Medicaid Billing Module Personal Care Services Billing Form

Medicaid Billing Module
Personal Care Services
Billing Form
Changes to Personal Care Billing
• Personal Care will now be billed in
15-minute units.
• Maximum of 28 units per instructional day.
• Units must be documented with start and stop times.
• Extra minutes can be carried over to the next instructional day.
Personal Care Changes
• Billing form is a daily form per student.
• Form is two pages long.
• Personal Care Provider will be required to document start and stop times for each billable service throughout the school day.
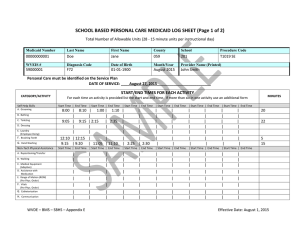
Personal Care must be identified on the Service Plan
DATE OF SERVICE: ______________________________
Student Demographics Section
Medicaid
Number
WVEIS #
Last Name First Name
Diagnosis Code Date of Birth
County School Procedure Code
T1019 SE
Month/Year Provider Name (Printed)
Student Demographics Section
• On the top row enter the information as requested.
County and school as the code numbers
• On the second row enter data as requested.
• Suggest printing a copy with all demographics completed except month/year. This will serve as a template for the school year.
• Print the name of the employee providing the personal care services.
• If two employees split the tasks with one student, each employee would complete a separate form for the services they provided.
Personal Care must be identified on the Service Plan
DATE OF SERVICE: ______________________________
Student Demographics Section
Example
Medicaid
Number
0000000001
WVEIS #
999999999
Last Name First Name
Doe Jane
Diagnosis Code Date of Birth
01-01-1900
County School Procedure Code
058 303 T1019 SE
Month/Year Provider Name (Printed)
August, 2015 John Smith
Date of Service
• List the date the services were performed.
• List the same date on the second page.
• List the student’s name on the second page.
Data Entry Section
• This is divided into 5 categories of personal care activities.
• Total of 25 billable activities
• Minutes from all of the activities are combined to determine the number of units for the day.
Data Entry Section
• There is space for six start and stop times for each activity.
• If an activity occurs more than six times a day, add additional pages as needed.
• Document the start and stop times as soon as possible when the activities occur.
• Documenting quickly will ensure more accurate data.
• If a specific activity does not occur, leave those spaces blank.
Data Entry Self Help Skills
CATEGORY/ACTIVITY
START/END TIMES FOR EACH ACTIVITY
For each time an activity is provided list the start and end time. If more than six in one activity use an additional form
MINUTES
Self Help Skills
A. Grooming
B. Bathing
C. Toileting
D. Dressing
E. Laundry
(Employee Doing)
F. Brushing Teeth
G . Hand Washing
Start Time | End Time | Start Time | End Time | Start Time | End Time | Start Time | End Time | Start Time | End Time | Start Time | End Time
8:00 | 8:10 | 1:00 | 1:10 | | | | | | | | 20
| | | | | | | | | | |
9:05 | 9:15 | 2:13 | 2:25 | | | | | | | | 22
| | | | | | | | | | |
| | | | | | | | | | |
12:10 | 12:15 | | | | | | | | | | 5
9:15 | 9:20 | 11:05 | 11:10 | 2:25 | 2:30 | | | | | | 15
Data Entry
Non-Tech Physical Assistance
Non-Tech Physical Assistance
A.
Repositioning/Transfer
B. Walking
C. Medical Equipment
(Adaptive)
D. Assistance with
Medication
E. Range of Motion
(ROM)
(Per Phys. Order)
F. Vitals
(Per Phys. Order)
G. Catheterization
H. Communication
Start Time | End Time | Start Time | End Time | Start Time | End Time | Start Time | End Time | Start Time | End Time | Start Time | End Time MINUTES
| | | | | | | | | | |
| | | | | | | | | | |
| | | | | | | | | | |
| | | | | | | | | | |
| | | | | | | | | | |
| | | | | | | | | | |
| | | | | | | | | | |
| | | | | | | | | | |
Data Entry Nutritional Support
CATEGORY/ACTIVITY
START/END TIMES FOR EACH ACTIVITY
For each time an activity is provided list the start and end time. If more than six in one activity use an additional form
MINUTES
Nutritional Support
A. Meal Preparation
Start Time | End Time | Start Time | End Time | Start Time | End Time | Start Time | End Time | Start Time | End Time | Start Time | End Time
| | | | | | | | | | |
B. Feeding | | | | | | | | | | |
C. Special Dietary
Needs
| | | | | | | | | | |
Data Entry Environmental
Environmental
A. Housecleaning
B. Laundry/Ironing
(Supervision)
C. Making/Changing
Bed
D. Dishwashing
Start Time | End Time | Start Time | End Time | Start Time | End Time | Start Time | End Time | Start Time | End Time | Start Time | End Time
| | | | | | | | | | |
| | | | | | | | | | |
| | | | | | | | | | |
| | | | | | | | | | |
MINUTES
Data Entry Behavior Modifications
Behavior
Modifications
Start Time | End Time | Start Time | End Time | Start Time | End Time | Start Time | End Time | Start Time | End Time | Start Time | End Time
A. Supervision of
Non-Educational
Time
B. Redirection
7:45 | 8:00 | 11:10 | 12:10 | | | | | | | |
C. Positive Behavior
Supports
9:30 | 9:40 | 9:55 | 10:00 | 1:15 | 1:20 | 1:30 | 1:39 | 1:50 | 1:55 | |
1:55 | 2:15 | | | | | | | | | |
MINUTES
90
34
20
Data Entry Minutes
• Add up the total minutes per row and list in the
Minutes column at the far right of the pages.
• If an activity does not have any start and stop times listed, place NA in the minute column for that row.
• In the carryover box enter any extra minutes from the previous day. The first day would be zero minutes. This carryover would be added to the minutes for the total minutes for the day.
• Add up the minutes from both pages and the carryover minutes. List under total minutes.
Unit Calculations
CARRYOVER MINUTES FROM PREVIOUS INSTRUCTIONAL DAY 0
Unit Calculations
TOTAL DAILY MINUTES 206 DIVIDE BY 15 = TOTAL DAILY UNITS 13 Carryover minutes for next instructional day 11
Calculations
• There were not any carryover minutes in our example.
• Total 206 minutes
• Divided by 15 minutes
• Equals 13 units
• Remainder of 11 minutes that will be entered into the carryover box on the next day’s data entry form.
Signature and Credential
• The provider signs the form
• The provider lists credential
• Credential is the employee designation such as Aide (I, II, III, IV), Autism Mentor,
Paraprofessional, ECCAT(I,II,III), Braille
Specialist, Sign Language Interpreter(I, II),
Sign Support Specialist, or LPN.
Terry Riley – Coordinator
Office of Special Education tjriley@k12.wv.us
304-957-9833 ext 53223
WVDE Medicaid Website:
http://wvde.state.wv.us/osp/medicaid.html