Document 11038347
advertisement

g
(
LIBRARIES)
'o/TV
C9
M.I.T.
LIBRARIES
-
DEWEY
>3,
HD28
.M414
Dynamic Multidrug Therapies for HIV:
A Control Theoretic Approach
Lawrence M. Wein, Stefanos
Zenios, and Martin A.
#3874-95-MSA
Nowak
December,
1995
MASSACHUSETTS INSTITUTE
^23
J/
1996
LIBRARIES
Dynamic Multidrug Therapies for HIV:
A Control Theoretic Approach
Lawrence M. Wein
Sloan School of Management, M.I.T.
Cambridge,
MA
02139
Stefanos Zenios
Operations Research Center, M.I.T.
Cambridge,
MA
02139
Martin A. Nowak
Department of Zoology, University
Oxford
0X1
of
Oxford
UK
3PS,
ABSTRACT
Motivated by the inability of current drug treatment to provide long-term benefit to HIVinfected individuals,
we
derive
HIV
therapeutic strategies by formulating and analyzing a
mathematical control problem. The model tracks the dynamics of uninfected and infected
CD4 +
cells
and
free virus,
in time, several different
and allows the virus
to
mutate into various
strains.
At each point
therapeutic options are available, where each option corresponds
to a combination of reverse transcriptase inhibitors.
current status and chooses
among
minimize" the total viral load.
Our
The
controller observes the individual's
the therapeutic options in a dynamic fashion in order to
initial
numerical results suggest that dynamic therapies
have the potential to significantly outperform the static protocols that are currently
in use;
by anticipating and responding to the disease progression, the dynamic strategy reduces the
total free virus, increases the uninfected
CD4 +
count, and delays the emergence of drug-
resistant strains.
December 1995
Submitted to Journal of Theoretical Biology
Introduction
1.
Optimal treatment of the human immunodeficiency virus of type
the subject of intense research activity. Rapid progress has been
and testing of anti-HIV therapeutic agents, resulting
Administration of
five reverse transcriptase
in
in viral
made
(HIV) infection
in the
is
development
the approval by the Food and Drug
(RT) inhibitors (AZT. ddl, ddC, d4T, 3TC) and
one protease inhibitor (saquinavir). These potent drugs inhibit
a rapid decline
1
viral replication
and lead to
abundance, often within days after starting therapy. Unfortunately,
these drugs have had only limited success in delaying the onset of AIDS: continual viral
replication of
DNA.
HIV, together with the high error rate of reverse transcription of viral
leads to the
emergence of drug-resistant virus
strains, typically within
(depending upon the drug) of treatment initiation (McLeod
aL.
1993; Volberding ef aL.
1994:
Wei
et a/..
multidrug resistance has been documented
1993;
Richman
et ah. 1994;
of protease inhibitors
in
1995;
Schuurman
combinations of
Shafer et aL. 1994, 1995; Kojima
(Condra
et aL.
shown that the AZT-3TC combination
& Hammer.
RT
into
weeks or months
199*2;
1995).
Lagakos
et
Moreover,
inhibitors (Larder et aL.
et ai.,
1995). although Larder et
is
et aL.
RNA
1995) and combinations
a!.
(1995) have recently
able to sustain in vivo antiviral effects for at least
24 weeks.
It
would appear that increased effectiveness of HIV therapy could be achieved by
developing dynamic multidrug approaches, where the combination of drugs received by a
patient changes over time in response to the disease progression (e.g., current
viral load,
mix
of viral strains). In this paper
C4 +
count,
we mathematically model the dynamic multiple
drug therapy problem as an optimal control problem that can be informally described as
follows:
choose an optimal mix of drugs
viral load over
regimen.
some time horizon
(e.g..
at
each point in time in order to minimize the total
one year) subject to a toxicity constraint on the drug
Several mathematical models have been developed that incorporate the effects of ther-
apy on an HIV-infected individuals. In a
1993; Kirschner
&
series of
Perelson, 1994; Kirschner
papers (Perelson, 1989; Perelson
& Webb,
et al.,
1995a; Kirschner et al, 1995), Perelson
and Kirschner and their colleagues have studied the timing, frequency and intensity of
AZT
treatment. Agur (1989) focuses on the optimal tradeoff between the toxicity and efficacy of
AZT. The mathematical models considered
Nowak
et al. (1901),
and Kirschner
McLean t Nowak
& Webb
in these studies
(1992),
do not allow
Nowak k May
for virus
(1993), Frost
mutation.
k McLean
(1994)
(1995b) analyze descriptive (as opposed to optimization) models for
the competitive interaction of AZT-sensitive and AZT-resistant strains of HIV; the latter
three papers also include numerical simulations of alternating and/or combination therapies.
Our
deterministic control problem, which
number
of virus strains, or quasispecies,
A
number
finite
is
described in Section
of therapeutic options are allowed,
RT
CD4 +
and infectious
and infected
strain; in this context, the
uninfected
CD4 +
CD4 +
RT
cells
where each option consists of the
inhibitors.
The model
si-
incorporates uninfected
free virus associated
with each virus
inhibitors prevent the free virus from successfully infecting
Each drug option has a
cells.
considers a finite
and allows mutations from one strain to another.
multaneous application of one or more
T-cells,
2,
different efficacy against each virus strain,
thereby allowing for complex drug-virus interactions.
Because of the high dimensionality of the control problem, we resort to approximation
methods
in
Section
more
3;
specifically,
perturbation methods and the policy improvement
algorithm are used to derive a closed form dynamic policy. Several other types of therapeutic
approaches, such as protease inhibitors and the reconstitution of the
considered in Section
discussed in Section
4.
6.
immune
system, are
Results from numerical simulations are reported in Section 5 and
Concluding remarks can be found
in Section 7.
.
2.
Problem Formulation
Our mathematical model incorporates
be the density of
yi(t)
CD4 +
If
we
by strain
cells infected
density of infectious free virus of strain
t
is
time
at
i
and
r,
=
i
1.
let u,-(£)
.
.
.
,
/, let
denote the
noninfectious virions are ignored in our model.
i;
define x(t) to be the density of uninfected
the system at time
HIV. For
/ different strains of
given by (x(t), yi(t),
.
.
,
CD4 +
cells at
yi(t), V\{t),
.
.
.
,
time
vj(t)),
t,
then the state of
which
denoted by
is
(x(t). yi (t).v (t)).
t
The
controller has
RT
inhibitors.
=
2 might be
a combination of
and combination
is
'
j
the amount of option
infectivity rate,
J therapeutic options
denoted by
3,.
efficacy of
which
manner.
drug combination j
drug policy
of pji
strain
dj(t),
and the
is
1
t,
where each option corresponds to
might represent
AZT. ddC and d4T. Our
assume that each
For
i
the infectivity of virus
it
i
=
is
The RT
=
—
1,...,J,
J2j Pj>dj{t)]:
CD4 +
cells;
own
the
inhibitors reduce virus
infections by virus strain
$i[l
used with ddl
virus strain has its
infects uninfected
1....,/ and j
new
AZT
control variables are dj(t). which
the next section.
in
blocking
in
We
t.
the rate that
is
reason for the "tilde" will become clear
infectivity in the following
=
For example, j
to use at time
j
time
at
let
i.
we assume
p3
i
denote the
Under a generic
that the values
toxicity parameters in equation (4) are chosen so that the infectivity of each
nonnegative under
The dynamics
of our
all
feasible therapeutic strategies.
system are described by the following
set of
ordinary differential
equations:
x(t)
=
A
-
(f,
+
£
ft«j(0[l
>=1
m
di(*)])*(*).
