September 2015
advertisement

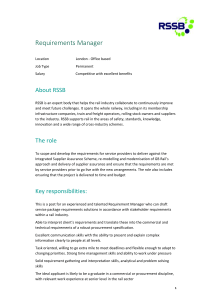
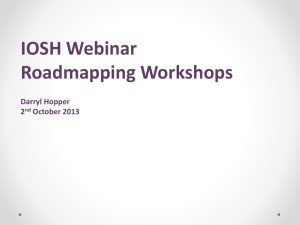
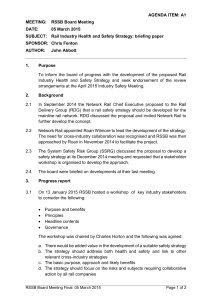
September 2015 This is a collation of some of the world’s railway formal inquiry reports. It includes a brief incident synopsis, along with the main causes and recommendations from each investigation. Readers may find some of the actions and recommendations useful to their own operations. Co-ordinated by Greg Morse, Operational Feedback Specialist, RSSB Contents: (Click to navigate) Australia: SPAD at Warnervale, New South Wales, 24 November 2014 Australia: Freight train derailment at Nambucca Heads, NSW, 14 May 2014 UK: Collision between a train and a collapsed signal post at Newbury, 17 November 2014 UK: Freight train derailment at Heworth, 23 October 2014 Australia: Level crossing collision at Woodvale, Victoria, 19 December 2014 Newbury Some of the key issues raised and/or suggested by the stories in this edition: SPAD Worksite protection Signaller handover Distraction Situational awareness Wagon loading Track twist Deficient guidance Signal maintenance and monitoring Track maintenance (cyclic top) Wagon maintenance User behaviour Sighting at crossings (vegetation) Produced by RSSB Author: Dr Greg Morse Email address: Greg.Morse@rssb.co.uk 16 September Australia: SPAD at Warnervale, New South Wales, 24 November 2014 For the full report, click here: LINK At 11:59 (local time) on 24 November 2014, a freight train passed 66.8 signal (between Wyee and Warnervale) at danger without authority. The SPAD was a breach of the Network Rules and Procedures involving the use of Absolute Signal Blocking (ASB) that had been granted as part of worksite protection arrangements for a workgroup conducting electrical maintenance tasks at Warnervale. The Protection Officer (PO) for the workgroup was granted ASB shortly after a change in the Network Control Officers (NCO) at Morisset, from where the signals protecting the section were controlled. Although assurances were given to the PO that the section was clear, two trains were still travelling between the protecting signals and the worksite at the time ASB was implemented. The first passed the worksite shortly afterwards without incident. The second, travelling some eight minutes behind, came to a stand approximately 1,300 metres before the worksite after the driver reacted to a signal returning to danger in front of the train. The signal had returned to danger because of electrical testing being conducted as part of the maintenance tasks. Its return also (fortuitously) prevented the train from entering the worksite and potentially injuring the track workers on duty. The Australian Transport Safety Bureau (ATSB) found that, when the NCOs changed over at Morisset, a breakdown in the handover process occurred, caused partly by the arrival of police officers trying to obtain information about an unrelated incident that had occurred two nights before. This resulted in ASB being granted to the PO at Warnervale without the exact location of trains being established, signals V8 and V6 being set back to stop and blocking facilities applied in accordance with the rules. At the time of the incident, Sydney Trains was trialling a modified ASB methodology to address previously identified safety issues, however trial had not been extended to Morisset. If it had been, the progress in granting ASB would have been documented and would have assisted the NCOs during the handover process. Additional interim arrangements for ASB were not implemented at the time of the incident as the requirements listed in the memorandum of July 2013 had not been promulgated to all staff. The ATSB notes that the incident illustrates the criticality of minimising interruptions and distractions that may affect the process for the granting or authorisation of work on track authorities, particularly Absolute Signal Blocking. Similarly, it reinforces the importance of information and situational awareness exchange between personnel during the handover process for the control of dynamic rail network operations. Action taken Sydney Trains advised that it has expanded its trial of the ‘Coded Authorisation Process for Absolute Signal Blocking’ to include signal box locations on the Main North Line between Gosford and Broadmeadow. It further advised that, on completion of the trial, the Network Rule and Procedure for Absolute Signal Blocking will be rewritten to improve its readability and application. Produced by RSSB Author: Dr Greg Morse Email address: Greg.Morse@rssb.co.uk Recommendations Sydney Trains should take further action to expedite the implementation of safeguards and procedural safety enhancements where Absolute Signal Blocking is to be used for worksite protection. Back to top 23 September Australia: Freight train derailment at Nambucca Heads, NSW, 14 May 2014 For the full report, click here: LINK At around 14:04 (local time) on 14 May 2014, the fourth wagon from the end of a Pacific National (PN) freight derailed whilst exiting a loop at Nambucca Heads. The train travelled a further 1,397 metres before the derailed vehicle tipped on its side, causing the consist to separate and subsequently stop. The ATSB found that the load had probably shifted, mostly to the left in the direction of travel. This would have transferred vertical forces from the wagon’s right side-bearer to the left side-bearer, causing the right-hand wheels to unload. At the point of derailment, the track geometry was transitioning out of a left-hand curve, which had a relatively high superelevation with respect to the