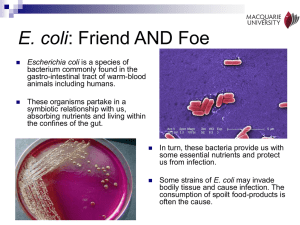
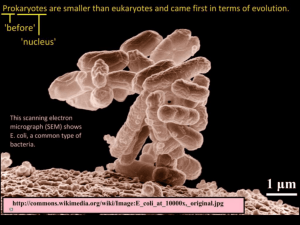
Pathogenic E. coli ---
advertisement

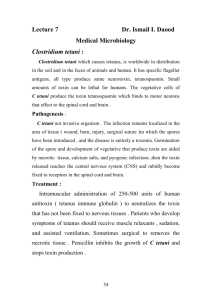
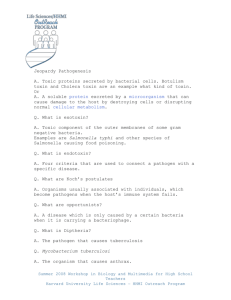
医学微生物学 Medical Microbiology 病原生物学教研室 Department of pathogenic Biology of Gannan Medical University 张文平 Chapter 11 Enteric Bacilli (Enterobacteriaceae) Classification •Enterobacteriaceae (肠杆菌科细菌) •Vibrio cholerae(霍乱弧菌) •Vibrio parahaemolyticus (副溶血性弧菌) •Helicobacter pylori (幽门螺杆菌) •Campylobacter(弯曲菌属) Characteristics large Gram- negative rods associated with intestinal infections (bacillary dysentery, typhoid, and food poisoning ) oxidase negative glucose fermenters & nitrate reducers the pathogenicity of a particular enteric bacterium can be determined by its ability to metabolize lactose Escherichia coli Coliform — enterobacteria which ferment lactose Characteristics Morphology usually motile, produce peritrichous flagella some produce polysaccharide capsules grow well on non-selective media, forming smooth, colourless colonies 2-3 mm in diameter in 18h on nutrient agar temperature (15-45℃) Characteristics Colonies on selective media blue and violet colonies on EMB agar red colonies on MacConkey agar Characteristics Biochemical reaction aerobic or anaerobic --can grow in the presence or absence of O2. typically oxidase-negative most strains ferment lactose & glucose with the production of acid and gas IMViC reaction : + + - - distinguish! Reactions on TSI agar slantsi Characteristics Antigenic structure Over 700 antigenic types (serotypes) are recognized based on O, H, and K antigens. Lipopolysaccharide LPS (heat-stable somatic antigens ) -- O antigens flagellar antigens -- H antigens "capsular" antigens -- K antigens Diseases caused by E. coli E. coli is responsible for three types of infections in humans: urinary tract infections (UTI), neonatal meningitis, intestinal diseases (gastroenteritis). Pathogenic E. coli Five classes (virotypes) of E. coli that cause diarrheal diseases are now recognized: enterotoxigenic E. coli (ETEC), enteroinvasive E. coli (EIEC), enterohemorrhagic E. coli (EHEC), enteropathogenic E. coli (EPEC), enteroaggregative E. coli (EAggEC). Pathogenic E. coli Pathogenic E. coli Enterotoxigenic E. coli (ETEC) •cause diarrhea in infants and travelers Pathogenic E. coli ---- ETEC pathogenesis of ETEC involves two steps: intestinal colonization, fimbrial adhesins e.g. CFA I, CFAII, K88. K99 non invasive diarrheagenic enterotoxin(s) -- LT and/or ST toxin both traits are plasmid-encoded Pathogenic E. coli ---- ETEC Enterotoxins LT (heatlabile) toxin ST (heatstable) toxin Pathogenic E. coli ---- ETEC heat-labile toxin(1) similar to Vibrio cholerae enterotoxin. two types of subunits. the B subunit binds the toxin to the target cells via a specific receptor that has been identified as Gm1 ganglioside. the A subunit is then activated by cleavage of a peptide bond and internalized Pathogenic E. coli ---- ETEC heat-labile toxin(2) The actived subunit A then catalyzes the ADP-ribosylation (transfer of ADP-ribose from nicotinamide adenine dinucleotide [NAD]) of a regulatory subunit of membrane-bound adenylate cyclase, the enzyme that converts ATP to cAMP. This activates the adenylate cyclase, which produces excess intracellular cAMP, which leads to hypersecretion of water and electrolytes into the bowel lumen. Pathogenic E. coli ---- ETEC heat-stable toxin ST enterotoxin causes an increase in cyclic GMP in host cell cytoplasm. Two major classes -- Sta & STb Those termed STa stimulate intestinal guanylate cyclase, the enzyme that converts guanosine 5'-triphosphate (GTP) to cyclic guanosine 5'-monophosphate (cGMP). Increased intracellular cGMP inhibits intestinal fluid uptake. Those termed STb do not seem to cause diarrhea by the same mechanism. Pathogenic E. coli ---- ETEC Laboratory methods for isolation and identification of ETEC Pathogenic E. coli ---- ETEC Control controlled by preventing transmission and by stressing the importance of breast-feeding of infants The best treatment is oral fluid and electrolyte replacement (intravenous in severe cases). Antibiotics are not recommended ----antibiotic-resistant pathogenic E coli Pathogenic E. coli Enteroinvasive E. coli (EIEC) Shigella-like E coli strains dysentery-like diarrhea (mucous, blood), severe inflammation, fever nonfimbrial adhesins, possibly outer membrane protein invasive (penetrate and multiply within epithelial cells) does not produce shiga toxin Pathogenic E. coli ---- EIEC Cellular pathogenesis of invasive E coli