X>*
=
.7
(1)
1
J
=
(E
9wW*)[i - E/wM')Lk>) -
b i {t)
rate at which uninfected
o.-y.-(*),
(
2)
3=1
fc=l
The
-
=
CD4 +
ir i
yi (t)-[ki
cells
+ Pix(t)]v (t).
(3)
i
are invaded by virus strain
i
at
time
t
is
$
t
v (t).r(t
l
).
and each of these potential infections leads to a reduction
infections by strain
is /?,-[l
i
— Z)j =]
decline in uninfected cells x(t)
is
j.
rise in infected cells y,(i).
the fraction of reverse transcriptions of strain
Hence, J2j=i
=
<7«j
CD4 +
interpretation
infected
cell.
cell,
is
Tr t
free virus of strain
is
Clair et
qi 3
and
cell
rate gt j in (2)
infected by strain
replicates at rate
7rj
a/.
at rate
lytic burst
7T,-y,-(i);
7r,
after
it
in
has
an alternative
during the death of an
can capture a wide range of drug-virus
and antagonistic
(1991) and Larder ef
a/.
i
produced
t
Notice that the quantities pJt-,
St.
i
/a virions are produced by a
interactions, including both synergistic
observed by
that result in a
i
terms are nearly zero. Strain
and thus
that
The mutation
an d the diagonal terms of the mutation matrix are close to one
1
value, while the off-diagonal
infected a
rate of successful
and these infections cause a simultaneous
Pjidj(t)]vi(t)x(t),
and
The
in free virus.
combination therapy, as
effects of
(1995), and surveyed by Wilson
and
Hirsch (1995).
Uninfected
CD4 +
compartments
tissue
pool of precursors
A.
In addition,
CD4 +
(e.g.,
(e.g.,
we
cells, cells
cells
let
increase because of (exponential) proliferation in peripheral
secondary lymphoid organs) and/or (linear) production from a
the thymus). For simplicity,
[t,
a and k denote the respective natural death
t
t
infected by strain
Because the primary focus of
i
and
this
free virus of strain
paper
is
rate
rates of uninfected
i.
on therapeutic regimens and not on natural
human immune response
into the
Hence, the mutants are assumed to escape from the drugs, not from the
immune
disease progression,
model.
we assume a constant production
response.
we purposely do not incorporate
The model
from actively infected
infected cells are
not incorporate
the
also ignores latently infected cells; although
cells
(Ho
unimportant
et ai, 1995;
for the
new data from Shaw
location of considerable production of
Wei
et a/.), this
emergence of drug
most plasma virus comes
does not imply that latently
resistance. Finally, our
(1995). which suggests that the
plasma virus and many new
model does
lymph system
infections.
is
the
We
impose the toxicity and nonnegativity constraints
£^(0<i.
3
>
dj(t)
where t3
is
constant over time (and
is
is
taken to be unity, without
assumption
adapted to the more
in (4)
is
j.
is
However, because the
one therapeutic option at each point
innocuous. Moreover, the dynamic policy can be
realistic setting
where the
months
toxicity threshold
of intense therapy
of light therapy) or the severity of the patient's side effects:
drug combination dictated by the index policy
in time,
loss of generality).
typically use only
specified function of either time (e.g.. six
months
(5)
additive across drugs, and that the toxicity threshold
emerge from our analysis
in time, the additivity
easily
0.
a (normalized) measure of the toxicity per unit time of drug combination
Hence, we assume that toxicity
policies that
(4)
=1
in the
is
is
an exogenously
alternated with six
we propose
that the
next section be employed at each point
but the dosage should be altered accordingly.
Let
T
be the time horizon. Then the mathematical control problem
controls {dj(t),t
>
is
to choose the
0} to minimize
T
L
5>(*)d
(6)
t=l
subject to (l)-(5).
Our
control problem assumes that the decision maker, in choosing dj(t) at time
observe the current state (x(t),y (t).v
l
to quantify virus load,
CD4 +
cell
l
{t)).
Although recent technology makes
counts and virus-infected
cells in
it
lymph system
is
the blood of infected
Moreover, quantification of virus load and infected
even more complicated.
A more
realistic control
can
possible
individuals, these techniques are not currently available for day-to-day treatment of
infected patients at large.
t,
problem
HIV-
cells in
the
for current day-to-
day treatment would allow the controller to see only a partial observation of the state
(e.g.,
only the total
problem
CD4 +
count x(t)
(l)-(6) then
+
YlUi
an ^ the
Vi(t)
becomes a nonlinear
filtering
greatly complicate the problem, reasonably
on page 161 of
Elliott,
good
^
total vir
(x(t),yi(t),Vi(t)} at
time
control
derived.
Kalman
filter
However, because we
dynamic multidrug therapies,
Analysis
control problem (l)-(6) does not appear to admit a closed form solution. More-
ai. 1962) cannot solve a
problem of
on Pontryagin's
maximum
principle (Pontrvagin
drug options and 30 virus
realistic size (e.g., five
Hence, we resort to an approximate method, which employs perturbation methods
strains).
in
The
t.
over, standard numerical techniques based
ct
';(0)-
and hereafter assume that the controller can observe
3.
The
l
policies (e.g., the linearized
Aggoun and Morse, 1994) can be
this line of inquiry
Hi=i
problem; although partial observations
are primarily interested in the potential value of employing
we do not pursue
l° a<i
conjunction with ideas from dynamic programming.
3.1.
time
t
Overview.
to time
(x,yi,Vi).
T
Let V(x.y .v
t
t
,t)
denote the cost incurred (as given
under the optimal policy, given that the state of the system
V
For ease of notation, we suppress the dependence of
the dynamic programming optimality equation
dv
+
f
<
its
at
from
time
t
is
arguments. Then
(Bellman. 1957)
f^dv,
'
„
.
.
,\
dV
mm - —
{^GfJ}l
.
is
on
in (6))
7
d.r
1=1
J=l
j
J
(<)
j=\
fc=l
where
Q
follows:
denotes the set of admissible controls that satisfy (4)-(5).
we use asymptotic methods
to obtain closed
Our
basic approach
form approximate expressions
(2I+l)-dimensional process {(x(t),yi(t),Vi(t)} under a static control policy
6
(i.e.,
is
as
for the
dj(t)
=
d3
for all t).
From these
same interpretation
expressions,
as the
V
in (7),
policy, not the
optimal policy.
(Howard. 1960)
is
derive
a.
closed form expression for
except that the (approximate) cost
Then one
iteration of the policy
is
V
which has the
under the
static
improvement algorithm
V
performed: we differentiate our approximate closed form expression for
with respect to x and y
the
we
t
.
substitute these derivatives into the right side of (7) and perform
embedded minimization
in this equation.
This approach yields a closed form dynamic drug control policy:
it
specifies
how much
of each drug combination to use at each point in time in terms of the current state, the
current time, and
exact, then
all
the problem parameters.