actual speed of the train (about 21 km/h). The relatively high superelevation and subsequent twist as the superelevation ramped down through the transition, likely resulted in additional transfer of vertical force from the wagon’s right side-bearer to the left side-bearer, resulting in a further unloading of the right-hand wheels. The combination of superelevation, twist and (more importantly) uneven lateral loading, combined to unload the right-hand wheels which, when steering through a left-hand curve, resulted in flange climb and derailment of the wagon. Furthermore, the Pacific National Freight Loading Manual (FLM), and the application of it, was ineffective at preventing load shift in this case. Action taken PN has engaged a consultant to conduct an audit of its procedures and operational processes relating to the development and implementation of the FLM, specifically performing a gap analysis in relation to current steel loading processes. In addition, PN will be arranging an external engineering group to undertake a twist test and/or computer simulation modelling of an RCOF wagon to record its wheel loading performance Produced by RSSB Author: Dr Greg Morse Email address: Greg.Morse@rssb.co.uk characteristics during scenarios based on the data. The final report will contain recommendations that can be utilised to further refine its FLM and associated procedures and loading practices. The ATSB acknowledges that PN has initiated a review of its FLM and has taken action to ensure freight is loaded in accordance with established procedures prior to departure. However, it draws attention to a fundamental requirement of freight loading, in that it is essential that the load be prevented from moving in any direction relative to the wagon, as a shifting load at any point during transit is an undesirable condition that can affect the dynamic behaviour and safety of the vehicle. While PN’s action serves to ensure freight is loaded in accordance with the FLM on starting its journey, no action has been proposed to specifically address the demonstrated potential for shifting and movement of the rod-in-coil product while in-transit. Accordingly therefore, the ATSB issues the following safety recommendation. Recommendation Pacific National should undertake further work to address the possibility that rod-in-coil product could shift during transit, thereby creating an undesirable condition that could affect the dynamic behaviour of the vehicle. Safety message The ability for a load to shift during transit is an undesirable condition that can affect the dynamic behaviour of the rail vehicle. All rail freight operators should consider the safety implications of shifting/moving loads and should ensure that all loads are restrained and/or enclosed in such a way that prevents movement in any direction relative to the wagon. Back to top 23 September UK: Collision between a train and a collapsed signal post at Newbury, 17 November 2014 For the full report, click here: LINK At about 14:35 on 17 November 2014, a passenger train travelling at 110 mph struck the top of a signal which had collapsed and fallen across the line near Newbury. The signal post completely obstructed one track and partially obstructed a second (the one on which the train was travelling). There were no injuries and the train did not derail, but it did sustain some exterior damage. The outcome could have been much more serious if the first train to encounter the signal had been travelling at speed on the line that the signal had completely obstructed. The signal collapsed because the base of the post, which was of hollow tubular steel construction, had corroded through, causing an almost complete loss of wall thickness at and just above ground level. Corrosion had occurred to both internal and external surfaces: internally because water had entered the post and there was no drainage for it to escape, while the external corrosion was affected by the base being buried in ballast, which held water around the base and damaged the protective coating on the signal post. Signal posts are subject to annual visual examinations, but the examinations of this signal did not detect the problem because the main area of corrosion was hidden by ballast, and the examinations regime was vulnerable to missing such defects. A separate examination in 2012 for a resignalling Produced by RSSB Author: Dr Greg Morse Email address: Greg.Morse@rssb.co.uk project in the area also did not detect the defect for similar reasons. Because the defect was not detected, it was not subsequently reported and remedied through maintenance. The investigation identified possible underlying factors associated with the management of ballast levels around post bases, competence management of structures examiners and corporate knowledge about the original design specifications for signal structures. Although not linked to the accident on 17 November 2014, RAIB observes that, as well as the risk from train accidents, there had been a potential risk to anyone climbing or working on the signal. RAIB has identified the following learning point: Those involved in managing and undertaking the Line of Route examinations of ancillary structures are reminded that the actual examination process for each structure is no different from that for ordinary visual examinations. While the reporting format is abbreviated, the examination itself is not. Action taken The ORR served an Improvement Notice on Network Rail (Western route) on 5 December 2014, which required it to examine all the straight signal posts on the route and amend its examinations