overviews-ii. & iii. committees ii. committee
advertisement

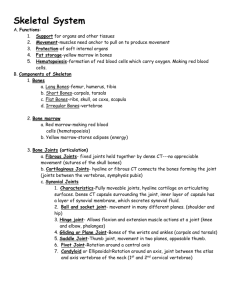
OVERVIEWS-II. & III. COMMITTEES II. COMMITTEE Introduction to anatomy Definition of anatomy Anatomy is the setting (structure) in which the events (functions) of life occur. a branch of morphology that deals with the structure of organisms http://www.merriamwebster.com/medical/anatomy Etymology: “Cutting through” in Ancient Greek and Latin. Anatomy deals with parts of the human body and investigates the body by the naked eye. Types of anatomy 1. Regional (topographical) anatomy 2. Systematic anatomy 3. Clinical (applied) anatomy In systematic anatomy, various structures may be separately considered. On the other hand, in topographical or regional anatomy, the organs and tissues may be studied in relation to one another. Surface anatomy is an essential part of the study of regional anatomy. Clinical (applied) anatomy emphasizes aspects of bodily structure and function important in the practice of medicine, dentistry, and the allied health sciences. It incorporates the regional and systemic approaches to studying anatomy and stresses clinical application. The importance of learning anatomy as a futue medical doctor: -To understandbodily function and how both structure and function are modified by disease. -To interpret the images that are produced by the sophisticated imaging techniques, such as CT, MRI, DTI. -To understand the pathway for targeting therapy to a specific site -To examine the patient properly -To communicate with the colleagues properly The ways of learning anatomy Cadaver Dissection Prosection Other materials of learning human anatomy: anatomy models, anatomy atlases, videos, textbooks, charts, medical dictionaries, etc. The field of Human Anatomy has a prestigious history, and is considered to be the most prominent of the biological sciences of the 19th and early 20th centuries. The final major anatomist of ancient times was Galen (of Bergama), active in the 2nd century. His collection of drawings, based mostly on dog anatomy, became the anatomy textbook for 1500 years. Andreas Vesalius is the first modern anatomist who wrote the first anatomy textbook of the modern times; De humani corporis fabrica (On the Fabric of the Human Body. Anatomical position: All anatomical descriptions are expressed in relation to one consistent position, ensuring that descriptions are not ambiguous. head, gaze (eyes), and toes directed anteriorly (forward), arms adjacent to the sides with the palms facing anteriorly, and lower limbs close together with the feet parallel. Variations: Occasionally a particular structure demonstrates so much variation within the normal range that the most common pattern is found less than half the time! Terminology in anatomy It is important for medical personnel to have a sound knowledge and understanding of the basic anatomic terms. With the aid of a medical dictionary, you will find that understanding anatomic terminology greatly assists you in the learning process. Anatomical planes: All descriptions of the human body are based on the assumption that the person is standing erect, with the upper limbs by the sides and the face and palms of the hands directed forward. This is the so-called anatomic position. The various parts of the body are then described in relation to certain imaginary planes. Median, sagittal, frontal-coronal, and transverse-axial) that intersect the body in the anatomical position. The sagittal plane, like an arrow, divides the body into right and left, coronal anterior to posterior, and axial superior to inferior parts. With reference to the anatomical planes: Superior inferior anterior posterior medial lateral Relating primarily to the body's surface: Superficial, intermediate, and deep (Lat. profundus, profunda) external internal proximal distal Terms of laterality: Unilateral and bilateral, ipsilateral and contralateral 1 OVERVIEWS-II. & III. COMMITTEES Terms of movemement: Flexion extension abduction adduction circumduction (medial and lateral) rotation Pronation, supination, eversion, inversion, opposition, reposition, elevation, depression Positions of the body: The supine position of the body is lying on the back. The prone position is lying face downward Introduction to systematic anatomy Trillions of the cells in the human body form tissues, and tissues make up the 78 organs in the body. The organs serving for the same function are organized under 12 systems (some say 13, counting the vestibular system; which contributes to our balance and our sense of spatial orientation not under the nervous system, but separately). 1. Integumentary system 2. Skeletal System 3. Articular system 4. Muscular System 5. Cardiovascular (Circulatory) System 6. Lymphatic system 8. Digestive (Alimentary) System 9. Urinary (Excretory) System 10. Reproductive (Genital) System 11. Endocrine System 12. Nervous system None of the systems functions in isolation. The passive skeletal and articular systems and the active muscular system collectively constitute a supersystem, the locomotor system, because they must work together to produce locomotion of the body. Although the structures directly responsible for locomotion are the muscles, bones, joints, and ligaments of the limbs, other systems are indirectly involved as well. Bones are organs, and along with the cartilages form the skeletal system. The articular system consists of joints and their associated ligaments, connecting the bony parts of the skeletal system and providing the sites at which movements occur. The three types of muscle can be characterized by whether they are controlled voluntarily or involuntarily, whether they appear striated (striped) or smooth, and whether they are associated with the body wall (somatic), or with organs and blood vessels (visceral). The Circulatory (Cardiovascular) System