If
our closed form expression
for
V
was
dynamic programming theory would imply that our proposed policy was better
(yields a lower cost in
(6))
than the static policy
fact,
(in
if
our expression
for
I'
was
exact then repeated policy improvement iterations would generate a sequence of policies
that converges to the optimal policy). However, our expression
draw
this conclusion.
is
not exact, and
we cannot
V
Nevertheless, this philosophy (finding an approximate value for
and performing one iteration of the policy improvement algorithm) has been used with
considerable success in designing dynamic call acceptance/rejection protocols for stochastic
models of telephone
3.2.
traffic (e.g.,
The Optimal
is
Because our proposed dynamic policy takes a
Static Policy.
static policy as its starting point,
optimization problem
Ott and Krishnan, 1985; Key. 1990).
it
is
natural to employ the optimal static policy.
The
static
given by the following nonlinear program:
r
minimize,..,,,.,,,.^
^=
!
bject
to
A -(fi
+ Yl &«i[l " EM;])-r =
i=i
(E q*hvk[l
(8)
v,
1
°-
(
9)
j=i
-J^Pjkdifjx - a iyi =
0.
(10)
j=i
fc=i
TT.-t/i
-
[ki
+ 0iX]Vi = 0,
(11)
We
£^<1,
(12)
dj>0.
(13)
have been unable to find a closed form solution to (8)-(13); however, standard numerical
techniques
(e.g.,
straint (12)
is
Avriel.
solved by direct enumeration of
J+
all
infectivity of virus
is
i
/^ J,,
where d
t
=
Asymptotic Analysis.
1
—
the additivity con-
=
or tJ
for all j;
feasible solutions.
1
Under
Let d* denote the optimal static policy that solves (8)-( 13).
3.3.
If
not realistic then one can change constraint (13) to d3
new problem can be
this
1976) can be used to solve this problem.
this policy, the
J2j=i Pji^j-
we
In this subsection
find a closed
form approximate
expression for the system trajectory under the optimal static policy. Consider equations
(3).
with
J,
taking the place of
1
— 5l/=i
Keeping
Pjidj(t).
in
mind
that
we
will
( 1
use the solul ion
to these equations to derive V. let us consider the initial conditions (in this subsection, s
a generic time index and
t
denotes a specific point
x(t)
=
To perform the perturbation
generality, let us
assume that
@\
=
x,
=
yi{t)
analysis,
Vi{t)
yi
j3 t
.
=
Vi
(14)
.
Then we
let e
=
/?i
e.
Without
loss of
and define
-
=
is
time)
we introduce the parameter
rnin{i<,<j}
&,
in
)-
(15)
f
Although 0!
=
1,
we
The asymptotic
10
analysis
than one). Typical values
less
-5
;
parameter
retain this
is
in
the model.
based on the assumption that
e is
small in value
the infectivity parameter
in the literature for
$
(i.e.,
much
are roughly
hence, the approximation should perform well.
We
x(s)
assume that our solution
= X M(s) +
ex^(s).
is
y> (s)
of the form:
=
0)
y\
(s)
+
8
ey
{
t
l
\s).
Vi (s)
-
0)
v\
(s)
+
1
er' '^).
(16)
Although we could define and solve
is
for higher order terms, just deriving the first order
We
quite cumbersome, at least without a computer.
use (15) to replace
use (16) to substitute in for the system state in equations (l)-(3) and (14).
we
collect
terms of order
Collecting the constant
e'
unknown
to solve for the
(3 t
by
For
i
terms
e/? t
and
=
0,1.
processes on the right side of (16).
terms yields the following system of differential equations:
(i.e., e°)
= \-iix {0] {s).
x {0) (s)
0)
y\
ii°\s)
=
0)
=
(s)
nyl
(17)
-
0)
(3)
(is)
(s),
-*iy\
kiV^is),
(19)
subject to the initial conditions
=
,-<°>(0
It is
y\°\t)
.r.
=
y
$\t) =
t
»,
(20)
worth noting that the mathematically perturbed system (17)-(20) corresponds precisely
to the physical perturbation performed
use data from Wei
et ai.,
Ho
et al.
when
RT
giving potent
and Perelson
et al.
who used
(1995),
and protease inhibitors to perturb the system, to estimate values
The
solution to equations (17)-(20)
z
(o)(
3)
=A+
The order
e
=
(
x
_
t
A) e -M(.-*)
ai{
Vi*-
= JEiW_ e -a,(.^) +
—
k
various
for the
RT
inhibitors
model parameters.
is
V?\s)
„<*»(,)
we
inhibitors. In Section 4,
{v
.
(21)
)
~\
t
_
J™_
—
k
a,
(22)
t
)e -M*-*).
(23 )
a;
terms lead to the following system of differential equations:
I
x(%) = - M xW( a )-x(°>( a )j:M»} 0) (-)i
i)
»}
(-)=x (o, (*)(x:««A^f (*))- a *»i 1) (*).
(
24 )
(
25 )
,
9
riy l%)
=
v\'\s)
- kivPia) -
i3 t
x^(s)vl
0)
(s).
(26)
subject to the initial conditions
1)
.r<
Now we
tially.
The
solution
is
yV(t)
0,
=
=
1)
u{
(i)
0.
(27)
given in Appendix A.
The Proposed Dynamic
tems (17)-(20) and (24)-(27)
(s))ds. This integration
simplified
tice,
=
substitute the solution (21)-(23) into (24)-(26) and solve equations (24)-(27) sequen-
3.4.
ev\
(0
if
T
is
carried out in
is
very large
(i.e..
function (and hence a policy) that
is
is
t
The proposed
B.
in years) in relation to
T =
set
V by J
5Zf_ 1 (f,-
solution
(Ho
Wei
ef al..
oc and
=
/
in
denoted by
V
c
.
to distinguish
t
In prac-
the time scale of the
et a/.): hence, this
%
Now we
Ctiki
Wij3
.
'
/_^_ +
\otikiH
it
from the value function
the (at most J
+
1)
is
a
T=
oo and
t
=
in (7).
0)
(ai
x
~
+
fi)(ki
A //'
+
y- Mil -
\ (j.
fi)J
I
'
J=l
otjkj
(28)
-
(29)
Ja
can substitute these derivatives into (7) and perform the minimization.
cause the function to be minimized
is
(46) to obtain a value
WctUt^-l)!*)^^),
e
+
independent of the time horizon; this approximate,
is
Differentiating (46) with respect to x and y yields (with
+
{s)
greatly
is
independent of the time horizon.
a daily basis
Consequently, we
stationary value function
Appendix
value function
systems dynamics, which change on
natural assumption.
solution to the asymptotic sys-
hand, we can estimate the value function
in
we assume that the
the time horizon
With the
Policy.
linear in
our controls
extreme points of the constraint
set (4)-(5),
form. Let us define the dynamic quantities
I
Ci{t)
= 0Mt)
7=1
10
dj(t),
Cilk'i
the solution d*(t)
and can be found
is
Be-
one of
in closed
/
Ki quel,
^
y.
_ J_
";A,
*jqijdi
\ /
ajkj
'\
^
fc,
Then the proposed
policy
+
7T/[^A(Qf
+
A-;
ctiki(cu
apply no therapy
is:
// )
+
-
Ay (?,/.; (Q
y (0]
f
_
(i.e.,
d^(t)
<
=
f
v(Q
\
k + (i'
t
for j
=
J)
1
(30)
if
(31)
0:
Tj
d".(t)
(i.e..
