Lean Implementation at Jefferson Healthcare Earll Murman LAI Annual Conference
advertisement

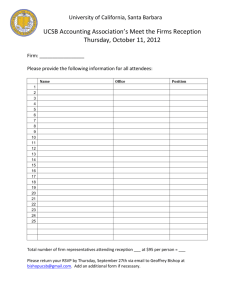
Lean Implementation at Jefferson Healthcare Earll Murman LAI Annual Conference March 25, 2010 Rural Healthcare Case Study Jefferson County, WA – Population 29,542 (2008 est.) Photo by Earll Murman Source: Google © 2010 MIT Murman LAI Annual Meeting 2 Jefferson Healthcare Overview • History 1890 Sisters of Providence founded St John’s Hospital 1975 Jefferson County Public Health District takes ownership and establishes Jefferson General Hospital 2002-2007 Acquired 5 primary care clinics 2003 Designated Critical Access Hospital 2004 Renamed Jefferson Healthcare • • • • Governed by 5 elected Commissioners Largest employer in Jefferson County, 489 employees Annual budget approximately $45 million Over three quarters of business is outpatient © 2010 MIT Murman LAI Annual Meeting 3 Seattle Hospitals Medivac Jefferson Healthcare Enterprise Harrison Hos. Bremerton Acute Cardiac Swedish MC Seattle Stroke Telemedicine Drive to Family Birth Center In Patient East Jefferson Fire & Rescue 25 Bed s ED and Express Care Surgery Five Primary Care Clinics PT and Rehab Home Health & Hospice Port Ludlow Fire & Rescue Medical Short Stay Diagnostics © 2010 MIT Murman LAI Annual Meeting 4 JHC Drivers for Lean Grow activity and contain costs while achieving: Purpose – To assure appropriate healthcare services are available to support the health of all people of Eastern Jefferson County Values – Jefferson Healthcare is: • Intentionally Patient Centered • Committed to the highest possible quality healthcare for all • An employer that recognizes the quality of its employees and helps them to reach their potential • Committed to a health community that encourages individual responsibility • A prudent steward of healthcare resources Mission – Jefferson Healthcare ... excellence with compassion and innovation Source: http://207.56.191.254/web/AboutJeffersonHealthcare/PurposeValuesMission/tabid/89/Default.aspx © 2010 MIT Murman LAI Annual Meeting 5 JHC Lean History • • Early 2000 – As one of 20 rural hospitals affiliated with Virginia Mason in Seattle, JHC CEO was aware of lean Exploratory: 2003 – 2006 • • • • • Four staff attended Lean training – brought tools home Conducted RPIW for patient registration Difficult implementation but good results (45 5 min) Island of success – no traction across JHC Enterprise commitment: 2006 – present • CEO and other directors received 1 week training • Strategic decision to make Lean the JHC Performance • • • • Improvement system Contracted with Joan Wellman & Associates Formed Lean Resource office Budgeted $1M annually for lean implementation ~ 200 improvement opportunities identified © 2010 MIT Murman LAI Annual Meeting 6 Lean Organization • Lean Resource Office reports to CEO • • • Lead is member of JHC Strategic Leadership Group Three Lean Fellows and one admin support Lead is RN with experience in ED, OB, IT • Joan Wellman Associates under contract to • provide lean expertise - the JHC Sensei • Associate spends 1 week/month on site The 5 lean team members support 30 events/year as coaches, experts, facilitators © 2010 MIT Murman LAI Annual Meeting 7 JHC Lean Events Primary tools employed are 5S, RPIW, VSMA 2007 7 events 2008 30 events 2009 30 events Photo by Earll Murman Examples: OP Clinic VS, ED VS, AMI RPIW, Stroke RPIW, Laundry RPIW, Safety Office 5S, Pt discharge © 2010 MIT Murman LAI Annual Meeting 8 Acute Myocardial Infarction RPIW • Time is critical for treating major • • • • • heart attacks. • Greatest loss of heart muscle is in first 2 hours Recommended treatment is catheter insertion of balloon within 90 min of “presentation” Alternate treatment “clot busting” thrombolytic drug Situation Closest Cat Lab is in Bremerton – minimum 55 min drive time No clear boundary for when patients go to Bremerton or when they require thrombolytics at JHC Average “as is” treatment or process time at JHC is 165 min RPIW Targets – Reduce Lead Times for AMI response © 2010 MIT Murman LAI Annual Meeting 9 Pt Value Stream Intersects Multiple Organizations Common process required for 6 different