Are Obesity and Physical Activity Clustered? articles Nadine Schuurman
advertisement

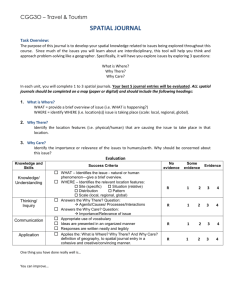
articles nature publishing group Epidemiology Are Obesity and Physical Activity Clustered? A Spatial Analysis Linked to Residential Density Nadine Schuurman1, Paul A. Peters2 and Lisa N. Oliver2 The aim of this study was to examine spatial clustering of obesity and/or moderate physical activity and their relationship to a neighborhood’s built environment. Data on levels of obesity and moderate physical activity were derived from the results of a telephone survey conducted in 2006, with 1,863 survey respondents in the study sample. This sample was spread across eight suburban neighborhoods in Metro Vancouver. These areas were selected to contrast residential density and income and do not constitute a random sample, but within each area, respondents were selected randomly. Obesity and moderate physical activity were mapped to determine levels of global and local spatial autocorrelation within the neighborhoods. Clustering was measured using Moran’s I at the global level, Anselin’s Local Moran’s I at the local level, and geographically weighted regression (GWR). The global-level spatial analysis reveals no significant clustering for the attributes of obesity or moderate physical activity. Within individual neighborhoods, there is moderate clustering of obesity and/or physical activity but these clusters do not achieve statistical significance. In some neighborhoods, local clustering is restricted to a single pair of respondents with moderate physical activity. In other neighborhoods, any moderate local clustering is offset by negative local spatial autocorrelation. Importantly, there is no evidence of significant clustering for the attribute of obesity at either the global or local level of analysis. The GWR analysis fails to improve significantly upon the global model—thus reinforcing the negative results. Overall, the study indicates that the relationship between the urban environment and obesity is not direct. Obesity (2009) doi:10.1038/oby.2009.119 Introduction Obesity levels in Canada have risen over the past several ­decades and these increases are troubling because of their associated comorbidities such as diabetes, cancer, and heart disease (1). In an effort to understand this trend, researchers are now focusing on the possible links between the physical environment and rising rates of obesity (2). In Canada, individuals who engage in walking and other forms of physical activity have been found to be less likely to be overweight or obese (1). Recent studies have broadened the scope of this exploration to probe the associations among obesity, the likelihood of engaging in physical activities, and the nature of the built urban environment (3–9). The built environment comprises all the elements constructed or modified by people— ranging from buildings, to transportation systems, to public spaces, and parks (10). These studies have shown that the built environment can play both a positive and a negative role in facilitating physical activities like walking (3,11–15). Although walkability, urban form, density, and access to green spaces (3–9) have been identified as components of the built environment that may influence obesity and levels of physical activity, studies have revealed conflicting results about the extent of this influence (13,16–19). This finding underscores the complexity of these relationships. For example, although some studies indicate a positive association between access to green space and physical activity (9), the results of other studies showed no significant relationship (17,18). A possible reason for this inconsistency is that multiple variables must be considered. It becomes important to understand, for example, the extent to which the physical environment actually influences one’s choice to walk—and how this balances with the role of other determinants of walking, like one’s ­ultimate destination (20). As this field of study matures, there is an increasing need for precision in parsing these associations and it is, therefore, critical that we employ reliable objective instruments to ­measure and confirm the actual existence and extent of these associations (21). Spatial methods of analysis are uniquely able to contribute to this level of evidence. Most studies examining the influence of the built environment on physical activity use nonspatial methods such as multilevel modeling (22) or regression (12,21,23). Studies using spatial methods to examine relations between the built environment and physical activity or obesity are rare. Such studies, however, may be useful because they can identify clusters of individuals 1 Department of Geography, Simon Fraser University, Burnaby, British Columbia, Canada; 2Health Information and Research Division, Statistics Canada, Ottawa, Ontario, Canada. Correspondence: Nadine Schuurman (nadine@sfu.ca) Received 21 May 2008; accepted 21 March 2009; advance online publication 23 April 2009. doi:10.1038/oby.2009.119 obesity 1 articles Epidemiology exhibiting similar health behaviors or patterns, which may be linked to the built environment. Traditionally, standard regression has been used to reveal such patterns. The argument presented in this paper asserts that spatial tests of local clustering are less susceptible to measurement bias than their aspatial global counterparts, as they account for the possible spatial autocorrelation of observations. Aspatial regression methods are generally predicated on the assumption of spatial independence of observations. An exception to this is the geographically weighted regression (GWR) method that employs a locally weighted approach to regression analysis and allows for parameter estimates to vary across the study space. The