=
t~,
,
d~(t)
=
for j
= argmax^^^jj eLiPj.-c»(0
j
We
f
+ fi)(k + (i)
max
{l<j<J}
otherwise, use drug combination j'
Q
^
j"),
where
/
QO x
(32)
.
conclude this subsection with several remarks.
The proposed therapeutic strategy
j has the
dynamic index
is
H t=] PjiCi(t)/Tj,
a
dynamic index
and
at
policy,
each point in time the policy uses the drug
combination that possesses the largest index. The quantity
marginal increase
virus strain
i
at
in
the total future viral load
time
dynamic marginal
/.
The index
cost for each virus
for
where drug combination
if
we
c (t) essentially represents the
t
one more CI)4 +
let
drug combination j
is
by the efficiency of drug
cell get
infected by
computed by weighting the
j for that virus,
summing up
over the virus strains, and dividing by the drug combination's toxicity. Hence, our dynamic
policy uses information on the effectiveness of each drug against each virus, the current
potential cost (in terms of total future viral load) of a
new
infection by each virus strain,
and the toxicity of each drug combination, and summarizes
manner. An important advantage of index
.
policies
is
this
information
their ease of use:
the derivation and implementation of an index policy
is
in a succinct
the complexity of
independent of the problem
size;
hence, policy (30)-(32) can easily be derived for a problem with 20 drug combinations and
150 virus strains. Although this policy
is
not the optimal solution to problem (l)-(6). the
optimal solution to dynamic resource allocation problems
is
often characterized by index
policies (e.g.. Gittins. 1989).
Notice that
if
we took
e
=
in (30)
then the policy would be independent of x and
whereas the proposed policy depends on the entire (2/
11
-+-
?/,-,
l)-dimensional system state; this
suggests that incorporating only the e° terms leads to a rather crude policy. Also, one of the
drug combinations would always be administered
inequality (31) never holds)
(i.e.,
Inquality (31) was never satisfied in any of our numerical runs: the proposed
=
if e
0.
dynamic policy
always used one of the drug combinations.
It is
possible to implement further iterations of the policy
us denote the proposed policy in (30)-(32) by eQ
it
improvement algortihm. Let
although this control
(t);
can be expressed solely as a function of time because the system
define d
=
(t)
t
—
1
state-dependent,
deterministic.
we
If
then this quantity can be used as our starting policy
\t)
J2j=iPjidj
is
is
next policy improvement iteration. Turning to the asymptotic analysis, we observe
for the
that the e°-order system (17)-(20) and
If
we substitute
is
still
d]
(t)
in for
d
t
in
its
solution (21)-(23) are independent of the control.
equations (24)-(25). then the eorder system (24)-(27)
a set of linear differential equations thai can be easily solved numerically using the
matrix exponential (Golub and Van Loan. 1989). Then we can carry out the calculations
Appendix B and equations (28)-(29) on a computer, and perform the minimization
to get a
also
new
policy d
}
(t).
Of
in (7)
course, higher order terms in the asymptoic expansion can
be performed relatively easily with a computer, and
it is
conceivable that, with enough
higher order terms and enough policy iterations (typically, only a handful of the latter
required to get close to optimality). such a procedure would generate a policy that
close to optimal.
in
However, because the proposed policy
in (30)-(32)
is
performed well
in
is
very
our
numerical study, we have not pursued this computational approach.
3.5.
A
Symmetric Case.
To gain a better understanding
we
focus on the symmetric case where I
Ptj
—
p
for
i
^
strain has the
strain
i.
j
(where p
>
p), q n
same parameter
Also, let y
=
Y.\=\ Vi
—
q
values,
and
v
=
=
and
and
=
J, a,
q,j
for
£)f=1 v
=
t
(I
=
i
a, k
1,
—
.
t
=
q)/(I
.
,
.
/,
k,
—
7r t
=
of the proposed policy,
7r,
1) for
i
/?,•
/
=
j.
/?,
Tj
=
1,
=
p,
Hence, each virus
drug combination
i
is
targeted at
denote the total number of infected
12
pn
cells
and
Symmetry arguments imply
the total free virus, respectively.
extreme point
static
j
and
t,
or d3 {t)
=
policies
1/7 for
efficacy" of the static
the second policy.
and
#
is
dj(t)
=
1/7
all j
and
>
if
t
(<--
1
— p
zero for the
is
for all
so): dj(t)
where p
i.
policy and
first
the one minimizing (8))
(i.e.,
[p
is
is
for all
the "average
{I
—
dj(t)
=
+
=
1
)p]/I for
<
if
where
0.
k
iTii
+
a
Then d =
t.
best static policy
airy
//(A-- q;
optimal (although perhaps not uniquely
drug policy, which
The
—
=
is
that one of the two symmetric
Jf
—
r— -)(—
a
oq
r-
A
x--
-
A
A'
(q
/'
+
/.i)(k
—
a)
+ (v--, k
)-
a k
+
fi.
(33)
The
solution in the symmetric case reduces to:
r-(.r-y)>——
~
if 7r(
1
—
p)
< a
p[?r(
then apply no treatment
Q
+
~
/'
p)
—
then apply no drugs
+
if
(34)
;
ak
a\
+ //)(fc + /x) +
r-(r-«/) < ^7—
/3|_3r
Otherwise administer drug combination
-
—
— p) > a
if
(a
,
1
If 7r( 1
/*,
(_
1
—
p)
where
—
A(q
+
A-
+
/0
r
v~(t)
(35)
•
aj
qA'
>
Uj(f) for
?
=
1.
.... 7.
Hence, the proposed policy in the symmetric case always applies the drug combination
This therapeutic strategy certainly seems
that corresponds to the most prevalent virus.
reasonable, although not obvious nor necessarily optimal. Also, the drug/no drug decision
in (34)-(35)
depends only on the relative value of the amount of
between the number of uninfected and infected
cells.
the drug/no drug decision) in three dimensions
as a straight line in
and the difference
Hence, the "switching curve" (between
x, y
and
v)
can actually be expressed
two dimensions.
4.
The
(i.e..
free virus v
Alternative Therapies
tedious part of the analysis in Section 3
is
the perturbation analysis that leads to
the derivatives of the value function for a generic static policy.
13
Now
that these derivatives
have been estimated,
it
a relatively simple matter to consider other types of therapies.
is
Here are two examples; much of the previous notation
Protease Inhibitors. Protease
is
reused.
inhibitors render newly produced virions non-infectious.
Suppose we have J combinations of protease inhibitors, and the controller must decide how
much
<
of each to use subject to II,=i Tjdj(t)
matrix pJn and the resulting virus replication rate
to that in Sectic;. 3 yields the
The
1-
is 7r t [l
drugs' effectiveness
— Y?i=\
Pjidj{t)].
is
An
given by the
analysis similar
dynamic index
E'"'**^*"
(36)
drug combination
for
At each point
j.
in time,
the combination with the largest index
administered. Note that
d
t
=
one
—
1
in
J2j=i Pjid*,
index
is
positive: otherwise,
no drugs are
should be positive, so therapy should always be applied. Define
'i^f-
where
this
if
the proposed therapeutic strategy uses
optimization problem that
dj solves the static
is
analogous to the
Section 3.2. Integrating the approximate value function in Appendix
B
with respect
to Vi gives
and substitution of
W.