transports fluids throughout the body. The heart and blood vessels make up the blood transportation network, the cardiovascular system. The heart pumps blood throughout the body, and the blood vessels, which are a closed network of tubes that transport the blood. There are three types of blood vessels: arteries, veins, capillaries. The respiratory system consists of air passages & lungs. The respiratory system supplies oxygen to the blood and eliminates carbon dioxide from it. The thorax is an irregularly shaped cylinder with a narrow opening (superior thoracic aperture) superiorly and a relatively large opening (inferior thoracic aperture) inferiorly. The superior thoracic aperture is open, allowing continuity with the neck; the inferior thoracic aperture is closed by the diaphragm. The diaphragm forms a section between thorax and abdomen. The digestion starts in the mouth. Most of the digestive organs are localized in the abdomen. The abdominal wall covers a large area. It is bounded superiorly by the xiphoid process (the third-most inferior part- of the sternum) and costal margins, posteriorly by the vertebral column, and inferiorly by the upper parts of the pelvic bones. The urinary (excretory) system consists of the kidneys, ureters, urinary bladder, and urethra, which filter blood and subsequently produce, transport, store, and intermittently excrete urine (liquid waste). The two bean-shaped kidneys are located in the posterior abdominal region. The ureters are muscular tubes that transport urine from the kidneys to the bladder.The ureters descend down to the pelvis exiting from the kidneys on each side. They enter the pelvic cavity, and continue their journey to the bladder. The reproductive tracts are located in the pelvic cavity. The pelvic cavity, between the pelvic inlet superiorly and the pelvic diaphragm inferiorly, contains the terminal parts of the urinary and digestive systems, the internal genital organs, the associated vascular structures, and the nerves supplying both the pelvis and lower limbs. 2 OVERVIEWS-II. & III. COMMITTEES The endocrine system consists of specialized structures that secrete hormones, including discrete ductless endocrine glands (such as the thyroid gland), isolated and clustered cells of the gut and blood vessel walls, and specialized nerve endings. The central nervous system (CNS) has two parts: the brain and the spinal cord.The peripheral nervous system (PNS) is the remainder of the nervous system outside of the CNS. The peripheral nervous system (PNS) consists of nerve fibers and cell bodies outside the CNS that conduct impulses to or away from the CNS. The PNS is organized into nerves that connect the CNS with peripheral structures. Introduction to regional anatomy Regional anatomy (topographical anatomy) considers the organization of the human body as major parts or segments: a main body, consisting of the head, neck, and trunk (subdivided into thorax, abdomen, back, and pelvis/perineum), and paired upper limbs and lower limbs. All the major parts may be further subdivided into areas and regions. Cavities in the body Dorsal Body Cavities Cranial cavity & vertebral cavity Ventral Body Cavities Thoracic cavity & abdominopelvic cavity Diaphragm: divides body cavity into thoracic and abdominopelvic cavities. Regions in the body Anatomists have divided the body into several regions. These regions help localize disease names, surgeries, and have other medical implications. The head (cranial region; made by the cranium) is the superior part of the body that is attached to the trunk by the neck. The head is composed of a series of compartments, which are formed by bone and soft tissues. They are: the cranial cavity; two ears; two orbits; two nasal cavities; and an oral cavity The cranial cavity is the largest compartment and contains the brain and associated membranes (meninges). The neck (cervical region; skeleton of the neck is made up by the 7 cervical vertebrae) is the transitional area between the head and the trunk. The neck extends from the head above to the shoulders and thorax below. • Upper limb – includes the hand, wrist, forearm, elbow, arm, and shoulder. Shoulder: proximal segment of the limb that overlaps parts of the trunk (thorax and back) and lower lateral neck. The axilla is the gateway to the upper limb, providing an area of transition between the neck and the arm. Arm (L. brachium): first segment of the free upper limb (more mobile part of the upper limb independent of the trunk) and the longest segment of the limb. It extends between and connects the shoulder and the elbow. It includes one bone. Forearm (L. antebrachium): second longest segment of the limb. It extends between and connects the elbow and the wrist (L. carpus). There are two bones in the forearm. Hand (L. manus): part of the upper limb distal to the forearm. It is composed of the wrist, palm, dorsum of hand, and digits (fingers, including an opposable thumb). • Thorax – the region of the chest from the thoracic inlet to the thoracic diaphragm. • Abdomen- the part of the trunk between the thorax and the pelvis. It is a flexible, dynamic container, housing most of the organs of the alimentary system and part of the urogenital system. Containment of the abdominal organs and their contents is provided by musculoaponeurotic walls anterolaterally, the diaphragm superiorly, and the muscles of the pelvis inferiorly. • Back – consists of the posterior aspect of the body and provides the musculoskeletal axis of support for the trunk. Bony elements consist mainly of the vertebrae. The back contains the spinal cord and proximal parts of the spinal nerves, which send and receive information to and from most of the body. • Pelvis and Perineum – the pelvis consists of everything from the pelvic inlet to the pelvic diaphragm. The perineum is the region between the sex organs and the anus. 3 