process. The Improvement Notice had a deadline of 1 June 2015, but this was subsequently extended to 1 October 2015 in light of the need to consider internal corrosion, as identified in the corrosion analysis commissioned by RAIB. The ORR is also pursuing the issue of internal corrosion at a national level with Network Rail. Network Rail (Western route) responded to the accident with the following actions: As an immediate response, local inspections had been carried out on 35 signal posts in the Newbury area by the end of November 2014. Nine were found to have their bases buried by ballast, of which two showed signs of corrosion. A wider exercise involving closer examination of all 1,754 straight signal posts on the route was implemented, including multiple photographs of the structures and bases. The purpose was to determine whether the bases of these structures were buried by ballast and, if so, to assess the condition of the base. At the same time, ballast boards would be installed where necessary. As of 30 July 2015, 1,704 signal posts have been examined while an additional 13 were not inspected as they were recently installed. A proportion of these revealed the need for supplementary examination and/or minor works – for the Swindon maintenance delivery unit, this amounted to 85 out of 404 structures requiring some level of ballast removal (as at 7 September 2015). In total across the route, 407 structures need to be revisited (as at 30 July 2015) and one signal post required follow up action to ensure its structural integrity. Network Rail (Western route) has also commissioned a retrofit design to strengthen any weak assets. At a national level, Network Rail has reported the following actions: A briefing note about the accident was issued on 23 December 2014, which included a number of recommendations for action at both route and central (ie national) level. These actions covered a review of all straight signal posts to confirm the condition of hidden components followed by risk-based remedial actions where necessary, processes for managing the effects of track work on structures, and a review of management controls for ancillary structures. As of 30 July 2015, all of the central actions had been completed and most of the route actions were either complete or on target to be completed by their nominal deadline. Where these Produced by RSSB Author: Dr Greg Morse Email address: Greg.Morse@rssb.co.uk actions have not yet been completed, Network Rail has reported difficulties in gaining track access as the reason and completion dates have been rescheduled. A workshop was held on 29 January 2015 to understand the limitations of the existing examination process. The workshop produced a high-level failure analysis of various forms of structure, which then fed into the development of a new examination methodology and report form for all ancillary assets that currently only receive visual examinations. At the time of writing, this methodology is still in development. In addition, Amey has: Issued a technical brief (December 2014), offering guidance on examining the interface between post and ground, positively reporting its condition and any parts not examined, and removing ballast. Briefed examiners that Line of Route reports should include a clear statement of where the structure was examined from and whether there were any parts not examined. Changed its method of examining and reporting information on straight signal posts, by providing more photographs and including parts not examined on the examination form, as well as restricting examinations to cover only those where the structure can be directly approached. Recommendations Network Rail should review its asset management strategy with the objective of improving the examination and maintenance of its ancillary structures. The review should consider: o Identification of structures at greatest risk of failure (eg by age of the structure, those of hollow section, those without galvanised or otherwise treated surfaces, those in hostile environments) and the possible consequences of failure in the context of wider safety risks to the railway; o Steps to mitigate the risk (such as periodic replacement); and o Specific measures to deal with planted posts as well as those structures fixed to foundations. Network Rail should develop and implement a risk assessment process to determine when it is necessary for the critical elements of ancillary structures to be exposed for the purposes of examination and/or to mitigate the risk of corrosion. The process should take into account the specific risk of corrosion of buried metalwork on hollow section ancillary structures that are fixed to foundations. Taking account of the emerging findings from the implementation of Recommendation 1, Network Rail should review its examination and maintenance regimes for ancillary structures and make any necessary improvements to ensure that its processes are commensurate with the risk arising from the failure of those structures. The review should include, but not be limited to, consideration of the following areas: o A regime of periodic enhanced examinations for ancillary structures (such as the Detailed Examination regime applied to bridges and other complex structures); o Consideration of the special requirements for examination of the buried elements of planted posts; o A means for assessing the internal condition of hollow section structures as well as their external condition; Produced by RSSB Author: Dr Greg Morse Email address: Greg.Morse@rssb.co.uk o Re-designing the examination forms (whether electronic or paper