1
dvi
ki
tA
ki(ki
it)
fegofe
[p ajkj
-iW-A).
this quantity into (36) yields the
problem parameters and the current
3.5,
+
state.
h)
(37)
v
proposed therapy
in
terms of the
For the symmetric case considered in Section
the solution in (36)-(37) employs the protease inhibitor combination that corresponds
to the largest value of y,{t) at each time
has infected the most
that
is,
the therapy targets the virus strain that
cells.
Reconstituting the
Immune System.
(IL-2), that reconstitutes the
immune
the production rate of uninfected
where our control
t;
A(r)
€
[0,A].
Consider using a drug, such as interleukin-2
system. This drug affects our model by increasing A,
CD4 +
cells.
Suppose the new production rate
Then the optimization problem embedded
14
is
in the
A
+
A(i),
dynamic
programming optimality equation
simply to minimize A«-. The proposed policy
is
\*(t)
and
X*(t)
=
otherwise, where
4^
=
\
if
^<0.
ox
(38)
given in equation (28) (with d
is
is
t
=
Define the
1).
constants
*=
>
If c t
drug;
for all
i
£*?-!-•
then we never use the drug, and
neither of these cases hold then a
if
the right side of (39)
is
if c,
(»)
<
dynamic policy
for all
is
~,
if
> a
(that
.
is,
and so
this
course, our
cell will
7r t
>
a,;
always given
I\\,"
first
quantity on
)
value of
nearly equal to ^/(q^A:,),
and only
if 7r £
-
>
a, for all
i.
If
than unity
free virus particle during its lifetime),
fuel to the fire".
hence, adding uninfected
if
is
for the infected cells is greater
produce more than one
drug effectively "adds more
suggest that
some
is
then the "basic reproductive ratio
each infected
The
the expected (with respect to the mutation probabilities q tJ
we ignore mutations then the drug
t
then we always use the
optimal.
w/(ak). Since the mutation rates are very small, this quantity
and
i
CD4 +
Empirical results (see Section 5)
cells in isolation is
not desirable; of
model has not incorporated an immune response, and thus may be omitting
positive side effects of additional
analysis can
be performed
for a
CD4 +
cells.
Although we do not do so here, a similar
therapy that reduces
CD4 +
cell
production.
Other therapies that can be analyzed include certain forms of immunotherapy (which
would increase the death rate of
CD4 +
expansion of
decrease
y;,
cells
(Wilson
free virus
et al.,
and/or the death rate of infected
cells),
ex vivo
1995). which would simultaneously increase x
and dynamic gene therapy (Nabel, 1994), which would increase
i\
and
for certain
strains.
Most importantly, we can
also consider
ously, with a joint toxicity constraint.
RT
inhibitors
and production of
CD4 +
employing some of these therapies simultane-
For example,
cells
if
(Schwartz
15
one allowed the simidtaneous use of
et a/., 1991),
it
may
turn out to be
beneficial to introduce
CD4 +
when the
times
cells at
infectivity of the virus
and the
viral
load are sufficiently suppressed.
An
5.
In this section, the
under several simpler
rather,
we
dynamic model
policies.
Example
Illustrative
is
simulated under the proposed policy, as well as
No attempt has been made
to generate a
model
of realistic size;
consider only two virus strains and two drug combinations in order to illustrate
the nature and the impact of dynamic drug treatment. In a subsequent study,
use data from multidrug clinical
Parameter Values.
5.1.
Table
1.
a
Ho
et
al.
and Wei
per day. About
model are displayed
in
analyze larger models.
The parameter
2%
estimate a
et al.
of the total
cells/mm 3 per day. The death rate
equilibrium
CD4 +
contains roughly 5 x 10 6
human body
for
to
values for our
Most of these values were sequentially derived from existing data
manner.
cells
trials to
we plan
CD4 +
count
is
A///
=
//
mm
CD4 +
in the following
production rale of roughly
1.8
x 10 9
population resides in the peripheral blood, and
3
.
Hence, the 1.8 x 10 9 figure
is
comparable
to 7
was chosen to be 0.007 per day, so that the virus-free
1000
cells
per
mm
3
,
which corresponds to the
CD4 +
count
an uninfected individual.
Now we
Wei
et al.
turn to the death rates a, of infected
cells
estimate the death rate of virus-producing
recentby. using
more accurate data. Perelson
et al.
and
cells to
A*;
of free virus.
Ho
et al.
and
be about 0.35 per day. More
(1995) show that the
about 0.49. They were also able to get a rough estimate of 3.07
mean death
for the
rate
is
death rate of free
virus.
Some
of the remaining
parameters are derived by considering the quasi-steady state
conditions before drug treatment. For typical pre-treatment values,
(over 20 individuals) in Table
1
of
Ho
et a/.;
we use the average
the average pre-treatment
16
CD4 +
values
count was 180
mm
per
cells
3
and the average
was present
virus
in
mm
was 134 virions per
viral load
3
Only the wild-type
.
we can
nonnegligible amounts before treatment. Hence,
the wild-type virus, and set the
consider only
side of equations (l)-(3) equal to zero (reflecting the
left
+
quasi-steady state) to obtain a set of four equations (equations (l)-(3) and x
and four unknowns: the pre-treatment number of uninfected
infectivity rate
J3
and the replication rate
solving these two equations for
mm
3
per
mm 3
per day and y
,
=
J3
180/)i>/(a
and the fraction of
cells
agreement with the estimate of
for
yields k
7r
=
v(k
+ 0x)/y —
produced by an infected
is
produced
and
cell in
+
Substituting 180
K.
y yields
fSv)
=
=
J3
(aX
found
is
y/(x
Embretson
in
-
y for x in (1)
180a/i)/(lS0m>
11.86 cells per
that are infected
5%
—
x and infected
cells
mm
+
et al.
3
y)
=
in
and
(2)
168.14
is
-4
cells
in close
Finally, solving (3)
(1993).
Readers should keep
the
2.58 x 10
0.066, which
=
35.18 virions per day, implying that tt/o
our model.
=
Hence, x
.
180)
cells y,
and
- \v) =
=
y
mind
71.8 virions are
that most virus
the lymph system, whereas our estimates for k and $ are based on plasma
in
concentrations.
We
10" 5
we
use the mutation rate calculated
We also
.
pn
let
=
assume that drug combination
P22
=
0.95 and p 12
=
P21
effective at blocking infections of its
=
own
not
is
dominant
AZT) RT
at
i
0.05.
is
(1995), q u
targeted at virus strain
i.
=
More
921
=
might
arise
if
5%
is
The
95%
effective at blocking infections
virus
1
is
an AZT-resistant strain
time zero, and the two drug combinations correspond to two other
inhibitors.
x
3.4
specifically,
meaning that each drug combination
strain, but only
of the other strain; such a state of affairs
that
Mansky and Temin
in
toxicity coefficients are set to t x
-
r2
=
1.
so that
if
(i.e.,
dj(t)
=
1
then the amount of drug combination j administered corresponds to the threshold toxicity
level.
Notice that, until now, the parameter values are consistent with the symmetric case
introduced in Section
3.5.
Now we
introduce asymmetry by letting n 2
17
=
0.9^!; hence,
we
assume that
state
virus
1
has a higher replication rate than virus
2.
was taken as the starting point of our simulation runs
Variabl<
The pre-treatment equilibrium
(see Table
1).
80
100
time (days)
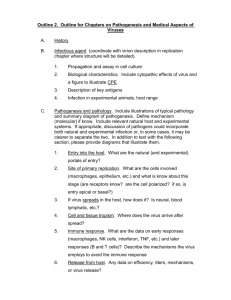
Figure
1.
