Gifted Referral (for Private Schools)
advertisement
")
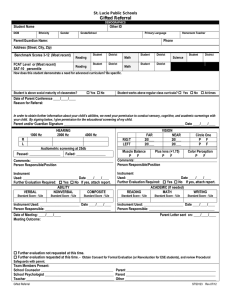
School Board of St. Lucie County Gifted Referral (for Private Schools) DEMOGRAPHICS Student Name DOB Other ID Ethnicity Gender Grade School Primary Language Parent/Guardian Name: Phone (multiple) H- Homeroom Teacher C- W- Address (Street, City, Zip) Academic Assessment (Most recent) Name of Assessment: National Percentile Rank National Percentile Rank Reading Math National Percentile Rank Science How does this student demonstrate a need for advanced curriculum? Be specific. Student is above social maturity of classmates? Yes No Student works above regular class curricula? Yes No At times Date of Parent Conference ____/____/____ Reason for Referral: In order to obtain further information about your child’s abilities, we need your permission to conduct sensory, cognitive, and academic screenings with your child. By signing below, I give permission for the educational screening of my child. Parent and/or Guardian Signature ______________________________________________________________________ Date ____/____/____ HEARING 2000 Hz 1000 Hz 4000 Hz R L Audiometric screening at 25db Passed: __________________ Failed: _________________ RIG T LEFT FAR 20/___ 20/___ VISION NEAR 20/___ 20/___ Circle One P F P F Comments:________________________________________________ Person Responsible/Position Muscle Balance Plus lens (+1.75) Color Perception P F P F P F Comments:________________________________________________ Person Responsible/Position Instrument Used: ________________________________ Date ____/____/____ Further Evaluation Required: Yes No If yes, attach report. ABILITY VERBAL NONVERBAL COMPOSITE Instrument Used: _______________________________ Date ____/____/____ Further Evaluation Required: Yes No If yes, attach report. ACADEMIC (If needed) READING MATH WRITING Standard Score - %ile Standard Score - %ile Standard Score - %ile Instrument Used: _______________________ Date ____/____/____ Person Responsible: ______________________________________ Standard Score - %ile Standard Score - %ile Standard Score - %ile Instrument Used: _______________________ Date ____/____/____ Person Responsible: ______________________________________ Date of Meeting: ____/____/____ Parent Letter sent on: ____/____/____ Meeting Outcome: Further evaluation not requested at this time. Further evaluation requested at this time. --- Obtain Consent for Formal Evaluation, and review Procedural Safeguards with parent. Team Members Present: School Counselor __________________________________________ Parent ____________________________________________________ School Psychologist ________________________________________ Parent ____________________________________________________ Teacher ___________________________________________________ Other _____________________________________________________ Gifted Referral for Private Schools Rev.09/11