organizations © 2010 MIT Murman LAI Annual Meeting 10 Images from AMI RPIW Planning training ED RN Lean Fellow BEFORE 165 min AFTER 20 or 60 min Cardiologist CNO ED MD Writing new protocols Lean Fellow Photos by Earll Murman House Coordinator Jefferson Healthcare Acute Myocardial Infarction RPIW – April 20-24, 2009 Process Owner © 2010 MIT Murman LAI Annual Meeting 11 Future State AMI Algorithm • • • • • Key to RPIW was the focus on Pt and Pt value stream Six different organizations working collaboratively to provide the best care possible given constraints Clear geographic boundaries delineate treatment pathway based on time-to-treatment constraints Process time measured by stopwatch strapped to Pt Medics certified to administer thrombolytic drugs in EMS van The “hospital” is where the patient is. © 2010 MIT Murman LAI Annual Meeting 12 Value Stream Event for JHC Outpatient Clinics • Situation • Five legacy outpatient clinics • Few standard processes • Little coordination between clinics and • • • with other parts of JHC Patients per day per doctor under national norms Poor flow and facility layout Primary Event Focus: • Identify standard patient flow for clinic encounters; improve patient access and provider productivity Photos by Earll Murman © 2010 MIT Murman LAI Annual Meeting 13 Jefferson Healthcare Clinic - Current State Map OVERALL CLINIC DATA EXTERNAL PROVIDERS - Blocked Hours – 67/day - Cost per visit - $125.39 - Contact Hours 59/day - Avg. Pts per hour - 1.83 - Utilization 88% - Available hours per day – 67 PATIENT DATA Enterprise Receive Med History & Call to Schedule - Cancel by reason - see chart A Reception - Payor mix – commercial 38% ROS V1 - Satisfaction – overall 74.4 Visit Clinic Reception - Volume by Diagnosis – See chart B Phone call Reg Pkt V2 Enterprise EMR Enterprise Call patient to schedule Hot Reception Input Med History Reception ROS V1 Reception Interface EMR Room & perform vitals, etc. Reception RN 19.1 1.6 Enterprise Pre-reg, Schedule, & Send packet Med list Check-in patient for visit 2.2 - Schedule on 1st call – 0% Rad film rg Routing Slips - Days out by provider - See C Obtain Demographics “mini-reg” & Send packet Scripts Di sc Scripts - Days out for first 3rd visit – 3.75 Enterprise ha Salmon reminder (PTFP) Document delays – 2% - # of Pts on panel – 5997 e EXTERNAL PHARMACIES Phone call - Schedule on 1st call – 0% - Market share - Hospital 46.7% Input Med History e Wait for ex prov to return info PATIENT Phone call EMR rg Request Med History records Reception Wait for pt to return packet - Volumes - 131 visit/day ha Reception Med History sc Di Receive call & Send registration packet Reg Pkt V1 Discharge Enterprise Interface Educ. EMR EMR See patient Check-out patient MD, PA Referral Coordinator 20.7 - # of Pts on panel - 5998 - No shows – 2% - On-time starts – 37% - Days out for first 3rd visit 2.00 - On-time starts – 37% - Time by diagnosis – Chart D - Days out by provider- see chart C - Document delays – 12% - Volume by hour – Chart E Reg Pkt V2 Reception - Schedule on 1st call – 100% - # of Pts on panel 5886 - Days out for new visit - 15.01 EMR Walk to hospital MediTech MediTech Register for Ancillary Services HOSPTIAL Ancillary Services Hospital Registration 4.8 walk or return 4.4 31.2 9.7 Referrals Orders 14.0 L/T 2.3 2.1 - Referral volume – 14.5 % 3.1 - Volumes by service – 13.0% - Lead-time by service - varies ROS V2 Input Med History following Check-in Reception - Document delays – 30% LEGEND = PTFP Scheduling = Hospital Services = OPC Scheduling = Patient = JMPG Scheduling = Patient on schedule = Clinic flow (all sites) - Days out by provider – See Chart C Days out for first 3rd visit – 1.16 Source: Jefferson Healthcare, Port Townsend, WA © 2010 MIT Murman LAI Annual Meeting 14 C/T Jefferson Healthcare Clinic - Ideal State Map OVERALL CLINIC DATA Jefferson Website History Request Appt Request - Research Providers - Input Medical History - Input Registration Data - Initiate requests for Med Hx from external providers Appt History Request EXTERNAL PROVIDERS Request Reg Pkt Reg Pkt Pt Info - Contact Hours 59/day - Avg. Pts per hour - 1.83 - Utilization 88% PATIENT DATA - Available hours per day – 