System behavior under the dynamic
19
policy.
80
100
time (days)
Figure
2.
System behavior under the continuous treatment
20
policy.
the same quantities under the continuous treatment policy that continually applies drug
(i.e..
di(t)
=
l.d 2 (t)
=
for all
/).
Under both
were very similar, with the free virus
v
t
policies, the
shape of the
lagging behind the infected
cell
count
days; hence, the dynamics of the infected cells do not appear in Figures
simulated the model under the optimal static policy derived in Section
d
{
—
0.5-3,
d2
=
0.47.
Although we do not include figures
average (over one year) uninfected
policies are reported in Table 2.
CD4 +
for the
is
1
3.2;
and
y,
and
y,
curves
by several
2.
We
also
the solution was
optimal static policy, the
count and average total viral load for the various
Readers should note that the optimal static policy was
derived under the assumption that drug toxicities are additive;
valid then the static policy
v,
1
not a feasible alternative.
if
this
assumption
is
not
and
cells,
this
quantity peaks at three months; the peak corresponds to more than a three-
Not surprisingly, the dynamic policy
fold increase over the pre-treatment value.
treatment with drug
with drug
1
The
policy
first
week
at the
beginning of the second month) switches back and forth
1.
for over a
initiates
uses drug 2 on day 18, and irregularly
(e.g., it
stays
between the two drugs about once per day until the end of the third month. During the fourth
month, the two virus strains feed on the large pool of uninfected
emerge, peaking with a total viral load that
The drug treatment
roughly four times the pre-treatment
is
attempt to simultaneously control both viruses. The
the majority of
The
and
fifth
large viral load in turn leads to
CD4 +
count.
This reduction
more
in
viruses back under control during the fifth
(e.g.,
fit
virus
new steady
state
is
cell infections,
policy
expended more
effort
Continuous Treatment.
we again
to the
first
uninfected
cells
month. After
slowly reached. Over the
allocated 58.7% of the time to drug
and the uninfected
is
six
about 55%
this time, these oscillations
month with
first six
rise in
the
CD4 +
2:
hence, the dynamic
virus.
fit
in
Figure
the end of the month. This high viral load then drops the uninfected
which
in turn leads to a
2,
count; however, in contrast
policy, the continuous treatment policy suppresses virus
level,
dampen
a value of about
1
throughout the
months. Virus 2 emerges during the second month, and reaches a very high
pre-treatment
count
months, the dynamic policy
and 41.3% of the time to drug
and a linear
CD4 +
allows the drugs to bring both
Under the continuous treatment policy pictured
1
an
higher than the pre-treatment
than the optimal static policy on the more
see a rapid drop in virus
dynamic
1
in
1.
the total viral load peaks again at the end of the seventh
240) and a
month,
less fit virus 2 constitutes
decreases in the fourth month, bottoming out at a level that
uninfected
this
level.
months, and hence the dynamic policy exerts
more
controlling the
its effort in
and simultaneously
between the two options during
oscillates rapidly
of the free virus during the fourth
cells
CD4 +
level
by
count below
its
reduction of free virus 2 in the third month.
99
Comparison of
Table 2 shows that the dynamic policy performs much better
Policies.
than the continuous treatment policy:
in
average (over the
first six
months)
the continuous policy achieves a 17.4% reduction
viral load
and a 31.6% increase
in
CD4 +
uninfected
count with respect to the drug-free equilibrium, whereas the dynamic policy achieves a
53.4% reduction
peaks and
viral
in viral load
CD4 +
and 126.2% increase
valleys are less
in uninfected
CD4 +
count. Moreover, the
pronounced under the dynamic policy than under the
continuous treatment policy. Finally, the dynamic policy, by frequently switching between
the two drug options during the early months, delays the emergence of virus 2 from the
second month until the fourth month. Although the results are not reported here, we also
tested an alternating policy that uses drug
2 for the last three
We
and
for the first three
1
months. Not surprisingly,
months and then uses drug
this policy did not
perform
well.
should note that the post-treatment steady state values of uninfected
under
total virus load
CD4 +
cells
of the therapeutic strategies are not appreciably different
all
than the pre-treatment steady state values; hence, the therapeutic benefits in our model
are achieved during the transient domain.
individuals undergoing
for
many
However, the
years. Therefore, the
improvements over the transient domain
Unequal Infectivity Hates.
0.9/?i-
The
in
our model should
in clinical practice.
Because there seems to be some uncertainty about whether
virus strains have different infectivity rates,
=
of HIV-infected
dynamic drug treatment would probably exhibit transient behavior
be indicative of the improvements that can be realized
02
dynamics
viral
we reduced
the infectivity of virus 2 so that
qualitative results were similar to our base case, although the
policy expended a slightly larger fraction of
its effort
larger proportion of virus 2 in the viral mix.
More
runs were generated by varying the parameters
7r £-,
displayed in Figures
1
and 2 remained
on virus
resulting in a
somewhat
numerous other simulation
generally,
$, A and p (J and the qualitative
intact; hence, the
23
1,
dynamic
,
model appears
to
results
be robust.
7.
We
Conclusions
have used the control theory paradigm
HIV
in a
Our model
therapeutic setting.
incorporates different virus strains, and a variety of therapeutic options are available.
The
approximation method, which uses perturbation analysis and the policy improvement
gorithm, gives rise to a dynamic index policy:
dynamic index, and
largest index.
each drug combination has an associated
drug combination with the
at each point in time the policy uses the
The dynamic
indices succinctly
al-
summarize three
quantities:
the efficacy of
each drug combination on each virus strain, the toxicity of each drug combination, and the
marginal benefit of blocking a new
cell infection
by each virus
strain; the last of these three
quantities changes over time as a function of an individual's
viral
count, viral load and
mix.
Numerical results
for a two- virus,
two-drug model suggest that dynamic multidrug ther-
apies outperform their static counterparts:
CD4 +
count
is
increased,
the total viral load
and the emergence of drug
the individualized therapy that we propose
is
reduced, the uninfected
in anticipation of
delayed. Although
difficult to
may outweigh
implement than
the costs of implemen-
allowing the less
fit
more
fit
realistic
response
virus strains at a relatively low level, while perhaps
strains to partially establish themselves.
Although our numerical results focus on the two- virus, two-drug
more
in
the emergence of drug-resistant strains. In addition, the dynamic
policy attempts to maintain the
of
is
These benefits are achieved by frequently changing therapies over time
tation.
and
is
resistant strains
no doubt more
protocols that are currently in practice, the benefits
to
CD4 +
models using data from multidrug studies
turn out that the best way to delay the onset of
AIDS
is
is
planned
case, the
for the future.
etc.).
The model and
24
It
may
via the intelligent use of a wide
range of therapies (RT inhibitors, protease inhibitors, reconstitution of the
immunotherapy, gene therapy,
development
immune
system,
analysis presented here provides the
framework
for the
Finally, our
development of such therapeutic
approach to
this
strategies.
problem circumvents the usual obstacles inherent
ing high-dimensional nonlinear control problems.
in solv-
This method, which appears to be new,
has potential applications in a wide variety of control problems in epidemiology and ecology:
besides allowing for mutation
among
multiple variants of entities (in this case, viruses), the
approach can also incorporate discrete age classes
and discrete
(e.g., for
spatial (e.g.. lattice) structures (e.g., for
optimal vaccinations of measles)
dynamic control
of spatial epidemics).