OVERVIEWS-II. & III. COMMITTEES • Lower limb – everything below the inguinal ligament, including the hip, the thigh, the knee, the leg, the ankle, and the foot. The gluteal region (G. gloutos, buttocks) is the transitional region between the trunk and free lower limbs. The femoral region (thigh) is the region of the free lower limb that lies between the gluteal, abdominal, and perineal regions proximally and the knee region distally. It includes one bone. The knee region is the transitional area between the thigh and the leg. The posterior region of the knee (L. poples) is called the popliteal fossa. The leg region is the part that lies between the knee and the narrow, distal part of the leg. The leg (L., crus) connects the knee and foot. Often laypersons refer incorrectly to the entire lower limb as “the leg.” There are two bones in the leg. The ankle region (L. tarsus) or talocrural region (L. regio talocruralis) is the region where the foot and the leg met. The foot (L. pes) or foot region (L. regio pedis) is the distal part of the lower limb. Introduction to Osteology Osteology (Gk, osteon, bone, logos, science) is the branch of medicine concerned with the development and diseases of bone tissue. The human skeleton is composed of 270 bones in the newborn, 222 bones in children and 206 bones in adults. • The axial skeleton consists of the bones of the head (cranium or skull), neck (hyoid bone and cervical vertebrae), and trunk (ribs, sternum, vertebrae, and sacrum). • The appendicular skeleton consists of the bones of the limbs, including those forming the pectoral (shoulder) and pelvic girdles. Bone is a living tissue capable of changing its structure as the result of the stresses to which it is subjected. Like other connective tissues, bone consists of cells, fibers, and matrix. It is one of the hardest structures of the animal body, because of the calcification of its extracellular matrix. Living bones have some elasticity (results from the organic matter) and great rigidity (results from their lamellous structures and tubes of inorganic calcium phosphate). The skeleton is composed of cartilages and bones. Cartilage is a resilient, semirigid form of connective tissue that forms parts of the skeleton where more flexibility is required—for example, where the costal cartilages attach the ribs to the sternum. Cartilage is an avascular form of connective tissue consisting of extracellular fibers embedded in a matrix that contains cells localized in small cavities. Bone is a calcified, living, connective tissue that forms the majority of the skeleton. It consists of an intercellular calcified matrix, which also contains collagen fibers, and several types of cells within the matrix. Bone has a protective function; the skull and vertebral column, for example, protect the brain and spinal cord from injury; the sternum and ribs protect the thoracic and upper abdominal viscera. It serves as a lever, as seen in the long bones of the limbs, and as an important storage area for calcium salts. It houses and protects within its cavities the delicate blood-forming bone marrow. A fibrous connective tissue covering which is called periosteum surrounds each skeletal element like a sleeve, except where articular cartilage occurs; whereas that around cartilage is perichondrium. The periosteum and perichondrium nourish the external aspects of the skeletal tissue. They are capable of laying down more cartilage or bone (particularly during fracture healing) and provide the interface for attachment of tendons and ligaments. Long bones develop by replacement of hyaline cartilage plate (endochondral ossification). They have a shaft (diaphysis) and two ends (epiphyses). The metaphysis is a part of the diaphysis adjacent to the epiphyses. The diaphysis encloses the marrow cavity. There are two types of bones according to histological features: • compact bone • spongy (trabecular) bone Spongy bone is found at the expanded heads of long bones and fills most irregular bones. Compact bone forms the outer shell of all bones and also the shafts in long bones. Bones are classified according to their shape (gross anatomy): 1) Long bones are tubular (e.g., the humerus in the arm). 2) Short bones are cuboidal and are found only in the tarsus (ankle) and carpus (wrist). 4 OVERVIEWS-II. & III. COMMITTEES 3) Flat bones usually serve protective functions (e.g., the flat bones of the cranium protect the brain). 4) Irregular bones have various shapes other than long, short, or flat (e.g., bones of the face). 5) Sesamoid bones (e.g., the patella or knee cap) develop in certain tendons and are found where tendons cross the ends of long bones in the limbs; they protect the tendons from excessive wear and often change the angle of the tendons as they pass to their attachments. Bone markings appear wherever tendons, ligaments, and fascias are attached or where arteries lie adjacent to or enter bones. Other formations occur in relation to the passage of a tendon (often to direct the tendon or improve its leverage) or to control the type of movement occurring at a joint. Surfaces of the bones are not smooth. Bones display elevations, depressions and holes. The surface features on the bones are given names to distinguish and define them. Bones are richly supplied with blood vessels. Most apparent are the nutrient arteries (one or more per bone) that arise as independent branches of adjacent arteries outside the periosteum and pass obliquely through the compact bone of the shaft of a long bone via nutrient foramina. Veins accompany arteries through the nutrient foramina. Nerves accompany blood vessels supplying bones. The periosteum is richly supplied with sensory nerves—periosteal nerves—that carry pain fibers. Introduction to Skull & Neurocranium The skeleton of the head is the skull. We rather use the ancient Greek term “cranium”, e.g. the