Centers for Disease Control defines a cluster as “an unusual aggregation, real or perceived, of health events that are grouped together in time and space and that are reported to a health agency” (24). Many health-related behaviors are clustered with links to the built environment. Chaix et al., for example, found a distinct spatial distribution for two classes of mental disorder at the neighborhood and local level (25). Clusters of health-related behaviors associated with weight gain and physical activity have also been linked to factors within the built environment. One study found youth distributed into nonoverlapping activity/inactivity clusters that could be used to predict overweight (26). In another study, obesity, diabetes, and hypertension were found to be clustered based on census tract variables (27). Mobley et al. investigated the presence of spatial clustering in high BMI, low BMI, and smoking to find significant differences in neighborhood characteristics linked to smoking (28). They concluded that cluster analysis indicates the value of spatial methods for policy application and evaluation purposes. These initial uses of spatial cluster analysis is for determining patterns of correlation in the built environment inform this study. Spatial clustering techniques are commonly employed in conjunction with geographic information systems to explore whether patterns of distribution for a variable have significance. The search for positive—or negative—spatial autocorrelation among variables is based on Tobler’s first law of geography which states that “everything is related to everything else, but near things are more related than distant things” (29). Spatial analysis allows researchers to determine whether observations within a study area are random or exhibit a significant deviation from a pattern that would likely arise from random underlying factors. If a set of observations is not random, then it becomes important to measure the degree and the nature of the spatial distribution in order to make relevant hypotheses on its underlying cause. It is important to rely on quantitative metrics for objective measures of spatial patterns, because even when data are mapped, individuals often have difficulty recognizing or identifying random distributions; rather they often “see” clusters when none truly exist (30). Spatial analysis instruments in this study include Moran’s I, Anselin’s Local Moran’s I—a local indicator of spatial autocorrelation (LISA)—and GWR. The purpose of this study is to determine whether significant patterns of clustering of obesity and/or moderate physical activity can be revealed. This hypothesis is tested via spatial cluster analysis within eight suburban neighborhoods. Neighborhoods are selected for contrasting levels of income and residential density and are not selected at random. Multiscale analysis is performed to allow identification of clusters within and between neighborhoods. This method also allows comparisons to be made regarding the frequency and density of clustering within the two residential density categories. This paper further examines the association between the degree of clustering of obesity and physical activity relative to specific combinations of built environment. The central hypothesis of this paper is that the physical built environment has a direct influence on clustering of obesity and physical activity. Methods And Procedures The neighborhoods The study area (Figure 1) consists of eight neighborhoods with ­different combinations of built environments, further qualified by income level. Each neighborhood area comprises 3–4 census tracts with resulting populations varying between 11,000 and 17,000. Residential density is Locations of study neighborhoods Newport High income High density Maillardville Low income Low density Sapperton High income High density Fraser Heights High income Low density Hammond High income Low density Edmonds Low income High density Greater Vancouver Whalley Low income Low density Langley Low income High density Area of detail Figure 1 The eight suburban neighborhoods used in this study and their location in the context of Metro Vancouver. 2 www.obesityjournal.org articles Epidemiology defined as population per hectare of residential land, as designated by the Greater Vancouver Land Use Data. A description of these data is available elsewhere (21). Areas with the highest and lowest residential densities are excluded from the study as densities are needed to reflect a suburban profile. Of the qualifying areas, four neighborhoods represent a higher residential density while the other four represent a lower residential density. The study areas are also categorized by median family income, calculated using census data from the 2001 Census of Canada. Areas that fall within the highest and lowest income deciles are excluded so as to select typical neighborhoods rather than areas of extreme poverty of affluence. Income categories for this study are classified as higher median family income (CDN $53,000–77,000) and lower median family income (CDN $32,000–44,000). Neighborhood selection avoided extremes of income and density in favor of areas with relatively high automobile use and largely middle class households. These categories are then combined with the residential density categories to render four groupings, each represented by two neighborhoods: lower density/higher income; higher density/lower income; higher density/higher income; and higher density/ lower income. Survey data Data on individuals were collected through a telephone survey of adults ≥aged 19, residing in the eight designated neighborhoods. The ­average length of residence for these respondents was 8.5 years. A sampling frame of households in each neighborhood was constructed from the regional telephone