respire ppt
advertisement

How much do you know about …
The Respiratory
System
Website friendly
What does the Respiratory System do?
The respiratory system….
Oversees gas exchanges between the
blood and external environment
Exchange of gasses takes place within the
lungs in the alveoli
Passageways to the lungs purify, warm,
and humidify the incoming air
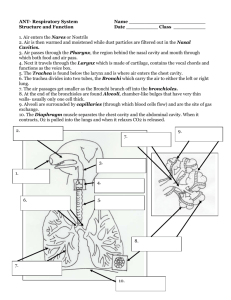
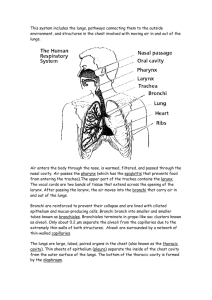
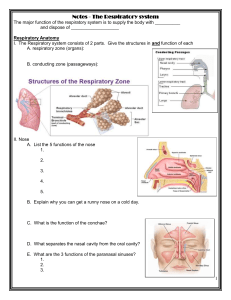
Structures of the Respiratory System
The Nasal Cavity
The Oral Cavity
Pharynx – aka the throat
Epigottis –aka the guardian of
the airways
Larynx – aka the voice box
Trachea – aka the windpipe
Bronchi
Bronchioli
Alveoli
the nose
– nares
the nasal
cavity
– conchae
– the
palate
– the
sinuses
4
The Nose
• Provides airway entry (nares)
• Inflammation of the nasal mucosa is called rhinitis.
5
Nasal cavity
Olfactory receptors located in mucosa on superior
surface.
Nasal septum divides nasal cavity in midline
Connects with pharynx posteriorly through nasopharynx
6
Nasal cavity
Lateral walls have projections called Conchae
Increases surface area
Increases air turbulence within the nasal cavity
Resonating chamber for speech
The nasal cavity is separated from the oral cavity by the Palate
Anterior hard palate (bone)
Posterior soft palate (muscle)
7
Nasal Conchae
•Increases turbulence of air
•3 scroll-like structures
•Reclaims moisture on the way out
8
Paranasal sinuses (open cavities w/in bones around nose)
•Frontal, sphenoid, ethmoid and maxillary bones
•Lined by same mucosa as nasal cavity
•Functions: Lighten the skull, Act as resonance chambers
for speech, Moisten air, & Produce mucus that drains into
the nasal cavity
9
Respiratory Mucosa
• Pseudostratified ciliated
columnar epithelium with
goblet cells.
– goblet cells – secrete
mucous
– Serous cells – secrete watery fluid with antibiotic enzymes,
e.g. lysozyme
– Cilia move the mucus toward the pharynx for swallowing.
• Even when you're healthy, your body makes about a quart of
mucus/day.
• Most of that mucus trickles down your throat and you don't
even notice it.
10
Anatomy of the Respiratory System
• the pharynx
– tonsils
• the larynx
– epiglottis
• the trachea
– C rings
The Pharynx (throat)
Muscular passage from nasal cavity to larynx
Three regions of the pharynx
Nasopharynx – superior region behind nasal cavity
Oropharynx – middle region behind mouth
Laryngopharynx – inferior region attached to larynx
The oropharynx and laryngopharynx are common passageways
for air and food
12
The Pharynx (throat)
• Houses tonsils (they respond to inhaled antigens)
• Uvula closes off nasopharynx during swallowing so food
doesn’t go into nose
• Epiglottis (guardian of the airway) posterior to the tongue:
keeps food out of airway
• Lined with stratified squamous epithelium for protection
• Intrenal Auditory tube enters the nasopharynx
• Tonsils of the pharynx
• Pharyngeal tonsil (adenoids) in the nasopharynx
• Palatine tonsils in the oropharynx
• Lingual tonsils at the base of the tongue
13
The Larynx (voicebox)
• Approx. same level as 4th - 6th cervical vertebrae
• Attaches to hyoid bone superiorly
Three functions:
1. Produces vibrations resulting in speech. {true vocal cords}
2. Provides an open airway (breathing)
3. Switching mechanism to route air and food into
proper channels
• Closed during swallowing
• Open during breathing
14
Framework of the larynx
–8 cartilages connected by membranes and ligaments
–Thyroid cartilage with laryngeal prominence (Adam’s
apple) anteriorly
–Cricoid cartilage inferior to thyroid cartilage: the only
complete ring of cartilage: signet shaped and wide
posteriorly
15
*
Posterior views
Epiglottis
Elastic cartilage attached to thyroid
Cartilage of larynx.
Seen @ back of tongue
During swallowing, it flips inferiorly to
cover and seal laryngeal opening.
Keeps food out of lower respiratory tract
16
Vocal cords (vocal folds)
Vibrate with expelled air to create sound
(speech)
Glottis – opening between vocal cords
17
Trachea (the windpipe)
• Connects larynx with bronchi
•16-20 C-shaped rings of hyaline cartilage joined by
fibroelastic connective tissue
•Flexible for bending but stays open despite pressure
changes during breathing
18
Trachea
• Lined with ciliated mucosa that beat continuously in the
opposite direction of incoming air to expel mucus loaded
with dust and other debris away from lungs
• Carina-Ridge on internal aspect of last tracheal cartilage
•Divides into two main (primary) bronchi
•Surgical opening of the trachea is called
a tracheostomy.