cranial nerves. The skull has 22 bones, excluding the ossicles of the ear. Except for the mandible, which forms the lower jaw, the bones of the skull are attached to each other by sutures, are immobile, and form the cranium. The part that is covering the cranial cavity and the brain in it is called neurocranium. The skeleton of the face is called viscerocranium or facial skeleton. It is the lower part of the cranium. Out of the 22 bones in the skull, 8 of them are in the neurocranium. They are: • 1 Frontal bone; the bone in the front of the head • 1 Occipital bone; the bone at the back of the head • 2 Parietal bones; “paries” means wall, and these though bones are on the lateral sides of the skull. • 2 Temporal bones; “temple” has two meanings “time” and “temple”. Time can make more sense for the temporal bones, as where they are the hair becomes grey first. • 1 Sphenoid bone in the middle (Greek sphēnoeidēs wedge-shaped) • 1 Ethmoid bone again in the middle (In Moore’s textbook it is part of the facial skeleton,though) The skeleton of your face is made up by the remaining 14 bones of the cranium. The inferior and anterior parts of the frontal lobes of the brain occupy the anterior cranial fossa, the shallowest of the three cranial fossae. The fossa is formed by the frontal bone anteriorly, the ethmoid bone in the middle, and the body and lesser wings of the sphenoid posteriorly. The butterfly-shaped middle cranial fossa has a central part composed of the sella turcicae on the body of the sphenoid and large, depressed lateral parts on each side. The bones forming the lateral parts of the fossa are the greater wings of the sphenoid and squamous parts of the temporal bones laterally and the petrous parts of the temporal bones posteriorly. The posterior cranial fossa, the largest and deepest of the three cranial fossae is formed mostly by the occipital bone, but the dorsum sellae of the sphenoid marks its anterior boundary centrally and the petrous and mastoid parts of the temporal bones contribute its anterolateral “walls.” Sutura is that form of articulation where the contiguous margins of the bones are united by a thin layer of fibrous tissue; it is met with only in the skull. The major suturae in the skull are; coronal, lambdoid, and sagittal suturues. The bones of the calvaria of a newborn infant are separated by membranous intervals. They include the anterior and posterior fontanelles and the paired sphenoidal and mastoid fontanelles. Skull (Splanchocranium) The skeleton of your face is made up by the remaining 14 bones of the cranium. They are: • Two Nasal bones • Two Maxillæ • Mandible • Two Lacrimal bones • Two Zygomatic bones 5 OVERVIEWS-II. & III. COMMITTEES • Two Palatines • Two Inferior Nasal Conchæ • Vomer The viscerocranium forms the anterior part of the cranium and consists of the bones surrounding the mouth (upper and lower jaws), nose/nasal cavity, and most of the orbits (eye sockets or orbital cavities). The viscerocranium consists of 14 irregular bones: 2 singular bones centered on or lying in the midline (mandible and vomer) and 6 bones occurring as bilateral pairs (maxillae; inferior nasal conchae; and zygomatic, palatine, nasal, and lacrimal bones). Vertebral Column, Ribs and Sternum VERTEBRAL COLUMN The vertebrae and intervertebtal (IV) discs collectively make up the vertebral column (spine), the skeleton of the neck and back that is the main part of the axial skeleton (i.e., articulated bones of the cranium, vertebral column, ribs, and sternum). The vertebral column extends from the cranium (skull) to the apex of the coccyx. The vertebral column is flexible because it consists of many relatively small bones, called vertebrae (singular = vertebra), that are separated by resilient intervertebral (IV) discs. The vertebral column in an adult typically consists of 33 vertebrae arranged in five regions: 7 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 4 coccygeal. The vertebrae gradually become larger as the vertebral column descends to the sacrum and then become progressively smaller toward the apex of the coccyx. Vertebrae vary in size and other characteristics from one region of the vertebral column to another, and to a lesser degree within each region; however, their basic structure is the same. A typical vertebra consists of a vertebral body, a vertebral arch, and seven processes. Regional variations in the size and shape of the vertebral canal accommodate the varying thickness of the spinal cord. Cervical vertebrae form the skeleton of the neck. The smallest of the 24 movable vertebrae, the cervical vertebrae are located between the cranium and the thoracic vertebrae. Their smaller size reflects the fact that they bear less weight than do the larger inferior vertebrae. The most distinctive feature of each cervical vertebra is the oval foramen transversarium (transverse foramen) in the transverse process. The thoracic vertebrae are in the upper back and provide attachment for the ribs. Thus the primary characteristic features of thoracic vertebrae are the costal facets for articulation with ribs. The middle four thoracic vertebrae (T5-T8) demonstrate all the features typical of thoracic vertebrae. Lumbar vertebrae are in the lower back between the thorax and sacrum. Because the weight they support increases toward the inferior end of the vertebral column, lumbar vertebrae have massive bodies, accounting for much of the thickness of the lower trunk in the median plane. The wedged-shaped sacrum (L. sacred) is usually composed of five fused sacral vertebrae in adults. It is located between the hip bones and forms the roof and posterosuperior wall of the posterior half of the pelvic cavity. The coccyx (tail bone) is a small triangular bone that is usually formed by fusion of the four rudimentary coccygeal vertebrae, although in some people, there may be one less or one