Ins and outs of cost-effectiveness analysis for treatments of rare diseases:
advertisement

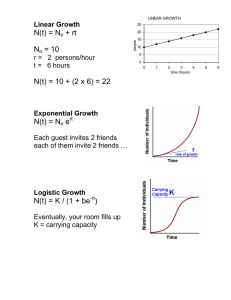
Ins and outs of cost-effectiveness analysis for treatments of rare diseases: Fabry and Gaucher disease Marcel G.W. Dijkgraaf, PhD Clinical Research Unit m.g.dijkgraaf@amc.nl 6th Health Policy Workshop 26 November 2014 My dear colleagues Carla Hollak Saskia Rombach Laura van Dussen Marieke Biegstraaten Gabor Linthorst 2 …. between 14.30 and 15.30 hrs …. TIPharma 3 4 Presentation lay-out • Regulatory context of cost-effectiveness analyses • Enzyme replacement therapies for Fabry & Gaucher • Common grounds in analytic approach • Distinct results • Discussive remarks on CEAs of rare diseases 5 Why cost-effectiveness analyses of rare diseases? Increasing numbers of orphan product designations 1983-2011 (FDA) 350 Number of Orphan Designations 300 250 200 150 100 50 0 83 84 85 86 87 88 89 90 91 92 93 94 95 96 97 98 99 00 01 02 03 04 05 06 07 08 09 10 11 6 Orphan drug designation • Incentives: – 10 year exclusivity after granting of a marketing authorisation – help with preparing the dossier to meet regulatory requirements – fee reductions, depending on size of enterprise – eligibility for EU-funded research 7 Orphan designation criteria REGULATION (EC) No 141/2000 OF THE EUROPEAN PARLIAMENT AND OF THE COUNCIL of 16 December 1999 Less than 5 in 10,000 in the EU (around 250,000 people) Life-threatening or chronically debilitating Expected sales don’t cover the developmental costs: incentives needed Likelihood of significant benefit over existing medicinal products or methods EMA/Committee on Orphan Medicinal Products assesses the available evidence supporting that likelihood 8 Market authorisation • significant benefit to be confirmed with data by applicants at the time of market authorisation to maintain orphan status • significant benefit defined as ‘a clinically relevant advantage or a major contribution to patient care’ • authorisation “under exceptional circumstances”, following limited available evidence justified by – Lack of trial data given rarity of the disease – Lack of trial data given ethical issues 9 Why cost-effectiveness analyses of rare diseases? If authorisation ‘under exceptional circumstances’, then there will be a continuing need to assess the long term effectiveness and cost-effectiveness of the orphan drug under usual circumstances 10 Why cost-effectiveness analyses of rare diseases? Increasing global orphan drugs demand by value in US$ million 2005 2006 2011 CAGR (%) 2006–2011 Biologics 30,200 35,300 53,400 9 Nonbiologics 24,300 23,400 28,400 4 Total 54,500 58,700 81,800 7 Sharma A, Jacob A, Tandon M, Kumar D. Orphan drug: Development trends and strategies. Journal of Pharmacy and Bioallied Sciences 2010;2(4):290-299. 11 Presentation lay-out • Regulatory context of cost-effectiveness analyses • Enzyme replacement therapies for Fabry & Gaucher • Common grounds in analytic approach • Distinct results • Discussive remarks on CEAs of rare diseases 12 Enzyme replacement therapies under evaluation FABRY* General name GAUCHER agalsidase alpha agalsidase beta Replagal Fabrazyme Cerezyme VPRIV Company Shire Genzyme Genzyme Shire Authorisation 2001 2001 1991** 2010 Brand name imiglucerase velaglucerase *Specific requirement: outcomes research + pharmaco-economic evaluation **Orphan Drug Legislation approved by European Parliament in 1999 Fabry disease • X-linked inherited deficiency of -Galactosidase A, an enzyme for the breakdown of glycolipids (globotriasylceramide or GL-3) in lysosomes • storage of glycolipids in vascular endothelial cells, smooth muscle cells or other cell types normal deficiency storage increased volume Fabry disease symptoms & organ damage • • • • • • • • • Acroparesthesia / neuropathic pain in extremities, Fabry-crises (periodic intense pain attacks) fatigue red-purple spots in the skin (angiokeratomas) proteinuria