67 - Volumes - 131 visit/day PATIENT Patient Info Reg Pkt - Blocked Hours – 67/day - Cost per visit - $125.39 - Cancel by reason - see chart A Reminder - Payor mix – commercial 38% Pre Visit Check-in - Satisfaction – overall 74.4 Reg Pkt - Volume by Diagnosis – See chart B EXTERNAL PHARMACIES Reminder Reminder Visit Clinic Phone call Reschedule Mail or Walk-in EMR n Same Day (urgent) 2-Wks (non-urgent, no preference) Schedule Pt Schedule & Initiate Pt & Initiate Registration Registration Reception Reception Reschedule Reg Pkt n Call Pt to Reschedule due to incomplete records Scripts Phone call reminder Pt Info Enterprise Complete Pre-Reg & Demographic Documentation n Reception Call Pt for Visit Reminder Reception Reception 1 Wk prior E-mail reminders EMR - Check-In Enterprise Hold daily Check-in Check-in huddle Check-in Patient Check-in Patient Patient Clinic Patient Reception Team Reception Reception Reception Pod n Scripts Routing Slips Interface EMR Check-in Patient Interface Rad film Clinic Kiosk Pre Visit Check-in Enterprise Enterprise n Enterprise Phone call MediTech Enterprise E-mail reminders Discharge Med History Appt Request - Market share - Hospital 46.7% Internet EMR Room & perform vitals, etc. ROS Reception Med list MA n n Educ. See See Orders patient See patient patient Care Providers, Team Providers, RN, MA RN, MA MediTech HOSPTIAL Ancillary Services Referrals Enterprise E-orders Check-out patient Recall Patient Follow-up care Referral Coordinator Reception n n 2 days prior for limited patients 10-15 min - Schedule on 1st call - No shows - On-time starts - # of Pts on panel - On-time starts - Time by diagnosis - Days out for first 3rd visit - Document delays - Volume by hour - Referral volume - Volumes by service – 13.0% - Days out by provider - Lead-time by service - varies LEGEND = Hospital Services = Scheduling Receptionist = MA = Clinic Receptionist = MD/PA = Referral Coordinator = RN = Patient = Patient on schedule Source: Jefferson Healthcare, Port Townsend, WA n = Queues (Inventory) © 2010 MIT Murman LAI Annual Meeting 15 Jefferson Healthcare Clinic – Future State Focus (2008) OVERALL CLINIC DATA EXTERNAL PROVIDERS - Available hours per day – 67 Enterprise Receive Med History & Call to Schedule PATIENT Phone call EMR Reception by –(TBD) - Payor mix commercial 38% ROS V1 - Satisfaction – overall 74.4 Reception Visit Clinic Establish Pt focus group by 4-1-08 - Volume by Diagnosis – See chart B EXTERNAL PHARMACIES Obtain Demographics “mini-reg” & Send packet Enterprise Develop standard Call patient registration packet by 12-31-07 to schedule Enterprise EMR Hot Reception Develop clinic service standards by 12-31-07 Hire/train MA resources - Days out by provider - See C Input Med History Develop process ROS for capturing Hx V1 Reception pre-visit by 7-1-08 Reception Check-in patient for visit Enterprise Pre-reg, Schedule, & Send packet EMR 19.1 1.6 Align Educ. to care teams in pods EMR by Orders (TBD) See patient MD, PA 31.2 9.7 Develop pre-order 4.4 & future lab capabilities in EMR by 7-1-08 20.7 - # of Pts on panel - 5998 - No shows – 2% - On-time starts – 37% - Days out for first 3rd visit 2.00 - On-time starts – 37% - Time by diagnosis – Chart D - Days out by provider- see chart C - Document delays – 12% - Volume by hour – Chart E Reg Pkt V2 Reception - Schedule on 1st call – 100% - # of Pts on panel 5886 - Days out for new visit - 15.01 EMR Rad film Routing Slips Med list standard room by 4-1-08 RN Implement daily huddle by 11-1-08 Scripts Di sc Scripts Room & perform Develop vitals, etc. Reception 2.2 Develop standards for scheduling & reception by 4-7-08 - Schedule on 1st call – 0% Interface ha Salmon reminder (PTFP) Document delays – 2% - Days out for first 3rd visit – 3.75 rg e Phone call - # of Pts on panel – 5997 Develop standard Reg Pkt Enterprise scheduling template by 4-1-08 V2 Improve Pt satisfaction - Cancel by reason - see chart A Phone call - Schedule on 1st call – 0% - Market share - Hospital 46.7% Input Med History e Wait for ex prov to return info Wait for pt to return packet - Volumes - 131 visit/day rg Reception PATIENT DATA Address safety measures & gaps by 10-31-08 Med History Request Med