19
Primary Bronchi
Formed by division of the trachea
Enters the lung at the hilus (medial depression)
Right bronchus is wider, shorter, & straighter than left
Bronchi subdivide into smaller & smaller branches –
secondary & tertiary bronchi
Rt. bronchus
is more
common site
for an inhaled
object to get
lodged.
20
Respiratory Tree Divisions
Primary bronchi
Secondary bronchi
Tertiary bronchi
Bronchioli
Terminal bronchioli
Bronchioles
Smallest branches of the bronchi
All but the smallest branches have reinforcing cartilage
Bronchioles
Terminal bronchioles end in alveoli
Alveoli –air sacs
• are specialized for
optimal diffusion
– moist membrane
– large surface area
– thin walls for diffusion
(1 cell thick)
- next to pulmonary
capillaries, which are
also 1 cell thick for gas exchange.
- the inner surface of the alveoli are covered
with a single layer of lipid called surfactant
24
Surfactant
– Surfactant reduces the surface tension in the alveoli allowing
them to easily expand to twice their size with each breath
– it decreases tension b/w the pleural walls.
– Aids in the expansion of the alveoli
• Made of cuboidal epithelial cells are scattered in
alveolar walls
• Without it the walls would stick together during
exhalation
25
Surfactant in Babies
• The first cry of new born is done without the aid of
surfactant
• The 1st breath immediately activates body to
secrete the surfactant & breathing is easier.
• Premature babies – problem breathing is difficult
because lack surfactant. Breathing is assisted until
the baby’s lungs fully develop.
Lungs
(made up of the many subdivisions of the bronchi, bronchioli, & millions of alveoli)
Each is cone-shaped with anterior, lateral and posterior surfaces
contacting ribs
– 3 lobes on the right
– 2 lobes on the left
Apex is near the clavicle (superior portion)
Base rests on the diaphragm (inferior portion)
27
• Hilus or (hilum)
– Indentation on medial surface
– Place where blood vessels, bronchi, lymph vessel, and nerves
enter and exit the lung
• Smallest subdivision seen with the naked eye is the lobule
Medial view R lung
Medial view of L lung
28
Coverings of the Lungs
• Around each lung is a flattened sac of serous membrane
called pleura
• Parietal pleura (outer layer) lines the walls of the
thoracic cavity
• Visceral pleura – directly on lung
Coverings of the Lungs
• Pleural fluid fills the area between layers of pleura to
allow gliding (like film between 2 plates of glass).
• Pleura cling to thoracic wall and are forced to expand and
recoil as volume of thoracic cavity changes during
breathing
• Pleurisy is the swelling/irritation
of the pleura.
Lungs and Pleura
• Pleural cavity – divides thoracic cavity in three parts:
Right & left pleural cavities, & mediastinal cavity.
31
The Respiratory Organs
Conducting zone
– Respiratory passages
that carry air to the
site of gas exchange
– Filters, humidifies and
warms air
Respiratory zone
– Site of gas exchange
– Composed of
• Respiratory
bronchioles
• Alveolar ducts
• Alveolar sacs
Conducting zone labeled
32
Respiratory Zone
• End-point of respiratory tree
• Gas exchange occurs in the alveoli
• There are more than 300 million alveoli making up the lungs
33
Respiration
• Pulmonary ventilation
– Air moves in and out of lungs
– Continuous replacement of gases in alveoli (air sacs)
• External respiration
– Gas exchange between pulmonary blood and air at alveoli
– O2 (oxygen) in air diffuses into blood
Gas Exchange & Transport
– CO2 (carbon dioxide) in blood diffuses into air
• Transport of respiratory gases
– Performed by the cardiovascular system
– Blood is the transporting fluid
– Occurs b/w the lungs and the body tissues
• Internal respiration
– Gas exchange in capillaries between blood and tissue cells
– O2 in blood diffuses into systemic tissues
– CO2 waste in systemic tissues diffuses into blood
34
Cellular Respiration
• metabolic process occurring @ the cellular level in
which ATP is produced from the combination of
glucose & oxygen.
• C6H12O6 + 6O2
6CO2 + 6H2O + 34ATP
• All body cells
• Carbon dioxide (CO2) is produced as a waste
product
• The body’s cells die if either the respiratory or
cardiovascular system fails
36
Ventilation
• Breathing = “pulmonary ventilation”
– Pulmonary means related to the lungs
– Ventilation is air movement
• Two phases
1. Inspiration=inhalation-air in
– diaphragm and intercostal muscles contract
– thoracic cavity expands
2. Expiration=exhalation -air out
– diaphragm and intercostal muscles relax
– thoracic cavity shrinks
37
Ventilation
• Mechanical forces cause ventilation– requires energy.
• Diffusion of gases always flow from area of higher
pressure to areas of low pressure.
• For air to enter the chest, the pressure of the air in the
lungs has to be lower than atmospheric pressure.