Pathogenic E. coli ---- EIEC Sereny test -- Invasive E coli, like Shigella, causes a rapid keratoconjunctivitis when placed on the conjunctiva of the guinea pig eye. Virulent Sereny test-positive isolates carry a large (usually 140-megadalton) plasmid responsible for this property. Pathogenic E. coli Enteropathogenic E. coli (EPEC) non fimbrial adhesin (intimin) moderately invasive (not as invasive as Shigella or EIEC) "attaching and effacing" does not produce LT or ST; some reports of shiga-like toxin usually infantile diarrhea; watery diarrhea similar to ETEC, some inflammation, no fever; symptoms probably result mainly from invasion rather than toxigenesis Pathogenic E. coli Enterohemorrhagic E. coli (EHEC) represented by a single strain (serotype O157:H7) adhesins not characterized, probably fimbriae moderately invasive produces shiga toxin but not LT or ST copious bloody discharge (hemorrhagic colitis), intense inflammatory response, may be complicated by hemolytic uremia pediatric diarrhea caused by this strain can be fatal due to acute kidney failure (hemolytic uremic syndrome [HUS]). Pathogenic E. coli Enteroaggregative E. coli (EAggEC) adhesins not characterized non invasive produce ST-like heat-labile plasmidencoded toxin (EAST) and a hemolysin persistent diarrhea in young children without inflammation, no fever Pathogenic E. coli Treatment treatment is based on symptomatology. fluid replacement is the primary treatmen Antibiotics are generally not used except in severe disease or disease that has progressed to a systemic stage (e.g.hemolyticuremia syndrome). Shigella agents of bacillary dysentery Shigella Structure Gram-negative, nonmotile, facultatively anaerobic, non-spore-forming rods failure to ferment lactose or decarboxylate lysine closely related with Escherichia coli Shigella Classification four serogroups with multiple serotypes A (S dysenteriae, 12 serotypes); B (S flexneri, 6 serotypes); C (S boydii, 18 serotypes); D (S sonnei, 1 serotype). Shigella bacillary dysentery--shigellosis Shigella Virulence 1. invasin encoded by large extra-chromosomal elements (plasmids)--Invasion Plasmid Antigens (Ipa) B and C. induces the endocytic uptake of shigellae by M cells, epithelial cells, and macrophages. deform the plasma membrane of contiguous cells. IcsB plasmid-encoded protein lyses the plasma membranes, resulting in intercellular bacterial spread. Shigella Histopathology of acute colitis following peroral infectionwith shigellae Shigella Virulence 2. Endotoxin cause fever, shock, bloody, mucoid stools, and abdominal pain (cramps and tenesmus) . Shigella Virulence 3. exotoxin-- Shiga toxin(vero toxin) chromosomally-encoded neurotoxic, enterotoxic and cytotoxic The toxin inhibits protein synthesis (acting on the 70S ribosome and lysing 28S rRNA). Its enterotoxicity can make the disease clinically appear as a diarrhea. Shigella Diagnosis -- Sampling Positive cultures are most often obtained from blood-tinged plugs of mucus in freshly passed stool specimens obtained during the acute phase of disease Rectal swabs may also be used if the specimen is deposited in a buffered glycerol saline holding solution Shigella Diagnosis -- Isolation primary differential/se lective media: SalmonellaShigella (SS) Agar(contain bile salts& pH indicators) MacConkey, Hektoen Enteric Agar, Shigella Diagnosis -- Isolation colorless, non-lactose-fermenting colonies Secondly tubed slants of Kligler's Iron Agar or Triple Sugar Iron Agar. Shigella species produce an alkaline slant and an acid butt with no bubbles of gas in the agar. Shigella Diagnosis -- Identification slide agglutination tests with antisera for serogroup and serotype confirm the identification polymerase chain reaction (PCR). Enzyme-linked immunosorbent assay (ELISA) Shigella Epidemiology occurring by fecal-oral contact it can be transmitted by infected adult food handlers who contaminate food. Man is the only "reservoir" Shigella Treatment and Control Managing of dehydration is of primary concern. Patients with severe dysentery are usually treated with antibiotics (e.g. ampicillin). Patients respond to antibiotic therapy and disease duration is diminished Salmonella salmonellosis Salmonella Structure & Antigenic Types Gram-negative, flagellated, facultatively anaerobic bacilli three major antigens: H or flagellar antigen; O or somatic antigen; Vi antigen (only a few serovars) Salmonella Virulence Factors (1) the ability to invade cells ---- invasin: Vi (capsular) antigen (2) a complete lipopolysaccharide coat ---- LPS (endotoxin) (3) the