provider and numbers were selected by Random Digit Dialing. A minimum baseline of five call-backs for each selected number was used to reduce bias due to nonresponse. The ­survey was conducted by trained interviewers using Computer Assisted Telephone Interviewing. The survey achieved a response rate of 29% providing 1,935 respondents. For this study, we use data from the 1,863 ­respondents with valid postal codes. An analytic sample of 1,789 is used for weight and an analytic sample of 1,796 is used for moderate ­physical activity, due to the exclusion of 74 and 67 respondents, respectively, with missing variables. The survey was piloted in January 2006 and the full survey was conducted over 2 weeks in February 2006. Physical activity and obesity measures Respondents were asked a series of five survey questions that probed walking and physical activity (Table 1). Each survey question offered a range of 5–6 possible responses. These responses were then dichotomized by designating the two least active options as “nonactive” and the remaining responses as “active.” The Active responses were then tallied to form a broad index of overall physical activity. An individual with a score of ≥3 on this index (an Active response in at least three of the five questions) was designated as ­moderately active. Moderate physical activity, therefore, was defined in two possible combinations: a minimum of 3–3.75 h of physical activity per week combined with >2 h of sedentary leisure per day or, a minimum of 2–2.75 h of physical activity per week combined with <2 h of sedentary leisure per day. The benchmark of 3–3.75 h was selected because it closely reflects the 30 min per day of physical activity recommended by Canada’s Physical Activity Guide (31). We believe that for individuals with <2 h of sedentary leisure per day, 2–2.75 h of physical activity per week should put them in a similar standing because their reduced hours of sedentary leisure likely imply the presence of some degree of other moderate physical activity unaccounted for within the framework of the questions asked. The classification of respondents into the category of obese was done using self-reports of height and weight. With these data, standard BMI was calculated and respondents were classified so that an individual with a BMI ≥30 was classified as obese. Spatial analysis The locations of survey respondents are geocoded from their postal codes provided in the survey. The 2005 Unique Enhanced Postal Code product from Desktop Mapping Technologies Inc.’s CanMap Postal obesity Geography v2005.3 (Markham, Ontario, Canada) is used to determine precise geographic coordinates corresponding to each postal code (32). The postal code information provides a means of locating each respondent so that spatial correlation of particular attributes can be assessed among all respondents within each suburban neighborhood. In urban areas, postal codes cover ~15 households and as such provide a relatively accurate estimate of an individual’s residential location (33). In some cases respondents have the same postal code, likely due to residing in the same apartment building, and thus are given the same point location, resulting in the spatial duplication of some respondents. These respondents are not excluded as the methods employed can account for the increased local density of point locations. The first spatial measure used, the Moran’s I, is a global measure of ­spatial autocorrelation that quantifies the degree to which data are clustered or uniformly distributed overall (34,35). Recent studies have used it to evaluate the presence of spatial autocorrelation and spatial clusters in a range of attributes such as hemorrhagic fever with renal syndrome (36), neonatal characteristics and socioeconomic conditions (37), influenza (38,39), pneumonia (38), human brucellosis (40), and breast, lung, and colorectal cancer (41). Spatial proximity and differences in attribute values are evaluated in concert for all pairs of observations. Values for Moran’s I vary from +1 (strong positive spatial autocorrelation with similar values located near one another) to −1 (strong negative spatial autocorrelation with high values located nearest to low values and vice versa). A value near 0 implies a lack of spatial pattern (i.e., random distribution). The null hypothesis of no spatial pattern can be evaluated using a Z-score created from the mean and variance of I (42). Although the value of the Moran’s I itself can be a useful comparison, care must be taken in interpretation when a low Z-score is obtained. In this study, the Moran’s I test statistic is used to test for global spatial autocorrelation of physical activity and obesity across eight neighborhoods. Inverse distance squared weighting is used to measure the spatial relationships among respondents for the two attributes, obesity and moderate physical activity. This measure determines the relative influence that should be given to all other respondents when local spatial autocorrelation is calculated for one particular respondent. With inverse distance squared weighting, the influence of each location on the overall calculation decreases exponentially with distance. That is, when calculating the local spatial autocorrelation for a particular Table 1 The dichotomization of survey responses to questions regarding physical activity and sedentary leisure into “active” and “nonactive” responses Active Nonactive Q18: “In a typical week in the past 3 months how many hours did you usually spend walking to and from work or school?” Question >1 h <1 h Q19: “In a typical week in the past few months how many hours did you spend walking from home to grocery stores banks or to do other errands?” >1 h <1 h Q21: “In a typical week in the past 3 months how many days did you do at least 30 