versions) to improve usability for the examiners, to clarify the need to report hidden critical elements that were not examined and to improve reporting lines between Network Rail and its examinations contractors; o Revising the competence standards for staff involved in the examination of structures to ensure consistency in the level of training received both by those who are new to the industry as well as experienced examiners; and o Cyclical maintenance of any surface treatments on ancillary structures. Changes made as a result of the review should be re-briefed to all those involved in structures examinations and relevant company standards and other documents should be updated as appropriate. Without waiting for Network Rail’s actions in response to Recommendation 3 above, Amey should immediately review and revise its competence management processes for its staff involved in structures examinations in accordance with the findings from this investigation. The revised processes should allow for further adjustments to be made as necessary once Network Rail has completed its response to recommendation 3. Back to top 24 September UK: Freight train derailment at Heworth, 23 October 2014 For the full report, click here: LINK At about 15:25 on 23 October 2014, a freight train derailed just after passing through Heworth station. It was travelling at 51 mph when the leading wheelset of the tenth wagon derailed on track with cyclic top.1 The train continued for about 1.4 miles, where it was stopped by the signaller, who had become aware of a possible problem with the train from damage to the signalling system. By the time the train stopped, all of the wagon’s wheels had derailed and its suspension had been damaged. RAIB found the immediate cause of the accident to be a combination of a loss of damping within the suspension on one corner of the wagon that made it susceptible to derailing on the cyclic top track defect it passed over. This was because: The wagon had a worn suspension component that made its leading left-hand wheel susceptible to unloading and lifting up when responding to dips in the track. The wagon’s maintenance regime had not identified this worn component. The excessive wear was most likely due to misalignment of the wheelset within its suspension. The severity of the dips in the track required Network Rail to impose an emergency speed restriction, but no such restriction had been put in place. 1 That is, regularly spaced dips in both rails. Produced by RSSB Author: Dr Greg Morse Email address: Greg.Morse@rssb.co.uk The cyclic top defect formed due to water in the track not draining away and although the track inspection regime had identified this defect many times, often no repair took place. Occasionally the local Network Rail track maintenance team carried out manual repairs but these were ineffective. The local Network Rail track maintenance team was unable to cope with the volume of work it had to do. This was due to insufficient numbers of track maintenance staff over a long period of time, changes to the arrangements for working safely while on the track, restrictions on gaining access to the track and changes to how the track was inspected. Network Rail’s management arrangements did not identify the extent of non-compliances to its maintenance processes, or take earlier action to resolve the persistent problems that were affecting track maintenance in this area. RAIB has identified the following key learning point, which was also included in its report on the derailment near Gloucester that occurred on 15 October 2013: Network Rail should remind its staff responsible for managing the maintenance of its track (such as Track Maintenance Engineers and Track Section Managers) of the requirements in Network Rail standard NR/L2/TRK/001/mod11 relating to the imposition of a speed restriction due to persistent poor track quality: o If the vertical track geometry of an eighth of a mile long section of track is recorded in the maximum band (ie its SD value places it in the super- red category) and the remedial work undertaken is not sufficient to move the SD value out of the maximum band, then a speed restriction must be imposed. o This speed restriction should remain in place until a further repair is made and it is confirmed that the repair work has improved the vertical track geometry. Action taken Freightliner, the wagon owner and operator, carried out additional checks to identify any other wagons with the same worn suspension component and modified the maintenance regime for these wagons. Network Rail instructed its staff to always impose an emergency speed restriction for cyclic top defects, which shall remain in place until monitoring has shown that its staff have made an effective repair. Recommendations Freightliner should amend its vehicle maintenance instructions for its fleet of PCA wagons so that each damper pad is removed and measured during the VIBT examination to identify those wagons which have had levels of damper pad wear (on any corner) that exceed the permitted wear limit since the last VIBT examination. For each wagon identified, Freightliner should implement measures to prevent it being used in service with a damper pad that could wear beyond the permitted wear limit before its next VIBT examination. These measures could include: o Additional monitoring or checks for that wagon in between VIBT examinations; o Replacing damper pads on that wagon at an earlier interval; or o Carrying out work to identify and address the reasons why that wagon has had a high level of damper pad wear, such as pedestal or wheelset