ability to replicate intracellularly, (4) possibly the elaboration of toxin(s) Salmonella Salmonella Invasion of intestinal mucosa by Salmonella. Salmonella -- Clinical Manifestations 1) Gastroenteritis--food poisoning Symptoms usually begin 6 to 48 hours after ingestion of contaminated food or water the cardinal manifestation is diarrhea. nausea, vomiting, abdominal cramps, myalgia, headache, fever (38oC to 39oC) and chills are common The duration of fever and diarrhea is usually 2 to 7 days Salmonella -- Clinical Manifestations 2) Septicemia an intermediate stage of infection – no intestinal symptoms and the bacteria cannot be isolated from fecal specimens. it may remain localized in the intestine or disseminate to the bloodstream Salmonella -- Clinical Manifestations 3) Enteric fevers ---- typhoid severe systemic form, may be fatal The best studied enteric fever is typhoid fever, the form mainly caused by S typhi may be preceded by gastroenteritis an incubation period of 10 to 14 days symptoms of enteric fevers are nonspecific:fever, anorexia, headache, myalgias, and constipation Salmonella -- Clinical Manifestations 3) Enteric fevers ---- typhoid primary bacteraemic phase: (7- 10 days of the incubation period ) invade the epithelium spread to mesenteric lymph nodes & throughout the body be taken up by the reticuloendothelial cells infect the liver, spleen, gallbladder, bones, meninges invade bloodstream via thoracic duct Salmonella -- Clinical Manifestations 3) Enteric fevers ---- typhoid second and heavier bacteraemic phase (2-3 weeks) pass into the blood( the onset of the fever and other signs of clinical illness) From the gallbladder a further invasion of the intestine results. Peyer’s patches & other gut lymphoid tissues become involved in an inflammatory reaction infiltration with mononuclear cells followed by necrosis, sloughing and the formation of characteristic typhoid ulcers Salmonella -- Clinical Manifestations 3) Enteric fevers ---- typhoid Onset: 2 weeks/ insidious/ vague early symptoms Progression : the temperature shows a stepladder rise over the 1st week of the illness, remains high for 7-10 days and then falls by lysis during the 3rd or 4th week. physical signs include a relative bradycardia for the height of the fever, hepatomegaly, splenomegaly and often a rash of rose spots. Relapse: shorter and of milder. Complications: severe intestinal haemorrhage and intestinal perforation Salmonella -- Clinical Manifestations 4) The prolonged carrier state continue to excrete the salmonellae for a year or more The bacilli are most commonly present in the gallbladder Salmonella -- laboratory diagnosis Isolation & identification 1 Blood culture the definitive diagnosis of enteric fever most commonly found during the first 7-10 days and during relapses Stool and urine culture In typhoid fever, stool cultures are usually positive form the 2nd week and urine cultures from the 3rd week of the infection. Salmonella-laboratory diagnosis Identification & identification 2 Specimens should be plated on several nonselective and selective agar(EMB) media. Laboratory identification of the genus Salmonella is done by biochemical tests. Salmonella-laboratory diagnosis Identification & identification 3 Biochemical reactions of suspicious colonies are then determined on triple sugar iron agar and lysine-iron agar. serologic type is confirmed by serologic testing. It can be confirmed by antigenic analysis of O and H antigens using polyvalent and specific antisera. Salmonella-laboratory diagnosis Widal test a tube test for determining the quantity of agglutinating antibodies, or agglutinins, in the serum of a patient with typhoid fever Salmonella-laboratory diagnosis-widal test The procedure involves adding a suspension of dead typhoid bacterial cells to a series of tubes containing the patient’s serum, which has been diluted out to various concentrations. After the tubes have been incubated for 30 minutes at 37℃, they are centrifuged and examined to note the amount of agglutination that has occurred. The reciprocal of the highest dilution at which agglutination is seen designated as the antibody titer of patient’s serum. Naturally, the higher the titer, the greater is the antibody response of the individual to the disease Salmonella-laboratory diagnosis-widal test Generally, in typhoid cases, it is valuable that the titre of specific O antibodies is ≥1:80 or the titre of specific H antibodies is ≥1:160. In paratyphoid cases, if the titre of specific H antibodies is ≥1:80, the result is