affected vision or hearing gastrointestinal complaints heart complaints & failure renal complaints & failure stroke / dementia • 1 / 40,000 Clinical trials agalsidase beta agalsidase alfa Eng et al NEJM 2001; 345: 9-16 Clearance of storage in renal capillaries Baseline: Score = 3 Schiffmann et al JAMA. 2001;285:2743-2749 Decrease in painscore Week 20: Score = 0 p = 0.021 7 6 5 4 3 2 1 0 0 m. 6 m. Placebo Agalsidase alfa Type 1 Gaucher disease • deficiency of Glucocerebrosidase preventing the breakdown of glucocerebrosides in lysosomes • storage primarily in spleen, liver & bone marrow cells • no involvement of central nervous system Symptoms & organ failure: • easy bleedings & bruises • extreme fatigue • anemia • bone & joint crises (pain attacks) • bone fracture • large spleen and liver • 1 / 70,000 Disease courses Death Severity --------------------- Organ failure Advanced disease Early signs or symptoms No symptoms Age --------------------- Presentation lay-out • Regulatory context of cost-effectiveness analyses • Enzyme replacement therapies for Fabry & Gaucher • Common grounds in analytical appproach • Distinct results • Discussive remarks on CEAs of rare diseases 19 Analytic approach to appraisal of ERTs • Life-time Markov state-transition models – Events occur repeatingly over time – Longer term, lifetime consequences • “Significant benefit”: – Postponement of end-organ damage in years – Quality adjusted life years • Costs from a societal perspective – Medical costs – Costs of production loss 20 Simple Markov Model Time t Well Sick Dead t+1 Well Sick Dead Fabry disease 22 Gaucher disease 23 untreated prior to ERT introduction INTRO ERT In absence of RCTs of sufficiently long duration... treated after ERT introduction Selection bias untreated after ERT introduction 24 Assumptions FABRY: • • ERT only decreases the probability of progression to next state no distinction between agalsidase alpha and aglasidase beta because – lack of evidence for superiority of either one – comparable costs at the registered dose GAUCHER: • ERT allows for recovery from signs/symptoms: otherwise, it only decreases the probability of progression to next state Both: • Health utilities, health care volumes and related costs (other than ERT itself) for treated as well as untreated males and females are similar for patients in the same disease state 25 Number of Fabry patients for data gathering 26 Data & estimates transition probabilities (TP) • Medical chart reviews prior to & after intro of ERT • Natural course: – Kaplan-Meier survival curve analysis, with median (or less) durations in years recalculated into TPs accounting for model cycle length; in case of Gaucher accounting for competing risks • ERT: – Multiple logistic regression on progression to next state for ERT duration in years; odds ratio for treatment duration used together with median treatment duration and model cycle length to calculate ‘1 minus relative risk reduction’ as multiplicator of TPs natural course • Lower limit for probability of dying: general population CBS statistics 27 Fabry yearly transition probabilities 28 Data & estimates of health utilities • 3-monthly EQ-5D questionnaires, after introduction of ERT • Five dimensions: mobility, self-care, daily activities, pain/complaints, mood • Each dimension: no (1), some (2), severe problems (3) • Response patterns (e.g. 11231, or 21211) weighted with maximum health utility of 1 in absence of any problems and with death taking the value of 0. Weighting based on time trade-off based elicitation techniques of preferences in general population • First averaging all measurements per patient per disease state, then taking the average per disease state 29 Health utilities for Fabry disease states 30 Health utilities Fabry & Gaucher Disease state Fabry Gaucher Asymptomatic 0.87 0.93 Symptoms / 0.76 0.87 Recovery Single complication 0.74 Splenectomy 0.75 Bone