minutes of moderate physical activity such as brisk walking running swimming or team sports?” ≥2 days ≤1 day Q22: “On a typical day in the past 3 months how much time did you spend walking for leisure?” ≥16 min ≤15 min Q23: “On a typical day in the past 3 months how much time did you spend sitting while doing leisure activities such as: reading, watching T.V., on the computer, or playing video games?” <2 h >2 h 3 articles Epidemiology respondent, the greatest weight is given to the most proximate individuals. The Moran’s I test generates an index value and associated Z-score for each variable for each neighborhood. The Z-scores are used to identify the attributes that exhibited a significant degree of global spatial autocorrelation within a particular neighborhood. Individual clusters or smaller regions of clustering that are not ­evident within the global pattern may appear during analysis at the local level (30). To evaluate the existence of local clusters, it is necessary to use local statistics. The local Moran’s I decomposes the global measure into the contributions for each location, detecting similarities or dissimilarities in values around a given observation and thus measuring the local spatial autocorrelation at each observation point (43). These statistics are also known as Local Indicators of Spatial Association (LISAs), which can be indicators of local spatial clustering or used as diagnostics for outliers in global patterns. The sum of local Moran’s I values is proportional to global Moran’s I. Anselin’s Local Moran statistic is subsequently used to test for local spatial autocorrelation among respondents within each neighborhood for each of the same two variables. Inverse distance weighting squared is again used to conceptualize the spatial relationships. Respondents with missing data for a particular variable are excluded from any further analysis of that variable. An index value and Z-score are calculated for each respondent in each data layer. The Z-scores are used to identify respondents that exhibit a significant degree of local spatial autocorrelation for a particular variable within a particular neighborhood. Results of these analyses are mapped, highlighting respondents showing instances of significant positive and/or significant negative local spatial autocorrelation. If a perfectly homogenous cluster exists in the underlying population, it is expected that a grouping of respondents with significant positive local spatial autocorrelation would be visually evident. As is common practice for local analysis of spatial autocorrelation, maps are visually inspected for the presence of areas with a concentration of respondents with significant positive local spatial autocorrelation within close proximity of each other. For the purposes of this study, clear definitions of what constitutes evidence of local clustering are developed. First, groupings of four or five significant positive results in close proximity are considered to be moderate ­evidence suggesting the possibility of underlying clustering in the population. ­Second, groupings of six or more significant positive results in close proximity are considered to be stronger evidence supporting the existence of such underlying clustering. Inversely, evidence of significant negative local spatial autocorrelation amongst any of these groups is considered to weaken the evidence of the existence of an underlying cluster. The third method used to test the hypothesis for a relationship between obesity, physical activity, and the built environment is GWR. The essence of GWR is that a traditional regression framework is respecified using a locally weighted subsample of the population, to allow for the estimation of local parameters for each observation as opposed to a single parameter set for all observations. The power of the GWR approach is that for each observation point i, it is possible to produce a complete set of parameter estimates, local standard errors, measures of significance, influence statistics, and importantly, local r2 values. Additionally, it is possible to specify different methods for the local area sample, allowing for hypotheses on the spatial level of interaction to be tested. The analysis in this paper employs a binary logistic model with obesity as the response variable and moderate physical activity as an independent variable. Dummy variables for neighborhood density and median income are included. Results Table 2 summarizes the findings for obesity, overweight, and moderate physical activity rates for the eight neighborhoods. Table 3 identifies levels of physical activity over 3 h a week for the same neighborhoods. The global Moran’s I test statistic is evaluated for both ­obesity and moderate physical activity within each neighborhood (Table 3). Global dispersion means that individuals who are obese/nonobese (physically activity/not physically active) are not found in close proximity but distributed regularly throughout all the study areas. None of the neighborhoods exhibit statistically significant evidence of global clustering. This suggests that the built urban environment has little or no effect on the likelihood of finding this variable. None of the remaining variables exhibit a statistically significant degree of global clustering. Anselin’s Local Moran’s I is used to evaluate the existence of local clustering not evident within the global neighborhood ­patterns. Any region with multiple cases of significant local spatial autocorrelation provides evidence in support of the existence of an underlying cluster in the population. The mapped results of these analyses of local spatial autocorrelation in obesity are presented in Figure 2. The results for ­physical activity are not shown here for space considerations. Cases of both significant positive and