Acknowledgment
The
He
first
author was supported by
NSF grant DDM-9057297 and EPSRC
grant GR/J71786.
gratefully acknowledges a valuable discussion with Peter Whittle during the early course
ol this research,
estimation.
and thanks Denise Kirschner
for a helpful
The second author was supported by
25
conversation about parameter
the Wellcome Trust and Keble College.
REFERENCES
Agur.
A new method
(1989).
Z.
for
Biomedical Modeling and Simulation. Levine, D.
IMACS.
lishing Co.
Avriel,
AZT.
reducing cytotoxicity of the anti-AIDS drug
S., ed., J.
C. Baltzer
AG,
Scientific
Pub-
59-61.
M. (1976). Nonlinear Programming. Prentice- Hall, Englewood
Cliffs,
NJ.
Bellman, R. E. (1957). Dynamic Programming. Princeton U. Press, Princeton, NJ.
Condra.
H.
J.
et
In vivo
(1995).
al.
emergence of HIV-1 variants resistant to multiple
protease inhibitors. Nature 374, 569-571.
Elliott, R. J.,
Aggoun,
L.
Control. Springer- Verlag.
Embretson.
and Moore,
New
B. (1994).
J.
York.
(1993). Analysis of
J. ef al.
Hidden Markov Models: Estimation and
human immunodeficiency
virus-infected tissues by
amplification and in situ hybridization reveals latent and permissive infections at single-cell
resolution. Pvoc. Natl. Acad. Sci.
Frost, S. D.
W. and McLean,
USA
90, 357-361.
A. R. (1994).
Quasispecies dynamics and the emergence of
drug resistance during zidovudine therapy of HIV infection.
Gittins, J. C. (1989).
AIDS
8. 323-332.
Multi-armed Bandit Allocation Indices. Wiley,
New
York.
Golub. G. H. and Van Loan, C. F. (1989). Matrix Computations. Johns Hopkins U. Press,
Baltimore.
Ho. D. D.
infection.
et al.
(1995).
lymphocytes
in
HIV-1
Dynamic Programming and Markov
Processes.
MIT
Press,
Cam-
MA.
Key. P. B. (1990).
Inf.
CD4
Nature 373, 123-127.
Howard, R. A. (1960).
bridge,
Rapid turnover of plasma virions and
Sci.
Optimal control and trunk reservation
in loss networks.
Prob.
Engrg.
4. 203-242.
Kirschner. D., Lenhart. S. and Serbin.
S.
(1995).
Optimal control of the chemotherapy of
HIV. Preprint, Dept. of Math., U. of Tennessee, Knoxville, TN.
Kirschner. D. and Perelson. A. (1994).
AZT
treatment studies.
A model
for the
immune system
Mathematical Populations Dynamics
26
III,
response to HIV:
Theory of Epidemics.
Arino. 0.. Axelrod, D. and Kimmcl. M.. eds.,
Kirschner, D. and
of
AIDS. Submitted
Kirschner. D. and
in
Webb. G.
A model
for
Publ..
Winn. Manitoba.
treatment strategy
in
the chemotherapy
Math. Biology.
to Bull.
Webb. G.
the treatment of
F. (1995a).
Wuerz
1.
drug resistance
F. (1995b). Effects of
HIV infection.
in
Preprint, Dept. of Math.. Texas
chemotherapy strategies
A&M
U.. College Station.
TX.
Kojima. E.
ef al.
Human
(1995).
immunodeficiency virus type
and development of drug- related mutations
1
(HIV-1) viremia changes
with symptomatic HIV-1 infection
in patients
receiving alternating or simultaneous zidovudine and didanosine therapy.
J.
Infectious Dis-
eases 171. 1152-1158.
Lagakos.
S..
Pettinelli.
C.
Stein. D.
and Volberding.
P.
A. (1993).
The Concorde
Trial.
Lancet 341. 1276.
Larder. B. A.. Kellam.
P.
and
select viable multidrug-resistant
Larder. B. A..
Kemp.
S.
antiretroviral efficacy of
Mansky.
L.
HIV-1
in vitro.
Nature 365. 151-453.
D. and Harrigan. P. R. (1995). Potential mechanism for sustained
AZT-3TC
combination therapy. Science 269. 696-699.
in vivo
than that predicted from the
1
Convergent combination therapy can
(1993).
M. and Temin, H. M. (1995). Lower
eficiency virus type
J.
Kemp.
D.
S.
mutation rate of human immunod-
fidelity of purified reverse transcriptase.
Virology 69, 5087-5094.
McLean. A. R. and Nowak. M. A.
(1992).
zidovudine resistant strains of HIV.
AIDS
McLeod. G. X. and Hammer.
S.
M.
Competition between zidovudine sensitive and
6. 71-79.
(1992).
Zidovudine: 5 years
later.
Annals of Internal
Medicine 117. 487-501.
Nabel. G.
J.
(1994).
Nowak. M. A.
Gene therapy approaches
et al.
(1991).
to
AIDS. AIDS
8.
S61-S69.
Antigenic diversity thresholds and the development of AIDS.
Science 254. 963-969.
Nowak. M. A. and May. R. M. (1993). AIDS pathogenesis: mathematical models
and SIV infections.
Ott. T.
J.
AIDS
of
HIV
7. S3-S18.
and Krishnan K. R. (19S5). State dependent routeing of telephone
use of separable routeing schemes. In Proc. 11th
27
Int.
traffic
and the
TeletrafRc Cong.. Akiyama, M.. ed..
Amsterdam.
Elsevier,
Perelson, A. S. (19S9). Modeling the interaction of the
immune system
with HIV. In Mathe-
AIDS Epidemiology, Castillo-Chavez, C,
New York, 83, 350-370.
matical and Statistical Approaches to
Notes
Biomath., Springer- Verlag,
in
The dynamics
Perelson, A. S., Kirschner, D. and DeBoer, R. (1993).
CD4+
Lecture
infection of
Math. Biosciences 114, 81-125.
cells.
Perelson, A. S. ef
and
lifespan,
HIV
of
ed.,
HIV-1 dynamics
(1995).
al.
viral generation time.
Pontryagin, L.
virion clearance rate, infected cell
Submitted to Science.
Boltyanskii, V. G., Gamkrelidze, R. V.,
S.,
The Mathematical Theory of Optimal
Richman, D. D.
in vivo:
et al.
(1994).
and Mishchenko,
Processes. Interscience Publishers,
Resistance to
AZT
therapy in patients with advanced infection with
E. F. (1962).
New
York.
and ddC during long-term combination
human immunodeficiency
virus.
J AIDS
7,
135-138.
St.
Clair.
mutation
M.
in
ef
II.
a/.
Resistance to ddl and sensitivity to
(1991).
AZT
induced by a
HIV-1 reverse transcriptase. Science 253, 1557-1559.
Schuurman, R.
et al. (1995).
Rapid changes
human immunodeficiency
in
virus type
1
RNA
load and appearance of drug-resistant virus populations in persons treated with lamivudine
(3TC).
J.
Infectious Diseases 171. 1411-1419.
Schwartz, D. H., Skowron, G. and Merigan, T. C. (1991). Safety and effects of interleukin-2
plus zidovudine in asymptomatic individuals infected with
J AIDS
virus.
