Gifted Referral
advertisement

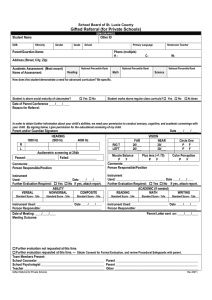
St. Lucie Public Schools Gifted Referral DEMOGRAPHICS Student Name DOB Other ID Ethnicity Gender Grade/School Primary Language Parent/Guardian Name: Homeroom Teacher Phone Address (Street, City, Zip) Benchmark Scores 3-12 (Most recent) FCAT Level or (Most recent) SAT-10 percentile Reading Reading Student District Student District Math Math Student District Student District Science Student District How does this student demonstrate a need for advanced curriculum? Be specific. Student is above social maturity of classmates? Yes No Student works above regular class curricula? Yes No At times Date of Parent Conference ____/____/____ Reason for Referral: In order to obtain further information about your child’s abilities, we need your permission to conduct sensory, cognitive, and academic screenings with your child. By signing below, I give permission for the educational screening of my child. Parent and/or Guardian Signature ______________________________________________________________________ Date ____/____/____ R L 1000 Hz HEARING 2000 Hz 4000 Hz Audiometric screening at 25db Passed: __________________ Failed: _________________ RIGT LEFT FAR 20/___ 20/___ VISION NEAR 20/___ 20/___ Circle One P F P F Comments:________________________________________________ Person Responsible/Position Muscle Balance Plus lens (+1.75) Color Perception P F P F P F Comments:________________________________________________ Person Responsible/Position Instrument Used: ________________________________ Date ____/____/____ Further Evaluation Required: Yes No If yes, attach report. ABILITY VERBAL NONVERBAL COMPOSITE Instrument Used: _______________________________ Date ____/____/____ Further Evaluation Required: Yes No If yes, attach report. ACADEMIC (If needed) READING MATH WRITING Instrument Used: _______________________ Date ____/____/____ Person Responsible: ______________________________________ Instrument Used: _______________________ Date ____/____/____ Person Responsible: ______________________________________ Standard Score - %ile Standard Score - %ile Date of Meeting: ____/____/____ Meeting Outcome: Standard Score - %ile Standard Score - %ile Standard Score - %ile Standard Score - %ile Parent Letter sent on: ____/____/____ Further evaluation not requested at this time. Further evaluation requested at this time. - Obtain Consent for Formal Evaluation (or Reevaluation for ESE students), and review Procedural Safeguards with parent. Team Members Present: School Counselor __________________________________________ Parent ____________________________________________________ School Psychologist ________________________________________ Parent ____________________________________________________ Teacher ___________________________________________________ Other _____________________________________________________ Gifted Referral STS0123 Rev.07/12