significant negative local ­spatial autocorrelation are indicated. Table 2 Survey respondents by neighborhood, summarizing their respective rates of overweight, obesity, and a moderate level of activity Respondents Whalley 233 Overweight (%) Obese (%) Moderately active (%) 53.6 17.1 42.9 Edmonds 229 48.1 18.1 56.8 Maillardville 247 46.6 14.0 47.5 Langley 231 55.9 13.5 53.6 Sapperton 230 53.6 19.8 46.4 Hammond 238 61.6 18.1 51.1 Newport 252 42.3 14.2 53.5 Fraser Heights 203 41.5 13.5 45.9 1,863 50.5 16.0 49.8 Total Table 3 Global Moran’s I test results for obesity and moderate physical activity by neighborhood Edmonds Fraser Heights Hammond Langley Maillardville Newport Sapperton Whalley −0.20 −0.01 0.01 0.00 −0.01 0.01 −0.01 0.00 Obesity (BMI >30) Moran’s I Z-score −1.29 −0.71 1.07 0.15 −0.72 0.10 −0.45 0.01 Physical activity (activity index 3+) Moran’s I −0.02 −0.01 −0.01 −0.02 −0.01 −0.02 0.00 0.00 Z-score −1.12 −0.75 −0.10 −1.12 −0.63 −1.07 0.52 0.01 4 www.obesityjournal.org articles Epidemiology High density neighborhoods Low density neighborhoods Newport Hammond Fraser Heights High income Sapperton Langley Whalley Maillardville Low income Edmonds Local Moran’s I <−2.0 −2.0 to −1.0 −1.0 to 1.0 1.0 to 2.0 >2.0 Figure 2 Moderate evidence of local clustering of obesity. There are several cases of strong positive spatial autocorrelation located within close proximity in several neighborhoods. However, these cases still do not meet the criteria of six cases required to conclude that there is significant local clustering. In Figure 2, there is moderate evidence of local clustering of obesity (several cases of strong positive spatial autocorrelation located within close proximity) within central and southwestern Sapperton. There is stronger evidence of local clustering in south-central Langley, Fraser Heights, and southeastern Hammond. The only neighborhood with potentially significant local clustering is in southern Langley, where there is a cluster of six higher than expected values. All neighborhoods contain respondents showing significant local spatial autocorrelation but widely separated individuals or pairs of such cases (e.g., Edmonds, Whalley) do not meet the criteria required to conclude there is significant clustering within the population. In other words, sporadic local clustering of obesity does not constitute significant clustering. The LISA analysis of physical activity (not shown here) demonstrates moderate evidence of local clustering of moderate physical activity within Maillardville and strong evidence for such clustering within Whalley. Similar to obesity, each of the study neighborhoods contains cases of significant local positive spatial autocorrelation but as these cases are dispersed, they do not provide evidence of local clustering in the underlying population. The Sapperton area provides an excellent example of a neighborhood with many individual cases of significant positive local spatial autocorrelation for respondents with moderate physical activity. However, there is no coherent evidence of any clustering in this attribute within the population given the dispersion of individual cases across the neighborhood. Neither obesity nor physical activities are affected by higher vs. lower density or different income levels. This is an unexpected result that begs the question of whether or not there are clear links between the built environment and obesity and/or ­physical activity. It certainly invites further investigation. obesity The results of the GWR analysis (Figure 3) do not provide significantly different results than those found by either the global-level Moran’s I statistic or the LISA analysis. The local regression model is highly simplified and developed to test the relationship between obesity and physical activity within each of the study neighborhoods. If local variation was apparent there would be visual differences in both the local r2 values and in the parameter estimates. As is apparent from Figure 3, while there are differences between the local r2 values and the parameter estimates of activity, they are very small and do not correspond to any statistical significance via Monte Carlo or Leung significance tests. Thus, from the testing done here, there is no significant difference between these values, suggesting that the relationship between obesity and physical activity was the same for all of the neighborhoods. Additionally, the GWR model is used to calculate the Aikaike information criterion for both the global and local models. The global model has a corrected Aikaike information criterion of 1,509 with the local model reporting a corrected Aikaike information criterion of 1,511. This suggests that not only is there no significant difference at the local level, the local model is a slightly poorer fit than at the global level. This confirms our results: spatial clustering of obesity and physical activity is not directly influenced by the urban built environment. Discussion There is a growing body of literature exploring the influence of the built environment on both obesity and physical activity. This literature is mixed in its conclusions with respect to the effect of the environment on obesity. Whilst studies generally agree that walkability influences levels of physical activity (7,12,23), there are a number of other known risk factors including childhood 5 articles Epidemiology Local r 2 0.015 − 0.017 0.018 0.019 − 0.021 Activity parameter −0.261 to −0.253 −0.252 to −0.220 −0.219 to −0.203 0 2.5 5 km 10 N Figure 3 Schematic representation illustrates that we do not have significantly different results, using geographically weighted regression, than those found by either the global-level Moran’s I statistic or the LISA analysis. None of the local areas indicates a significantly different relationship