more. Coccygeal vertebra 1 (Co1) may remain separate from the fused group. RIBS Ribs (L. costae) are curved, flat bones that form most of the thoracic cage. They are remarkably light in weight yet highly resilient. Each rib has a spongy interior containing bone marrow (hematopoietic tissue), which forms blood cells. There are three types of ribs that can be classified as typical or atypical: • True (vertebrocostal) ribs (1st-7th ribs): They attach directly to the sternum through their own costal cartilages. • False (vertebrochondral) ribs (8th, 9th, and usually 10th ribs): Their cartilages are connected to the cartilage of the rib above them; thus their connection with the sternum is indirect. • Floating (vertebral, free) ribs (11th, 12th, and sometimes 10th ribs): The rudimentary cartilages of these ribs do not connect even indirectly with the sternum; instead they end in the posterior abdominal musculature. Typical ribs (3rd-9th) have the following components: 6 OVERVIEWS-II. & III. COMMITTEES Head: wedge-shaped and has two facets. Neck: connects the head of the rib with the body at the level of the tubercle. Tubercle: located at the junction of the neck and body. Body (shaft): thin, flat, and curved, most markedly at the costal angle. STERNUM The sternum (G. sternon, chest) is the flat, elongated bone that forms the middle of the anterior part of the thoracic cage. It directly overlies and affords protection for mediastinal viscera in general and much of the heart in particular. The sternum consists of three parts: manubrium, body, and xiphoid process. III. COMMITTEE Bones of the Upper Limb The upper limb is characterized by its mobility and ability to conduct fine motor skills (manipulation). These characteristics are especially marked in the hand. One of the major functions of the hand is to grip and manipulate objects. Based on the position of its major joints and component bones, the upper limb is divided into shoulder, arm, forearm, and hand for precise description. The superior appendicular skeleton articulates with the axial skeleton only at the sternoclavicular joint, allowing great mobility. The clavicles and scapulae of the pectoral girdle are supported, stabilized, and moved by axioappendicular muscles that attach to the relatively fixed ribs, sternum, and vertebrae of the axial skeleton. The clavicle is the only bony attachment between the trunk and the upper limb. The medial end is called “sternal end". The lateral end is called “acromial” end”. The scapula lies on the posterolateral aspect of the thorax. It has medial, lateral, and superior borders and superior, lateral, and inferior angles. The posterior surface of the scapula is unevenly divided by spine of the scapula, into a small supraspinous fossa and a much larger infraspinous fossa. The spine continues laterally as the flat expanded acromion, which forms the subcutaneous point of the shoulder and articulates with the acromial end of the clavicle. The concave costal surface of most of the scapula forms a large subscapular fossa. The skeletal support for the arm is the humerus. The humerus (arm bone) articulates with the scapula at the glenohumeral joint and the radius and ulna at the elbow joint. The proximal end of the humerus has a head, surgical and anatomical necks, and greater and lesser tubercles. The distal end of the humerus has a condyle, two epicondyles, and three fossae. Ulna is the medial and longer of the two forearm bones. It is the stabilizing bone of the forearm. Radius is the lateral and shorter of the two forearm bones. The hand is the region of the upper limb distal to the wrist joint. It is subdivided into three parts: wrist, (carpus); metacarpus; digits (five fingers including the thumb). Introduction to arthrology Arthrology (Greek a rqron joint –logy) is the science concerned with the anatomy, function, dysfunction and treatment of joints. Joints (articulations) are unions or junctions between two or more bones or rigid parts of the skeleton. Joints exhibit a variety of forms and functions.Joints are classified according to the tissues that lie between the bones: fibrous joints, cartilaginous joints, and synovial joints. Fibrous joints: The bones are united by fibrous tissue. Cartilaginous joints: The bones are united by hyaline cartilage or fibrocartilage. In primary cartilaginous joints, or synchondroses, the bones are united by hyaline cartilage, which permits slight bending during early life. Secondary cartilaginous joints, or symphyses, are strong, slightly movable joints united by fibrocartilage. The fibrocartilaginous intervertebral discs between the vertebrae consist of binding connective tissue that joins the vertebrae together. Synovial joints: The bones are united by a joint (articular) capsule (composed of an outer fibrous layer lined by a serous synovial membrane) spanning and enclosing an articular cavity. Synovial joints are the most common type of joints and provide free movement between the bones they join; they are joints of locomotion, typical of nearly all limb joints. A synovial joint has three common features: 1) Joint cavity, 2) Articular cartilage, 3) Articular capsule. 7 OVERVIEWS-II. & III. COMMITTEES The six major types of synovial joints are classified according to the shape of the articulating surfaces and/or the type of movement they permit: 1. Plane joints (gliding joints) permit gliding or sliding movements in the plane of the articular surfaces. Most plane joints move in only one axis, hence they are called uniaxial joints. 2. Hinge joints (ginglymus, trochlear joints) also uniaxial and permits flexion and extension only, around the transverse axis. 3. Saddle joints permit abduction and adduction as well as flexion and extension, movements occurring around two axes at right angles to each other; biaxial joints. 