38
Muscles of Inspiration
• During inspiration, the dome
shaped diaphragm flattens
as it contracts
Together:
– This increases the height of
the thoracic cavity
• The external intercostal
muscles contract to raise the
ribs
– This increases the
circumference of the thoracic
cavity
39
Inspiration continued
Diaphragm and intercostal muscles contract
The size of the thoracic cavity increases
External air is pulled into the lungs due to an increase in
intrapulmonary volume
40
Expiration
Largely a passive process which depends on
natural lung elasticity
As muscles relax, air is pushed out of the lungs
Forced expiration can occur mostly by
contracting internal intercostal muscles to
depress the rib cage
Expiration
– Rib cage drops under force of gravity
– Relaxing diaphragm moves superiorly (up)
– Elastic fibers in lung recoil
– Volumes of thorax and lungs decrease
simultaneously, increasing the pressure
– Air is forced out
42
Expiration continued
•Forced expiration is active process
–Contraction of abdominal wall muscles
–Internal & External Oblique & Transverse Abdomenus
–Increases intra-abdominal pressure forcing the diaphragm upward.
–Depressing the rib cage, decreases thoracic volume
(try this on yourself to feel the different muscles acting)
43
Pressure Differences in the Thoracic
Cavity
Normal pressure within the pleural space is always
negative – negative feedback system
Differences in lung and pleural space pressures keep
lungs from collapsing
Factors Influencing Respiratory Rate
and Depth
Chemical factors
Carbon dioxide levels
Level of carbon dioxide in the blood is the main
regulatory chemical for respiration
Increased carbon dioxide increases respiration
Changes in carbon dioxide act directly
on the medulla oblongata
Factors Influencing Respiratory
Rate and Depth
Chemical factors (continued)
Oxygen levels
Changes in oxygen concentration in the
blood are detected by chemoreceptors in
the aorta and carotid artery
Information is sent to the medulla oblongata
Carbon Dioxide
• is transported three ways in the blood
– 7% dissolved in the blood plasma
– 23% carried on the hemoglobin molecule as
carbaminohemoglobin (HbCO2)
– 70% is carried as carbonic acid/carbonate ion
equilibrium
Non-respiratory Air Movements
Can be caused by reflexes or voluntary actions
Examples
Cough (clears the lower respiratory passage)
Sneeze (uvula closes the oral cavity off from pharynx in order to clear upper respiratory passage).
Laughing
Crying (involves release of air in # of short breaths, similar to laughing)
Yawn (formerly believed to be triggered by low O )
2
Hiccup (sudden inspiration due to diaphragm spasms)
Respiratory Volumes and Capacities
Normal breathing moves about 500 ml of air with each
breath (tidal volume [TV]) {normal quiet breathing}
Many factors that affect respiratory capacity
A person’s size
Sex
Age
Physical condition
Residual volume of air – after exhalation, about 1200 ml
of air remains in the lungs
Respiratory Volumes and Capacities
Inspiratory reserve volume (IRV)
Amount of air that can be taken in forcibly over the tidal
volume
Usually between 2100 and 3200 ml
Expiratory reserve volume (ERV)
Amount of air that can be forcibly exhaled
Approximately 1200 ml
Respiratory Volumes and Capacities
Residual volume
Air remaining in lung after expiration
About 1200 ml
Respiratory Volumes and Capacities
Vital capacity
The total amount of exchangeable air
Vital capacity = TV + IRV + ERV
Dead space volume
Air that remains in conducting
zone and never reaches alveoli
About 150 ml
Respiratory Volumes and Capacities
Functional volume
Air that actually reaches the respiratory zone
Usually about 350 ml
Respiratory capacities are measured with a
spirometer
• This “air-blood barrier” is where gas exchange occurs.
– The respiratory membrane is also called the air-blood barrier.
– Oxygen diffuses from air in alveolus into pulmonary
blood in capillary
• Carbon dioxide diffuses from the pulmonary blood in the
capillary into the air in the alveolus
54
Air Flow
•
•
•
•
•
•
•
•
•
•
•
•
1. Nose & Mouth
2. Pharynx
(the 3 parts of the pharynx)
nasopharynx
oropharynx
laryngeopharynx
3. Larynx
4. Trachea
5. Primary bronchi (right & left)
6. Secondary bronchi (aka. Bronchiole)
7. Tertiary bronchi (aka. Bronchiole)
8. Alveoli
Respiratory Rate Changes Throughout Life
Newborns (neo-6 wks) – 30 – 60 breath/min
Infants (6wk – 6mo) – 25-40 br/min
Toddler (1- 3 yrs) – 20-30 br/min
Young Children (3 – 6 yrs) – 20 – 25 br/min
Older Children (10 – 14yrs) – 15 – 20 br/min
Adults 15 & up – 12 – 20 br/min
Rate often increases somewhat with old age
Extra Credit Ideas
1.Create a 3-d model of the respiratory system out of
gummy life savers & other food items @ home. Label each
structures & indicate if it is part of the conducting or
respiratory zone.
2.Make a working lung model out of a plastic bottle,
balloons, & straws. Explain how it works.
3.Label the respiratory system on a turtle neck shirt.