between the dependent and independent variables. obesity, educational status, and related health risks (44–47). In this study, the assumption is that if the built environment affects behavior and health, physical activity and obesity will be clustered. If there is indeed a positive association between the physical context of one’s life and one’s health-related behaviors and outcomes, this association may reveal itself in obesity and physical activity clusters within a neighborhood. The built environment in any neighborhood determines the ease and access to commercial and retail amenities, the numbers of and proximity to parks and recreational facilities, and the extent to which an area is pedestrian friendly. Physical activity and obesity, therefore, may show distinct patterns relative to the underlying built environment, particularly at the local level. Utilizing the Moran’s I, the Anselin’s Local Moran’s I, and GWR instruments, this study maps data on obesity and moderate physical activity across eight suburban neighborhoods. 6 A number of neighborhoods are selected in order to provide diversity between densities of built environment assuming that different blends of neighborhood amenities and recreational areas might have revealed different patterns. The neighborhoods, therefore, represent two levels of residential density and two levels of income in four different combinations: high density/high income; high density/low income; low density/ high income; and low density/low income. Data are gathered from adults residing within those neighborhoods through a telephone survey. Geographic information systems and spatial mapping techniques are uniquely suited to identifying and analyzing these physical patterns of distribution. They provide the means to effectively and efficiently ascertain whether patterns of significance do indeed exist. Once patterns like clustering are geographically located and verified, further investigation into ground-level influences can proceed. There is, for instance, some evidence of moderate local clustering of physical activity in Whalley. This is an area where the local light rapid transit system, the SkyTrain, converges with local parks and commercial areas. Certainly moderate local clusters could provide the basis for more intensive qualitative examinations of possible correlation between the built urban environment and physical activity and/or obesity. The global analysis of possible clustering of obesity and/ or moderate physical activity across eight suburban neighborhoods yielded only one result of statistical significance. In the Edmonds neighborhood, a high density/low income area, there was evidence of uniform spatial distribution for obesity, i.e., dispersion rather than any clustering. We do not know of any underlying mechanism that would explain this result, nor have we encountered anything in the literature to suggest that this might ever occur. We believe that it is a random result or a product of random factors. Second, for our purposes of identifying potential clustering it consolidates our conclusion that there is no global clustering in Edmonds. The remaining neighborhoods showed no significant patterns of positive or negative distribution of clusters for moderate physical activity. None of the neighborhoods revealed any significant clustering for obesity. At the local level, on the other hand, some of the study areas did reveal patterns suggesting moderate to strong evidence for the existence of underlying areas of local clustering. This may suggest underlying spatial nonstationarity, where the structure of spatial dependency for obesity is heterogeneous. In short, our findings at the global level did not reveal a close association between obesity and/or moderate physical activity and the built urban environment. Although many of the studies examining the phenomenon of clustering employ spatial analysis at the global level only, this study took a multi-scale approach and “zoomed in” to ­examine patterns of distribution at the local level as well. This more granular level of analysis allows patterns of local ­spatial distribution to be revealed that may otherwise have been masked or obscured by the presence or absence of the more remote global patterns, as was the case with these data. In this www.obesityjournal.org articles Epidemiology case, lack of clustering at the global level indicates both lack of a clear causal relationship and possible obfuscation of a scaledependent pattern. Although the overall results of this study indicate that ­obesity and physical activity are not closely linked to the built urban environment, some of the study areas did reveal ­patterns ­suggesting moderate to strong evidence for the existence of underlying local clustering. Local analysis does, therefore, offer the basis for a closer examination of possible links that are only discernable at a large scale (small area) of analysis. This study did have certain limitations. Although eight areas were examined, with different density and income profiles, a greater number of area samples as well as a more granular level of distinction between each composite area’s factors may have rendered more detailed information about patterns relative to variables of income, access to retail, greenways, etc. The nature of the neighborhoods themselves, being suburban, may have contributed to the low level of findings. However, our study considered a diverse mix of land-uses as well as many variations of green space within walking ­distance of individuals (21). Deriving data from self-reports of physical activity and height and weight is often subject to bias. Women and men tend to under-report weight and over-report height, making BMI measurements derived from surveys subject to a potential skew downward (48). Accuracy in recall for