4. Condyloid (ellipsoid type) joints permit flexion and extension as well as abduction and adduction; thus condyloid joints are also biaxial. 5. Ball and socket joints (enarthrosis, spheroidal joint) allow movement in multiple axes and planes: flexion and extension, abduction and adduction, medial and lateral rotation, and circumduction; thus ball and socket joints are multi-axial joints. 6. Pivot joints permit rotation around a central axis; thus they are uniaxial. The rounded part of a bone rotates in a sleeve or ring like osteofibrous structure. Joints of the Upper Limb Movement of the pectoral girdle involves the sternoclavicular, acromioclavicular, and glenohumeral joints, usually all moving simultaneously. Functional defects in any of the joints impair movements of the pectoral girdle. Mobility of the scapula is essential for free movement of the upper limb. The clavicle forms a strut that holds the scapula, and hence the glenohumeral joint, away from the thorax so it can move freely. Sternoclavicular joint: the only articulation between the upper limb and the axial skeleton. The sternal end of the clavicle articulates with the manubrium and a small part of the 1st costal cartilage. Saddle type, but functions as a ball-and-socket joint. Acromioclavicular joint: The acromial end of the clavicle articulates with the acromion of the scapula. Plane type. Glenohumeral (Shoulder) joint: More freedom of movement than any other joint in the body. Humeral head articulates with the relatively shallow glenoid cavity of the scapula, which is deepened slightly but effectively by the glenoid labrum (L., lip). Ball-and-socket type of synovial joint. Elbow joint: The spool-shaped trochlea and spheroidal capitulum of the humerus articulate with the trochlear notch of the ulna and the slightly concave superior aspect of the head of the radius, respectively; therefore, there are humeroulnar and humeroradial articulations. Hinge type Proximal (Superior) radio-ulnar joint: The head of the radius articulates with the radial notch of the ulna. Pivot type. Distal (Inferior) radio-ulnar joint: The head of the ulna articulates with the ulnar notch on the medial side of the distal end of the radius.Pivot type. Wrist (Radiocarpal) joint: The wrist (carpus), the proximal segment of the hand, is a complex of eight carpal bones, articulating proximally with the forearm via the wrist joint and distally with the five metacarpals. The ulna does not participate in the wrist joint. The distal end of the radius and the articular disc of the distal radio-ulnar joint articulate with the proximal row of carpal bones, except for the pisiform. Condyloid (ellipsoid) type. Intercarpal joints: Carpal bones (the intercarpal joints interconnect the carpal bones). Plante type. Carpometacarpal joints: The distal surfaces of the carpals of the distal row articulate with the carpal surfaces of the bases of the metacarpals. The important carpometacarpal joint of the thumb is between the trapezium and the base of the 1st metacarpal; it has a separate articular cavity. Like the carpals, adjacent metacarpals articulate with each other. The carpometacarpal and intermetacarpal joints are the plane type of synovial joint, except for the carpometacarpal joint of the thumb, which is a saddle joint. The metacarpophalangeal joints are the condyloid type of synovial joint that permit movement in two planes: flexion-extension and adduction-abduction. The interphalangeal joints are the hinge type of synovial joint that permit flexionextension only. The heads of the metacarpals articulate with the bases of the proximal phalanges, and the heads of the phalanges articulate with the bases of more distally located phalanges. 8 OVERVIEWS-II. & III. COMMITTEES Skeleton of the Pelvis In common usage, the pelvis (L. basin) is the part of the trunk inferoposterior to the abdomen and is the area of transition between the trunk and the lower limbs. The bones of the pelvis consist of the right and left pelvic (hip) bones, the sacrum, and the coccyx. The pelvic girdle is a basin-shaped ring of bones that connects the vertebral column to the two femora. The pelvic girdle is strong and rigid, especially compared to the pectoral (shoulder) girdle. The pelvic bone is irregular in shape and has two major parts separated by an oblique line on the medial surface of the bone: pelvic bone above this line represents the lateral wall of the false pelvis, which is part of the abdominal cavity; pelvic bone below this line represents the lateral wall of the true pelvis, which contains the pelvic cavity. In the mature individual, the pelvic girdle is formed by three bones: Right and left hip bones (coxal bones; pelvic bones): large, irregularly shaped bones, each of which develops from the fusion of three bones, the ilium, ischium, and pubis. Sacrum: formed by the fusion of five, originally separate, sacral vertebrae. The ilium is the superior, fan-shaped part of the hip bone. The ala iliaca, wing of the ilium represents the spread of the fan, and the body of the ilium, the handle of the fan. On its external aspect, the body participates in formation of the acetabulum. The entire superior margin of the ilium is thickened to form a prominent crest (iliac crest), which is the site of attachment for muscles and fascia of the abdomen, back, and lower limb and terminates anteriorly as the anterior superior iliac spine and posteriorly as the posterior superior iliac spine. The ischium has a body and ramus. The body of the ischium helps form the acetabulum and the ramus of the ischium forms part of the obturator foramen. The large posteroinferior protuberance of the ischium is the ischial tuberosity. The small pointed posteromedial projection near the junction of the ramus and body is the ischial spine. The pubis is an angulated bone with a superior ramus, which helps form the acetabulum, and an inferior ramus, which helps form the obturator