4. 11-23.
Shafer. R.
W.
gene mutations.
Shafer, R.
W.
(1991).
ef al.
for drug-resistant
of
human immunodeficiency
Combination therapy with zidovudine and didanosine
human immunodeficiency
J.
et al.
virus type
1
selects
strains with unique patterns of pol
Infectious Diseases 169. 722-729.
(1995).
Drug
human immunodeficiency
combination therapy.
J.
resistance
and heterogeneous long-term
virologic responses
virus type Tinfected subjects to zidovudine
and didanosine
Infectious Diseases 172. 70-78.
Shaw, G. M. (1995). Personal communication.
Volberding, P. A.
tomatic
HIV
ef al.
infection.
(1994).
JAMA
The duration
of zidovudine benefit in persons with
272, 437-442.
28
asymp-
Wei, X.
et al.
(1995).
Viral dynamics in
human immunodeficiency
virus type
1
infection.
for the
treatment
Nature 373, 117-123.
Wilson, C. C. and Hirsch. M.
of
human immunodeficiency
S. (1995).
Combination antiretroviral therapy
virus type-1 infection.
Proc.
Ass.
American Physicians 107.
19-27.
Wilson. C. C. et
al.
(1995).
Ex
vivo expansion of CD-I lymphocytes from
human immunod-
eficiency virus type 1-infected persons in the presence of combination antiretroviral therapy.
J.
Infectious Diseases 172. 88-96.
29
/
)
APPENDIX A
The
solution to (24)- (27)
is
+ ft*(* - -)
\
/'
—
fc^-d, *
A
/
- -)
fi
'
V
-rr,
\f'{k,
Uibj
-
+
cti
kj
r
-
.
j
j
ki
n)
-
*,-)(<*
-
ki-ai
rr;
a,){k,
-
a,•-
- a j)( k t
r
+
r
(
1
fc;
//)
+
(r
a,-)
'
+
"
*,•
(v3
-
-
//
A'
/
(41
.
t
c -(*+rt(-t)\
t
)
a,
it
_
<
A-,
—
a,
;
o -kj.-fiJJ
aii-ki J
a
-
/
//
ki-cti
—^
Xiqjiftdjix—)
7r lt
-
(»<
-
a,
c\j
t)
-
a,
—-1±-)
-
Vj
{
ir-?/f-( ai+ ")( s -')
-77
/'
Ji
M-
- ai){ki -
(
\
-maPidiix ~ -)
^r'"
yi e-l°i-+
-
J J
—Q
fcj
A-,
(40)
.
A-,
t
fi
n-ki
ki-oti
cti)
(i
{ki-ctiy
\
-
a,)
- aj -
ocj){Cti
iri
ji
\{ki
/'
+
-
^(fcj
\
\{kj-
//
..
—Q
A',
j7j
- -)
-Pi(x
\
)
^/
+
oti)([i
^77
r- + & - -^-)
cti(ki-ai)
A'i-a,
//
qti&id t (x
-
H \(ki
i=i
P
-(fc.+/x)(s-t)
)'
a;
//(a,
-Vte TjMl-h
-
-
A- (
*,-)(**
:
\
//)
" ^)J
m
+
7
(42)
where the constants appearing
in these equations are
c,=i(-T^-.L --**-)-%* --i(^ + .-.))
^y,
=
-QiiPidi[t
(
7
VA'j
—
— + {ViQ,
30
A,
—
Q;
q,
—
Av
(«)
+ 9ii ftd
j--
-
--('-,-
-)(-7]
I
)
i
-)
;
*iVi
-
(aj
A
+
-a
\{kj
fi
){Qj
}
Vl
_
Ti l
-TTiqufiidi-
/
ft
\(ki
'
\(ki
t
)
l
H
V'j
("-'/,..
;Aj
j/<
-
\//(A*,
//
+
-
\(&j
-
KiVi
k
(Vi
-
Q,
-
-) +
(vi
—
-
a,
A
,
—
Q,
Q,
-
fa
_ Q j)
a,-)(fci
Qj)(Qi;-Qj
-
- Q
fcj
//)
j
7T,
-
/<)(*";
-
«j
+ (»i-
/((a,
(
_ aj
fc
77,11,
)
//
-
Cti)(ki
a, )(o,
A
Xiqjifydjix
ki
(44)
fi]
A' ly
n-«y,
)
t
-,
-
kj
^-)<
- an
-
(«i
<)
— ati)(ki — cti — p)
A
3 d {x
2
V(^«
- a[ „2 (*
,,
(
ft
I
^
A
+ft(x-
q it
- to - T 2 *-)"
kj - a } q, -
t
7T;t/j
/
"'//
a,
fcj
7T t
-a
+fi
A
C
~^±+ ft- T^^TT
_Q +
-
a, =
+
kj-aj (ai-kj
a,)
*iVj
3J dJ {x
qJl
-
%)(«<
(
-
A,
- fi)
a ~ j)(^ ~
«
fc
fc
i;
l
2/j
):
^i-«j (Ot-^i
/0
^-
-/*)(*
(45)
APPENDIX B
V
The approximate value function
L
+
—
0,(^
//
a
v
(
A
+Pi{x- -)
//'
t
(&i
-
a
2
t
+
-
Qj
«
"
_
)
7
fc
+
C„(i-
e -*iCr-t))
«iVi
>,+u)(T-t)
-
u
"t;
(Vi
(
MA', -Q,)(I',
(
e-'tr-*>)
)
-i
TTiJ/i
+
;
Cw *«(l -
ftA/^^e-^1 "-*)-!:
given by
ECt^OO + ^OO)*
77
e
is
I
rT
f
e
-
h_ y
fi){a
l;
-
+
31
)
1,2
a,-
+
fi)
(»,
//,
ki-Oi
1
- c -(^+"Hr-n
Vih + V
)
a'
:
,(o
KiVi
-Ki<4u
k;
\^ —
r| y
5|V iftift
"
l)c-
a {T - ,]
'
-{a
t
l
+
1)
-)-
+
^ W*i - aj)( ai -
—
/'
(»i
3570
kj
—r\
)(M*j - Qj)(ai
- a3
-
128
-
«,-)(<*
e
{a
t
-
kj
wy
.
[Vi
-
>
t
)
-{kj+n)(T-t)
32
-
a,
k3
-
Qj
-
kj
_
-
e
T - f)
-Qi)
-(^)(T-t) _
//(q,-
-
>
*,-(**
-otj-
!
1
k
-
t
-
/.i)(k t
*,-)(*
-
+
fi)
/
k^
——+
—
-Qj- fi){ki
fi)(ki
—
.
k\
[V
k
t
'<
J
+ fi)
fi){ai
yj
7T
+
Q,(k
m<*i-h)
^n(ki-ai){ki-ai-
-mjiPjdj{x
-Tjj-
q.
e
.(
l-e- a
of
—-(^)(r-0_i) —— +
.
)l
//
T+
Jidi-\
(j,\(ki-ai) 2
+(vi-——
+7Tigt i^di(x
t
:
-r
fi){Qj
/')
y
fi)(k3
+
fi]
))])
(46)
Date Due
my o
.-,
w|<?ff
m is*
Lib-26-67
MIT LIBRARIES
111111111!
Mlllll
llll
lllllllllllll
II III
3 9080 00939 8865