levels of physical activity is less likely to be an issue, as these are current daily or weekly activities, although demand characteristic bias may have influenced some respondents to adjust their responses in the hopes of providing what they felt might be the “right” answer. The survey was conducted in February, which is typically rainy and cold; results may have differed if the survey was conducted during a warmer month. A further limitation to this approach exists with regard to the attribute of obesity. Although patterns of significance were not found in this study, pattern analysis would have to take into consideration the onset period inherent in weight gain and attaining the BMI values associated with obesity. Should an influence exist between the built environment and obesity, it would need to be ascertained whether the condition of ­obesity was primarily influenced by the current neighborhood or by previous physical contexts. Moreover, the study design does not permit analysis of the possible influence of social networks on obesity and levels of physical activity (49). Social networking is becoming ever more ubiquitous with the exponential growth of the web. Web 2.0 broadly refers to a new generation of internet services and technology (50–52). Web 2.0 heralds a transition from local pockets of isolation to a global interconnectedness. Should social network become the pervasive form of interpersonal communication, this may have important health considerations (53). Certainly social networking is an emerging model that may partially explain patterns of obesity not directly related to the urban environment. Future studies may employ more complex questioning about social networks to determine possible influence. Social networks present an example of nonlinear, obesity nonspatial, and easily obfuscated influences on incidence of obesity and physical activity. Geographic information systems and spatial analysis provide an important means of broadening the exploration of the relationship between the built environment and personal levels of physical activity, interaction with the physical environment, and health outcomes. They provide a level of evidence much needed by researchers seeking to determine whether or not associations between the physical environment and behaviors are indeed present. Using spatial analysis, this study was designed to detect the presence or absence of evidence supporting spatial clustering of the attributes of obesity and moderate physical activity within eight study neighborhoods. Although no patterns of significance for either obesity or moderate physical activity were determined at the global level, by employing a multi-scale approach pockets of local clustering of moderate physical activity were identified within a variety of neighborhoods—pockets that had not been apparent at the global level. The evidence of physical activity clustering at the local level, although inconsistent, may yet indicate that there could be specific area features within a neighborhood that may warrant further investigation. There were, however, no similar local findings for the attribute of obesity. Although this does not rule out the possibility of association between ­obesity and the build environment, it does indicate that the relationship is more spatially complex than has been ­previously acknowledged. Acknowledgments We thank the Canadian Institutes of Health Research (CIHR) for their funding through grant #116338, as well as support from the Canadian Institute for Health Information and the Canadian Population Health Initiative. We also thank Alex Hall for his substantial technical assistance with the initial analysis. Ellen Randall thoroughly read two drafts of this paper and offered valuable editing suggestions. In addition, N.S. acknowledges the Michael Smith Foundation for Health Research and CIHR for their continued research support. Disclosure The authors declared no conflict of interest. © 2009 The Obesity Society References 1. Tjepkema M. Adult obesity. Health Rep 2006;17:9–25. 2. Hill JO, Peters JC. Environmental contributions to the obesity epidemic. Science 1998;280:1371–1374. 3. Frank LD, Schmid TL, Sallis JF, Chapman J, Saelens BE. Linking objectively measured physical activity with objectively measured urban form: findings from SMARTRAQ. Am J Prev Med 2005;28(Suppl 2):117–125. 4. Li F, Fisher KJ, Brownson RC, Bosworth M. Multilevel modelling of built environment characteristics related to neighbourhood walking activity in older adults. J Epidemiol Community Health 2005;59:558–564. 5. Boer R, Zheng Y, Overton A, Ridgeway GK, Cohen DA. Neighborhood design and walking trips in ten U.S. metropolitan areas. Am J Prev Med 2007;32:298–304. 6. Berke EM, Koepsell TD, Moudon AV, Hoskins RE, Larson EB. Association of the built environment with physical activity and obesity in older persons. Am J Public Health 2007;97:486–492. 7. Michael Y, Beard T, Choi D, Farquhar S, Carlson N. Measuring the influence of built neighborhood environments on walking in older adults. J Aging Phys Act 2006;14:302–312. 8. Craig CL, Brownson RC, Cragg SE, Dunn AL. Exploring the effect of the environment on physical activity: a study examining walking to work. Am J Prev Med 2002;23(2 Suppl):36–43. 7 articles Epidemiology 9. Neuvonen M, Sievänen T, Tönnes S, Koskela T. Access to green areas and the frequency of visits—a case study in Helsinki. Urban For Urban Green 2007;6:235–247. 10. National Institute of Environmental Health Sciences—National Institutes of Health. Obesity & the Built Environment <http://www.niehs.nih.gov/news/ events/pastmtg/2004/built/> (2004). 11. Gordon-Larsen P, Nelson MC, Page P, Popkin BM. Inequality in the built environment underlies key health disparities in physical activity and obesity. Pediatrics 2006;117:417–424. 