complication 0.86 Multiple complications Malignancy 0.58 0.73 0.15 31 Data & estimates of costs • 2004-2010 production data from national reference center; local unit costing • 3-monthly patient questionnaires for hospital care elsewhere, out-ofhospital care, and production loss • Unit costing compliant with national health care costing guideline • First averaging all measurements per patient per disease state per year, then taking the average per disease state • Yearly drug costs: – FABRY: prototypical yearly costs for a patient of 70kg – GAUCHER: mean yearly costs per patient per disease state based on used vials of 400 IU per 32 Yearly costs of Gaucher disease 33 Presentation lay-out • Regulatory context of cost-effectiveness analyses • Enzyme replacement therapies for Fabry & Gaucher • Common grounds in analytic approach • Distinct results: the Fabry case • Discussive remarks on CEAs of rare diseases 34 Cost-effectiveness analysis of ERT for Fabry • Lifetime perspective with a 70-year time horizon • Base case scenario: – Males : females = 1 : 1; enter the model at birth; ERT prescribed when symptoms developed; only medical costs included • Six alternative scenarios: – Delayed start with ERT: symptoms AND age>=40 – Lower health utility for untreated when in same state as treated – For classical phenotypes only (no R112H or P60L substitutions or intermediate level of lysoGb3) – Natural course of disease adjusted for the use of ACE-inhibitors or angiotensin blockers to prevent cardiovascular events – No ERT in groups with multiple complications – Including costs of production loss 35 CEA of ERT for Fabry: costs 36 CEA of ERT for Fabry: effects 37 CEA of ERT for Fabry: ICERs 38 Cost-effectiveness acceptability curve Fabry 39 CEA of ERT for Fabry: scenarios 40 CEA conclusions Fabry • Small gains in effectiveness over a lifetime • ERT has a low probability of being cost-effective according to conventional standards • High ICERs, hardly dependent on subgroup selection, including production losses or early stopping if progress • High ICERs, highly dependent on health utility contrast, costs of ERT (sensitivity analysis), or comedication 41 Presentation lay-out • Regulatory context of cost-effectiveness analyses • Enzyme replacement therapies for Fabry & Gaucher • Common grounds in analytic approach • Distinct results: the Gaucher case • Discussive remarks on CEAs of rare diseases 42 CEA of ERT for Gaucher • Lifetime perspective with a 85-year time horizon • Base case scenario: – Enter the model at birth; ERT prescribed when symptoms developed; only medical costs included • Three alternative scenarios: – Including costs of production loss (max 40 years) – drop in ERT costs per vial (up to 25%) – historical Dutch situation: distribution of patients across disease states a time of market introduction (with or without asymtomatic patients 43 The historical scenarios 44 CEA of ERT for Gaucher: ICERs (YFEOD) 45 CEA of ERT for Gaucher: ICERs (QALY) 46 Cost-effectiveness acceptability curve Gaucher 47 CEA conclusions Gaucher • Substantial gains in effectiveness over a lifetime • ERT has a low probability of being cost-effective according to conventional standards • ICERs hardly depend on including production losses and highly depend on ERT costs • Historical scenarios shows significance of early treatment start 48 Presentation lay-out • Regulatory context of cost-effectiveness analyses • Enzyme replacement therapies for Fabry & Gaucher • Common grounds in analytic approach • Distinct results • Discussive remarks on CEAs of rare diseases 49 Pro’s and con’s of CEAs Why? Why not? • Money matters • Rationing decision making • Reference case for further optimizations • Communicative vehicle • Expensive D, cheap R • Heavy assumptions & high uncertainty level • Lack of support • Risk of anticipative behavior • Imbalanced focus across settings within and beyond health care 50 Thank you !