History records Improve staff satisfaction by (TBD) ha Reception - Utilization 88% sc Di Receive call & Send registration packet Reg Pkt V1 - Contact Hours 59/day - Avg. Pts per hour - 1.83 Discharge Enterprise - Blocked Hours – 67/day - Cost per visit - $125.39 Interface MediTech Develop post- MediTech Referrals visit standard Register for Check-out work by (TBD) Ancillary Walk to patient hospital Services EMR Referral Coordinator HOSPTIAL Ancillary Services Hospital Eliminate need to Registration re-register in hospital Standardize 4.8visit walk documentation or return by (TBD) 14.0 L/T 2.3 2.1 - Referral volume – 14.5 % 3.1 - Volumes by service – 13.0% - Lead-time by service - varies ROS V2 Input Med History following Check-in Reception - Document delays – 30% LEGEND = PTFP Scheduling = Hospital Services = OPC Scheduling = Patient = JMPG Scheduling = Patient on schedule = Clinic flow (all sites) - Days out by provider – See Chart C Days out for first 3rd visit – 1.16 Source: Jefferson Healthcare, Port Townsend, WA © 2010 MIT Murman LAI Annual Meeting 16 C/T Standard Rooms and Central Supplies 5S Events in each Clinic © 2010 MIT Murman LAI Annual Meeting 17 Source: Jefferson Healthcare Lean Events Targeting Each Step in the Clinic Value Stream Standard Work creates a foundation to build on FIW Dec 2007 FIW Mar 2008 FIW Mar 2009 RPI Jun 2008 RPI Mar 2009 RPI Sep 2008 FIW = Focused Improvement Workshop © 2010 MIT Murman LAI Annual Meeting 18 Source: Jefferson Healthcare Daily Management System Implement daily huddle © 2010 MIT Murman LAI Annual Meeting 19 Photos by Earll Murman Results Project Access RPI Cumulative Available Clinic Hours 2007, 2008, 2009 (Feb 2009): • • Reorganized Medical Staff Structure Consolidate Provider meetings reducing meeting hours. • Revise scheduling guidelines (20 min vs. 40 min vs. 60 min) • 6000 5500 5000 4500 4000 3500 3000 2500 2000 1500 1000 Project Access RPI 2007 CML 2008 CML 2009 CML January February March April Create schedule management strategies using daily huddle © 2010 MIT Murman LAI Annual Meeting 20 Source: Jefferson Healthcare Results © 2010 MIT Murman LAI Annual Meeting 21 Source: Jefferson Healthcare JHC Accomplishments • Laundry RPIW was early success • • • • Saved laundry from being outsourced • Stabilized staff at 3 FTE from 4 FTE budgeted • Customer satisfaction went from 70% to 100% Most MDs “get it”, are on board, and are driving process improvement • Launching the Clinic VS was a tipping point • OR daily “on time start” went from 14% to 96% Culture beginning to change Community now has excellent stroke and acute cardiac care response for rural hospital 45% employee participation in at least one event Source: Jefferson Healthcare • © 2010 MIT Murman LAI Annual Meeting 22 • • • • • Success Factors CEO leadership, commitment, engagement Enterprise-wide process improvement method Commitment of resources • Engaging consultant on long-term contract • Lean Resource office • Tiger teams from IT, EVS, facilities, materials mgmt support rapid change during RPIWs Getting MDs involved and on board • Active participants in process improvement No layoffs for productivity improvements “The lesson learned by the MDs from the clinical value stream RPI was that lean focuses on what to do to make them, the patients, and the staff happy.” Vic Dirksen, CEO © 2010 MIT Murman LAI Annual Meeting 23 Challenges and Opportunities • “Lean fatigue” – 30 events per year for 489 • • employees and 4 lean resource office staff is at capacity of organizational rate of change Changing culture opens opportunities for bottom-up implementation • Transforming Care at Bedside is an example • Making everyone a problem solver all the time “Biggest gains still to come” “Lean is an effective way for me to make systemic, not charismatic, change in process improvement at Jefferson Healthcare.” Vic Dirksen, CEO © 2010 MIT Murman LAI Annual Meeting 24 Acknowledgements • • • • • • Terri Camp – Jefferson Healthcare Teresa Deason – Joan Wellman Associates Vic Dirksen – Jefferson Healthcare Paula Dowdle – Jefferson Healthcare John Nowak – Jefferson Healthcare Matt Ready – Jefferson Healthcare © 2010 MIT Murman LAI Annual Meeting 25