12. Frank LD, Andresen MA, Schmid TL. Obesity relationships with community design, physical activity, and time spent in cars. Am J Prev Med 2004;27:87–96. 13. Wendel-Vos W, Droomers M, Kremers S, Brug J, van Lenthe F. Potential environmental determinants of physical activity in adults: a systematic review. Obes Rev 2007;8:425–440. 14. Lake A, Townshend T. Obesogenic environments: exploring the built and food environments. J R Soc Promot Health 2006;126:262–267. 15. Lopez RP, Hynes HP. Obesity, physical activity, and the urban environment: public health research needs. Environ Health 2006;5:25. 16. Forsyth A, Oakes J, Schmitz K, Hearst M. Does residential density increase walking and other physical activity? Urban Stud 2007;44:679–697. 17. McCormack GR, Giles-Corti B, Bulsara M. The relationship between destination proximity, destination mix and physical activity behaviors. Prev Med 2008;46:33–40. 18. Hillsdon M, Panter J, Foster C, Jones A. The relationship between access and quality of urban green space with population physical activity. Public Health 2006;120:1127–1132. 19. Handy SL, Boarnet MG, Ewing R, Killingsworth RE. How the built environment affects physical activity: views from urban planning. Am J Prev Med 2002;23:64–73. 20. Owen N, Humpel N, Leslie E, Bauman A, Sallis JF. Understanding environmental influences on walking; Review and research agenda. Am J Prev Med 2004;27:67–76. 21. Oliver LN, Schuurman N, Hall AW. Comparing circular and network buffers to examine the influence of land use on walking for leisure and errands. Int J Health Geogr 2007;6:41. 22. Ross NA, Tremblay S, Khan S et al. Body mass index in urban Canada: neighborhood and metropolitan area effects. Am J Public Health 2007;97:500–508. 23. Frank LD, Engelke P. The built environment and human activity patterns: exploring the impacts of urban form on public health. J Plann Lit 2001;16:202–218. 24. Guidelines for investigating clusters of health events. MMWR Recomm Rep 1990;39:1–23. 25. Chaix B, Leyland AH, Sabel CE et al. Spatial clustering of mental disorders and associated characteristics of the neighbourhood context in Malmö, Sweden, in 2001. J Epidemiol Community Health 2006;60:427–435. 26. Monda KL, Popkin BM. Cluster analysis methods help to clarify the activityBMI relationship of Chinese youth. Obes Res 2005;13:1042–1051. 27. Schlundt DG, Hargreaves MK, McClellan L. Geographic clustering of obesity, diabetes, and hypertension in Nashville, Tennessee. J Ambul Care Manage 2006;29:125–132. 28. Mobley LR, Finkelstein EA, Khavjou OA, Will JC. Spatial analysis of body mass index and smoking behavior among WISEWOMAN participants. J Women’s Health (Larchmt) 2004;13:519–528. 8 29. Tobler WR. A computer model simulation of urban growth in the Detroit region. Econ Geogr 1970;46:234–240. 30. Rogerson PA. Statistical methods for the detection of spatial clustering in case-control data. Stat Med 2006;25:811–823. 31. Public Health Agency of Canada (PHAC). Canada’s Physical Activity Guide to Healthy Living for Older Adults. Public Health Agency of Canada: Ottawa, Canada, 1998. 32. DMTI Spatial Inc. Unique Enhanced Postal Code. Version 2005.3. CanMap Postal Geography 2005. 33. Statistics Canada. 2001 Census Dictionary. Report no.: 92-378-XIE (2003). 34. Moran PA. The interpretation of statistical maps. J R Stat Soc Series B Stat Methodol 1948;10:243–251. 35. Moran PA. Notes on continuous stochastic phenomena. Biometrika 1950;37:17–23. 36. Fang L, Yan L, Liang S et al. Spatial analysis of hemorrhagic fever with renal syndrome in China. BMC Infect Dis 2006;6:77. 37. d’Orsi E, Carvalho MS, Cruz OG. Similarity between neonatal profile and socioeconomic index: a spatial approach. Cad Saude Publica 2005;21:786–794. 38. Crighton EJ, Elliott SJ, Moineddin R, Kanaroglou P, Upshur RE. An exploratory spatial analysis of pneumonia and influenza hospitalizations in Ontario by age and gender. Epidemiol Infect 2007;135:253–261. 39. Greene SK, Ionides EL, Wilson ML. Patterns of influenza-associated mortality among US elderly by geographic region and virus subtype, 1968–1998. Am J Epidemiol 2006;163:316–326. 40. Fosgate GT, Carpenter TE, Chomel BB et al. Time-space clustering of human brucellosis, California, 1973–1992. Emerging Infect Dis 2002;8:672–678. 41. Jacquez GM, Greiling DA. Local clustering in breast, lung and colorectal cancer in Long Island, New York. Int J Health Geogr 2003;2: 3. 42. Cliff AD, Ord JK. Spatial Processes: Models and Applications. Pion: London, 1981. 43. Anselin L. Local indicators of spatial association—LISA. Geogr Anal 1995;27:93–115. 44. Martínez-González MA, Martínez JA, Hu FB, Gibney MJ, Kearney J. Physical inactivity, sedentary lifestyle and obesity in the European Union. Int J Obes Relat Metab Disord 1999;23:1192–1201. 45. Mozaffari H, Nabaei B. Obesity and related risk factors. Indian J Pediatr 2007;74:265–267. 46. Reilly JJ, Kelly L, Montgomery C et al. Physical activity to prevent obesity in young children: cluster randomised controlled trial. BMJ 2006;333:1041. 47. Robinson TN, Sirard JR. Preventing childhood obesity: a solution-oriented research paradigm. Am J Prev Med 2005;28(2 Suppl 2):194–201. 48. Gorber SC, Tremblay M, Moher D, Gorber B. A comparison of direct vs. self-report measures for assessing height, weight and body mass index: a systematic review. Obes Rev 2007;8:307–326. 49. Christakis NA, Fowler JH. The spread of obesity in a large social network over 32 years. N Engl J Med 2007;357:370–379. 50. Solomon G, Schrum L. Web 2.0: New Tools, New Schools. ISTE: Washington, DC, 2007. 51. Greaves M, Mika P. Semantic Web and Web 2.0. Web Semantics: Science, Services and Agents on the World Wide Web 2008;6:1–3. 52. Deshpande A, Jadad AR. Web 2.0: could it help move the health system into the 21st century? J Mens Health Gend 2006;3:332–336. www.obesityjournal.org