foramen. The pelvis is divided into greater (false) and lesser (true) pelves by the oblique plane of the pelvic inlet (superior pelvic aperture). The bony edge (rim) surrounding and defining the pelvic inlet is the pelvic brim. The pelvic inlet is the circular opening between the abdominal cavity and the pelvic cavity. Through the pelvic inlet structures traverse between the abdomen and pelvic cavity. It is completely surrounded by bones and joints. The pelvic outlet is diamond shaped, with the anterior part of the diamond defined predominantly by bone and the posterior part mainly by ligaments. The pelvic cavity is a body cavity that is bounded by the bones of the pelvis. Its oblique roof is the pelvic inlet (the superior opening of the pelvis). Its lower boundary is the pelvic floor. The pelvic cavity primarily contains reproductive organs, the urinary bladder, the pelvic colon, and the rectum. The linea terminalis consists of the the arcuate line, the pecten pubis or pectineal line, and the pubic crest. It is part of the pelvic brim, which is the edge of the pelvic inlet. The primary joints of the pelvic girdle are the sacroiliac joints and the pubic symphysis. The sacroiliac joints link the axial skeleton (skeleton of the trunk, composed of the vertebral column at this level) and the inferior appendicular skeleton (skeleton of the lower limb). The lumbosacral and sacrococcygeal joints, although joints of the axial skeleton, are directly related to the pelvic girdle. Strong ligaments support and strengthen these joints. The sacroiliac joints are strong, weight-bearing compound joints, consisting of an anterior synovial joint (between the earshaped auricular surfaces of the sacrum and ilium, covered with articular cartilage) and a posterior syndesmosis (between the tuberosities of the same bones). Weight is transferred from the axial skeleton to the ilia via the sacroiliac ligaments, and then to the femurs during standing, and to the ischial tuberosities during sitting. The sacrum is actually suspended between the iliac bones and is firmly attached to them by posterior and interosseous sacroiliac ligaments. The pubic symphysis is a secondary cartilaginous joint which consists of a fibrocartilaginous interpubic disc and surrounding ligaments uniting the bodies of the pubic bones in the median plane. The ligaments joining 9 OVERVIEWS-II. & III. COMMITTEES the bones are thickened at the superior and inferior margins of the symphysis, forming superior and inferior pubic ligaments. L5 and S1 vertebrae articulate at the anterior intervertebral (IV) joint formed by the L5/S1 IV disc between their bodies and at two posterior zygapophysial joints (facet joints) between the articular processes of these vertebrae as lumbosacral joints. The sacrococcygeal joint is a secondary cartilaginous joint with an intervertebral disc. Joints of the Vertebral Column The two major types of joints between vertebrae are.symphyses between vertebral bodies (n=2 one above, and one below) and synovial joints between articular processes (n=4, two above and two below). A typical vertebra has a total of six joints with adjacent vertebrae. Each symphysis includes an intervertebral disc. In addition to the joints between adjacent vertebrae, the vertebral column has the following joints below: 1) Craniovertebral (atlanto-axial and atlanto-occipital) joints 2) Costovertebral joints 3) Sacroiliac joints (will be discussed in the Pelvis) The joints of the vertebral bodies are symphyses (secondary cartilaginous joints) designed for weightbearing and strength. The symphysis between adjacent vertebral bodies is formed by a layer of hyaline cartilage on each vertebral body and an intervertebral disc, which lies between the layers. The articulating surfaces are not only connected by intervertebral discs, but by ligaments as well. The intervertebral disc consists of an outer anulus fibrosus, which surrounds a central nucleus pulposus. The semifluid nature of the nucleus pulposus allows it to change shape and permits one vertebra to rock forward or backward on another, as in flexion and extension of the vertebral column. The synovial joints between superior and inferior articular processes on adjacent vertebrae are the zygapophysial (facet) joints. The joints of the vertebral arches; the zygapophysial joints are often called facet joints. These articulations are plane synovial joints between the superior and inferior articular processes (G. zygapophyses) of adjacent vertebrae. The lateral margins of the upper surfaces of typical cervical vertebrae are elevated into crests or lips termed uncinate processes. These may articulate with the body of the vertebra above to form small "uncovertebral" synovial joints (Luschka’s joints). Joints between vertebrae are reinforced and supported by numerous ligaments, which pass between vertebral bodies and interconnect components of the vertebral arches. The anterior and posterior longitudinal ligaments are on the anterior and posterior surfaces of the vertebral bodies and extend along most of the vertebral column. The ligamenta flava, on each side, pass between the laminae of adjacent vertebrae. These thin, broad ligaments consist predominantly of elastic tissue and form part of the posterior surface of the vertebral canal. The supraspinous ligament connects and passes along the tips of the vertebral spinous processes from vertebra C7 to the sacrum. From vertebra C7 to the skull, the ligament becomes structurally distinct from more caudal parts of the ligament and is called the ligamentum nuchae. Interspinous ligaments pass between adjacent vertebral spinous processes. There are two sets of craniovertebral joints, the atlanto-occipital joints, formed between the atlas (C1 vertebra), and the occipital bone of the cranium, and the atlanto-axial joints, formed between the atlas and axis (C2 vertebra). The