positive. Salmonella-laboratory diagnosis-widal test Interpretation The level of ‘enteric’ antibodies in the healthy population must be known and may be variable. Previous inoculation with TAB(typhoid, paratyphoid A, paratyphoid B)vaccine can give relatively high titres of specific antibodies, as can previous infection, although only the H antibodies tend to persist at detectable levels. Cross-reating antibodies from previous exposure to other salmonellae sometimes confuse the picture. Salmonella-laboratory diagnosis-widal test Interpretation As with other serological tests for acute infections, the usefulness of the Widal test is greatest when a four-fold or greater rise in antibody levels is detected on testing a second specimen of the patient’s serum some days after the first’ by this time the diagnosis has usually been made by isolation of the offending organism from blood culture. The detection of persisting Vi antibody in significant titre may be of limited value in the search for long-term carriers after an outbreak of infection. Salmonella Control and Treatment Vaccines are available for typhoid fever and are partially effective. Typhoid fever and enteric fevers should be treated with antibiotics. VIBRIO Characteristics Gram-negative, highly motile curved rods, polar flagella oxidase-positive most species require 2-3% NaCl or a sea water base for optimal growth tolerant to alkali but not to acid Grow rapidly in the pH ranger 7.4- 9.6 Classification two groups 1.non-halophilic vibrios, including V. cholerae and other species that are able to grow in media without added salt. 2.halophilic vibros: species which do not grow in these media. V. cholerae and V. parahaemolyticus are pathogens of humans. Vibrio cholera History and spread of epidemic cholera classic biotypes/ from 1817 to the early 20th/six global waves "El Tor" biotype / In 1961 / Philippines /seventh global/hemolysins O139 "Bengal" /In 1992/Bangladesh /at least 11 countries in southern Asia Antigenic Variation three distinct O1 biotypes Bengal strain – O139 biotype -- "non- Pathogenesis Cholera Toxin Cholera toxin activates the adenylate cyclase enzyme in cells of the intestinal mucosa leading to increased levels of intracellular cAMP, and the secretion of H20, Na+, K+, Cl-, and HCO3- into the lumen of the small intestine The toxin has been characterized and contains 5 binding (B) subunits of 11,500 daltons, an active (A1) subunit of 23,500 daltons, and a bridging piece (A2) of 5,500 daltons that links A1 to the 5B subunits. Pathogenesis -- Cholera Toxin Colonization of the Small Pathogenesis Intestine determinants of the colonization : adhesins: fimbriae Tcp pili, hemagglutinin , acf (accessory colonization factor) genes motility: polar flagella LPS Clinical Manifestations "rice-water stool" Immunity to Cholera Secretory IgA, as well as IgG and IgM in serum exudate, can be detected in the intestinal mucosa of immune individuals. Vibriocidal antibodies reach a peak 8-10 days after the onset of clinical illness, and then decrease, returning to the baseline 2 - 7 months later. Diagnosis rapid diagnosis -wet mount of liquid stool is examined microscopically. culture of stool or rectal swab samples on TCBS agar (yellow colonies) and other selective and nonselective slide agglutination test of colonies with specific antiserum fermentation tests (oxidase positive) fluorescent antibody tests PCR Treatment & Control rapid intravenous replacement Most antibiotics and chemotherapeutic agents have no value in cholera therapy. A parenteral vaccine of whole killed bacteria has been used widely Vibrio parahaemolyticus a halophilic (salt-loving) vibrio associated with enteritis acquired by ingestion of raw or improperly cooked seafoods.. Morphology won’t grow in the absence of sodium chlorid. Strains from clinical specimens generally form green, nonsucrose-fermenting colonies on TCBS agar. Strains associated with gastroenteritis usually cause haemolysis of human red cells in Wagatsuma’s agar, a special medium containing mannitol. This haemolysis is known as the Kanagawa phenomenon Pathogensis Kanagawa-positive strains produce a heat-stable cytotoxin and adhere to human intestinal cells . A heat-lable haemolysin and causes mophologyical changes in tissue culture cells resembling those caused by cholera toxin and the heat-labile enterotoxin of Esch. coli. Diseases and Treatment V. parahaemolyticus can cause explosive diarrhoea, but symptoms usually abate after 3 days Patients with diarrhoea generally require only fluid replacement therapy.