alignment. Network Rail should investigate why water is not draining from the track bed in the vicinity of where the train derailed (between 99 miles 220 yards and 99 miles 264 yards on the Down Produced by RSSB Author: Dr Greg Morse Email address: Greg.Morse@rssb.co.uk Sunderland line between Pelaw and Newcastle) and implement measures to control the risk of excess water affecting the track’s vertical geometry. Such measures could include ballast cleaning, remedial work to improve the effectiveness of the installed track drainage, through to a renewal of the track. Network Rail should review the condition of the track assets in the area covered by the Newcastle Track Section Manager against the records on its system for maintaining its track assets (Ellipse). The aim of the review should be to identify track defects requiring maintenance action which are either not recorded on Ellipse, do not have a planned date for repair, or have not been correctly prioritised for repair. Once identified, these defects should be recorded on Ellipse, prioritised and given a date for repair. Network Rail should investigate why its track assets within the area covered by the Newcastle Track Maintenance Engineer consistently have the highest numbers of reportable track geometry defects and sections of track in the super-red category on LNE Route. The investigation should include consideration of: o The number of staff needed to maintain the track assets in the Newcastle Track Section Manager area, so that both reactive and planned volumes of preventative maintenance activities are delivered; o The effect that changes to safe systems of work used by the track maintenance teams has had on the time spent working on the track; o The effect that the introduction of PLPR within the track inspection regime has had on increasing the track maintenance workload; o The types and numbers of track assets in the Newcastle Track Maintenance Engineer’s area, their age, and their condition, in comparison to the other Track Maintenance Engineer areas on LNE Route; and o The effect that any other factors have had in contributing to the high number of track asset defects. Based on the findings of the above investigation, Network Rail should determine what the appropriate target values are for the numbers of reportable track geometry defects and sections of track in the super-red category in the Newcastle Track Maintenance Engineer area. Network Rail should then take action to improve the maintenance of the track assets in this area to a level that allows these targets to be met. Network Rail should investigate why its management arrangements allowed non-compliances to processes for track asset maintenance to go undetected in the area covered by the Newcastle Track Maintenance Engineer, which correspondingly had the highest numbers of reportable track geometry defects and eighth of a mile sections of track in the super-red category when compared to other areas. The investigation should include consideration of: o Why its audit and self-assurance framework did not identify the full extent of the non-compliances to processes found by RAIB; o Why its reporting and monitoring processes did not trigger earlier action by senior management within the Route to resolve the persistent problems affecting the track assets in the Newcastle Track Maintenance Engineer area; and o Whether there are other Track Maintenance Engineer areas, like the one at Newcastle, with persistent non-compliances to processes that are affecting the maintenance of its track assets. Produced by RSSB Author: Dr Greg Morse Email address: Greg.Morse@rssb.co.uk Based on the findings of its investigation, Network Rail should take action to improve the management arrangements at Route level that audit, monitor and review the performance of a local area to highlight non-compliances which are resulting in persistent deficiencies with the maintenance of its track assets. Back to top 25 September Australia: Level crossing collision at Woodvale, Victoria, 19 December 2014 For the full report, click here: LINK On 19 December 2014, a lorry collided with a Swan Hill–Melbourne service at a level crossing on Rileys Road, Woodvale, Central Victoria. Both occupants of the lorry and one rail passenger were taken to hospital with minor injuries. The lorry sustained significant damage to its front right-hand corner; the train also sustained damage to its side panel and the underfloor sections of several of its carriages. The ATSB found that the truck driver did not approach the level crossing with sufficient caution to be able to stop once he became aware of the approaching train. A road-user’s view of an approaching train was partially obscured due to lineside vegetation. Safety message The ATSB note that this incident highlights the responsibility that rests upon road vehicle drivers to remain aware when approaching railway level crossings, especially those with passive protection. Road users who frequently use a level crossing that sees limited rail traffic should be alert to the potential of developing a sense of expectancy that trains will not be present. Drivers of heavy vehicles have a special responsibility to ensure they remain aware of the dangers of railway level crossings. To ensure that road users can make a determination regarding crossing the track safely, it is important that the infrastructure manager ensures that any lineside vegetation that might reduce the road user’s distant view of the track approaches be kept to an effective minimum. Back to top Produced by RSSB Author: Dr Greg Morse Email address: Greg.Morse@rssb.co.uk