craniovertebral joints are synovial joints that have no intervertebral discs. Their design gives a wider range of movement than in the rest of the vertebral column. The articulations involve the occipital condyles, atlas, and axis. A typical rib articulates with the bodies of adjacent vertebrae, forming a joint with the head of the rib; and the transverse process of its related vertebra, forming a costotransverse joint. Together, the costovertebral joints and related ligaments allow the necks of the ribs either to rotate around their longitudinal axes, which occurs mainly in the upper ribs, or to ascend and descend relative to the vertebral column, which occurs mainly in the lower ribs. The combined movements of all of the ribs on the vertebral column are essential for altering the volume of the thoracic cavity during breathing. The range of movement of the vertebral column varies according to the region and the individual. The mobility of the vertebral column results primarily from the compressibility and elasticity of the 10 OVERVIEWS-II. & III. COMMITTEES intervertebral discs. The normal range of movement possible in healthy young adults is typically reduced by 50% or more as they age. Although the movement between any two vertebrae is limited, the summation of movement among all vertebrae results in a large range of movement by the vertebral column. Movements by the vertebral column include flexion, extension, lateral flexion, rotation, and circumduction. Movements by vertebrae in a specific region (cervical, thoracic, and lumbar) are determined by the shape and orientation of joint surfaces on the articular processes and on the vertebral bodies. Bones of the Lower Limb The skeleton of the lower limb (inferior appendicular skeleton) may be divided into two functional components: -pelvic girdle -bones of the free lower limb. Body weight is transferred from the vertebral column through the sacroiliac joints to the pelvic girdle and from the pelvic girdle through the hip joints to the femurs (L. femora). To support the erect bipedal posture better, the femurs (better “femora”) are oblique (directed inferomedially) within the thighs so that when standing the knees are adjacent and placed directly inferior to the trunk, returning the center of gravity to the vertical lines of the supporting legs and feet. The femur is the longest and heaviest bone in the body. It transmits body weight from the hip bone to the tibia when a person is standing. Its length is approximately a quarter of the person's height. The femur consists of a shaft (body) and two ends, proximal (superior) and distal (inferior). The patella is the largest sesamoid bone (a bone formed within the tendon of a muscle) in the body and is formed within the tendon of the quadriceps femoris muscle as it crosses anterior to the knee joint to insert on the tibia. The tibia is located on the anteromedial side of the leg, nearly parallel to the fibula. Medial and larger of the two bones in the leg. The only one that articulates with the femur at the knee joint. Second largest bone in the body. Flares outward at both ends to provide an increased area for articulation and weight transfer. Fibula is slender. Lies posterolateral to the tibia. Firmly attached to it by the tibiofibular syndesmosis, which includes the interosseous membrane. No function in weight-bearing. Serves mainly for muscle attachment, providing distal attachment (insertion) for one muscle and proximal attachment (origin) for eight muscles. The bones of the foot include the tarsus, metatarsus, and phalanges. There are 7 tarsal bones, 5 metatarsal bones, and 14 phalanges. The tarsus consists of seven bones: Talus Calcaneus Cuboid Navicular Three cuneiforms. Only one bone, the talus, articulates with the leg bones. Joints of the Lower Limb The joints of the lower limb include the articulations of the pelvic girdle—lumbosacral joints, sacroiliac joints, and pubic symphysis. The remaining joints of the lower limb are the hip joints, knee joints, tibiofibular joints, ankle joints, and foot joints. The hip joint forms the connection between the lower limb and the pelvic girdle. It is a strong and stable joint. Synovial joint type Multiaxial ball and socket type of synovial joint Articular surfaces: The head of the femur is the ball, and the acetabulum is the socket. The round head of the femur articulates with the cup-like acetabulum of the hip bone. Knee joint is the largest and most superficial joint. Synovial joint type hinge type; allowing flexion and extension; however, the hinge movements are combined with gliding and rolling and with rotation about a vertical axis. Articular surfaces The articular surfaces of the knee joint are characterized by their large size and their complicated and incongruent shapes. 11 OVERVIEWS-II. & III. COMMITTEES The tibia and fibula are connected by two joints: the tibiofibular joint and the tibiofibular syndesmosis (inferior tibiofibular) joint. In addition, an interosseous membrane joins the shafts of the two bones. The ankle joint (talocrural articulation) is located between the distal ends of the tibia and the fibula and the superior part of the talus. The trochlea (L., pulley) is the rounded superior articular surface of the talus. The medial surface of the lateral malleolus articulates with the lateral surface of the talus. Hinge-type The many joints of the foot involve the tarsals, metatarsals, and phalanges. The important intertarsal joints are the subtalar (talocalcaneal) joint and the transverse tarsal joint (calcaneocuboid and talonavicular joints). Inversion and eversion of the foot are the main movements involving these joints. The other intertarsal joints (e.g., intercuneiform joints) and the tarsometatarsal and intermetatarsal joints are relatively small and are so tightly joined by ligaments that only slight movement occurs between them. 12