenrollment to premium changes, age, sex, income, CRG, and months enrolled. Population Studied: Children in the Healthy Kids Program, the largest SCHIP program component in Florida Principal Findings: Prior to the premium increases, about 2% of the children disenrolled from the program monthly. Disenrollment increased after the July 2003 premium change to 3.6% in August 2003 and to 4.7% of the children in September 2003. When the premiums were reduced, a decline in disenrollment was observed. Families with incomes at or below 150% FPL were 36% more likely to disenroll in the post-premium change period when compared to the prepremium change period. Families in rural areas were 6% more likely to disenroll post the premium change than families in urban areas, even after considering the children’s health status and family income. Children with significant acute or chronic conditions were 8% to 17% less likely to disenroll compared to healthy children. Using this information we estimated a price elasticity for the disenrollment hazard rate of 2.2, indicating that disenrollment from SCHIP is very sensitive to price changes. For example, given this price elasticity, a 10% increase in the monthly premium would produce a 22% increase in the disenrollment hazard rate, Similarly, an increase in the premium from $15 per month to $20 per month (a 33% increase), would increase the disenrollment hazard rate by approximately 73%., or from a baseline hazard rate of 1.4% to 2.4%. Conclusions: Small premium increases are likely to have a large impact on disenrollment. The impacts are greater for healthy children, lower-income children, and children residing in rural areas. Implications for Policy, Delivery or Practice: States need to consider premium increases carefully and the impact these increases can have on the lowest income families and those residing in rural areas. Moreover, premium increases can contribute to increased disenrollment among healthy children, which may result in adverse retention in SCHIP. Primary Funding Source: Other Foundation, The Healthy Kids Corporation ● The Impact of Premium Increases in SCHIP Programs: The Experience of Three States Genevieve M. Kenney, Ph.D., Andrew Allison, Ph.D., Julia Costich, Ph.D., J.D., Jim Marton, Ph.D., Josh McFeeters, M.P.P. Presented by: Genevieve M. Kenney, Ph.D., Principal Research Associate, The Urban Institute, 2100 M Street, N.W., Washington, DC 20037; Tel: (202) 261-5668; Fax: (202) 223-1149; E-mail: jkenney@ui.urban.org Research Objective: States increasingly have used premiums as a cost containment tool in SCHIP programs in recent years. In 2003 alone, 13 states raised the premiums in their SCHIP programs. While SCHIP premiums have varied substantially both across states and over time, very little is known about how premiums affect enrollment among children. In this paper, we analyze the impacts of SCHIP premium changes on enrollment in three different states—Kansas, Kentucky, and New Hampshire that increased premiums in 2003 to gain insights about how enrollment responses vary across states and with the size of the premium increase. Study Design: The primary data source for this analysis is state enrollment files for Medicaid and SCHIP. These files contain information on the child’s age, race, eligibility category, and residential location. We assess enrollment patterns during the period prior to the premium hike and the period following the premium hike. We analyze changes following the increases in premiums that were introduced in 2003, in monthly enrollment, new enrollment, and disenrollment. We assess the extent to which disenrollment due to premium non-payment appears to increase following the premium hike, and we examine whether the premium changes have spillover effects on enrollment in Medicaid or in non-premium paying categories under SCHIP. Population Studied: The population studied includes children ages 0 to 18 enrolled in Medicaid or SCHIP in Kansas, Kentucky, and New Hampshire in the period prior to and following the premium increases in 2003. Principal Findings: Our preliminary analysis indicates that premium increases may have had negative enrollment effects in all three states. Enrollment declined in the premium-paying category in Kentucky by about 19 percent following the imposition of the new $20 per family premium. Enrollment in that category remained at the lower level until the end of the study period, nine months after the premium was implemented. Total enrollment in SCHIP and Medicaid declined between December 2003 and January 2004 and did not rise back above the December 2003 level until March 2004. Transfers between SCHIP and Medicaid enrollment increased slightly after of SCHIP premium hike, but it is unclear if the premium hike in SCHIP was the cause. Initial analysis of the data from New Hampshire indicates that enrollment in the SCHIP program declined by about four percent after the implementation of the $5 per child premium increase. The $20 to $30 premium increase for Kansas SCHIP families in January 2003 coincided with a small drop in the total SCHIP caseload, which began in February and lasted approximately three months. Caseload growth, which had been nearly continuous since SCHIP implementation in 1999, did not resume until approximately 10 months following the increase in premiums. Conclusions: This study indicates that premium increases reduce enrollment in public health insurance programs. Reduced enrollment growth or declines in enrollment can persist for several months after a premium increase. Future work will address the consequences of premium increases on overall coverage levels. Implications for Policy, Delivery or Practice: This research can help policymakers assess the impact on program enrollment of increasing premiums in public health insurance programs. Primary Funding Source: Other Foundation, The David and Lucile Packard Foundation

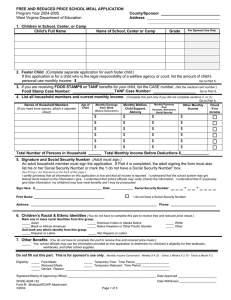

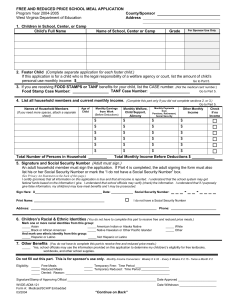
![[Product Name] Marketing Plan](http://s2.studylib.net/store/data/010126237_1-af5d431ac4bf7947710a4d07fade2aac-300x300.png)