final nhepc nutrition health education and patient counseling johali
advertisement

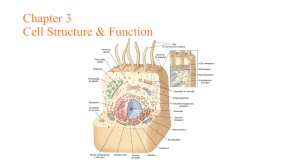
بسم هللا الرحمن الرحيم KINGDOM OF SAUDI ARABIA MINISTRY OF HIGHER EDUCTION KING SAUD UNIVERSITY CAMS \ CHS DEPARTMENT NUTRITION HEALTH EDUCATION & PATIENT COUNSELING The Way To APCHER Healthy Life The Quality Notational Plan Traditional\ unbalanced Habit Promote and Help To …….. The NHEPC 2012 EISA ALI JOHALI CHS456 عيس ى بن علي الجوحلي Johali2012 1 بسم هللا الرحمن الرحيم EISA ALI JOHALI عيس ى بن علي الجوحلي A Lecturer • Bachelor A. M. Sc. Heath Education, KSU 1407 /1987 •Short Fellowship Planning Health Professions Education, UIC, USA 199 •MA (Ed.) Philosophies and Sciences of Teaching, Learning and Curriculum in Nursing, UK 1995 •PhD Health Sciences By Accrediting Prior Experiences, Hill University Sept. 2012 Author of Two Published Books & 3 Projected http://faculty.ksu.edu.sa/JOHALI/default.aspx Johali59@hotmail.com WL Messengers NEHPC2012 http://sa.linkedin.com/pub/eisa-johali/31/3a6/896 https://twitter.com/TheNature2011 Dr. Eisa Johali CHS456 Johali2012 2 CHS456 Promontory ألن الجودة من الحرص واالجتهاد وآلن ”اإلحساس والشعور بمرض ومشكالت ومتاعب اآلخرين“هي غاية كل مسلم مؤمن وهي غايتنا : نستهل مقدمتنا هده بآيات من الذكر الحكيم في التقوى،“ وهي في ”التقوى،في عملنا وتعليمنا طلبا للحسنين ]3 ،2/[الطالق َو َم ْن َي َّت ِق َهللا َي ْج َع ْل َل ُه َم ْخ َر ًجا * َو َي ْر ُز ْق ُه ِم ْن َح ْي ُث َال َي ْح َت ِس ُب .]29/[األنفال َ َ إ ْن َت َّت ُقوا هللا َي ْج َع ْل ل ُك ْم ُف ْر َق ًانا ِ : عن أنس بن مالك رضي هللا عنه، وقول رسوله الكريم نبينا ”محمد“ عليه أفضل الصالة والسالم )( ال يؤمن أحدكم حتى يحب ألخيه ما يحب لنفسه وقوله صلى هللا علية وسلم (كان هللا في عون العبد ما كان العبد في عون أخيه) رواه مسلم وأبو داود والترمذي أخرجه البخاري These Islamic Calls are our Evidences to assure Quality of Profession; Quality of NHEPC & Quality of Life today and for the Day after. Meanwhile, do not forget the most common Arab Proverb: “Nothing Itching Your Skin Like Your Nail” ”“ما يحك جلدك مثل ظفرك Who can itch your skin! Effectively? You or other eg. teacher ? - When you will feel better & - Who can understand better: the Passive student who taught or filled by other the teacher? Or the active student who learn by himself or at least participate /share learning with teacher?. - Thus, what do you prefer /recommend: Be Passive Student & Patient? Or Be Active ? CHS456 Johali2012 3 A CONCISE OF NHEPC The COURSE EDUCATIONAL OBJECTIVES Explore the sciences of health, education, health education from the nature and duties of your profession practice and education courses, Briefly highlight the historical overview of Nutrition Health Education, Probe education ↔ health & briefly highlight philosophical & scientific NHE roots. Well realize the recent HE scientific concepts, methodologies, technologies & planning procedures that can promote the quality of lifelong health. Define Global health education ↔ Create a“ National Definition” which suites our national nature and characters & predict HE Principles, Fields, Communication & Ethics. Be aware of the “Teaching & Learning” methods and technologies that we taught by during our HE study. Distinguish & use the most common HE Methodologies & Technologies, and their major advantages and disadvantages. Discover / Produce / Evaluate some interactive HETechnologies “materials”: Leaflet, Folder, Poster and Pamphlet & Sites… Use the most related scientific concepts to plan an effective HE Activities. Our Overall Goal The Way Ahead Towards “ Assertive Patient Centred HE” with & Best Evidence” (APCHE’R) QUALITY CHS456 Johali2012 4 T & L Introductory As an introductory to this probing “Lectures’ Note”, I would like to send a progressive educational message to my dear “Adult Learners”. My dear learners remember that you are not a primary school pupil neither a an elementary nor even, a secondary student. You are mature adult learners, you should be smart CNs, that in order to success in this progressive course and in your life as well, you have to “Think, Participate, Practice & Reflect on and in… This course is not a traditional that you can just read, store and recall. it is a “Lifelong Learning Guide (LLG)” to help you to think around, back, about, over and up. It is prepared to promote you to search about the most appropriate knowledge, attitude that can lead to the right nutritional behaviors for you, your patients, family and community. This LLG consists of “ ten major learning units”. Before probing the history of ‘EDUCATIONHEALTHQNHEPC\LIFE “‘, you have to reason ‘why you are studying this course. The second and third units promote you to determine the boundaries of the quality of H & E through the modern philosophical and scientific concepts of education and health that can guide you to, the Fourth by which you will distinguish the appropriate methodologies and technologies that can enable you to plan and develop effective health education activities to increase the quality of Patients’ Healthful Life. In order to learn the course well, you have to use "Your All Senses" and "Abilities", as well; You have to attend, see, listen, ask, discuss and participate actively in teaching, learning and assessing your self, your colleague, your teaching and learning process and materials, your curriculum, and your teacher, as well. Finally, if you do so, do not worry, you will success in your course and your life as well. With this Concise & its T&L Plan and Process “All the Learners will success; Except the one Who DO NOT Welling to CHS456 Johali2012 5 Success” NHEPC T & LEARNING PLAN OUR Overall AIM The Way Ahead Towards APCHE’R NHEPC QUALITY “Assertive The Patients Centred HE” with Best Evidence to assure quality of NHEPC CHS456 Johali2012 6 CHS456 T & LEARNING PLAN APCHER Quality NHEPC Weeks Units/Subjects Notes UNDERSTANDING EACH OTHER DISCUSSING THE COURSE OBJECTIVES Via this T& L Plan WHY “NHEPC (The Place of HE in CN Profession & Interactive Lecture/Group Discussion/Role Playing /Ego Reflective Exercise & Research 1 hrs/week 1st & 2nd Education) A BRIEF HISTORICAL OVERVIEW 3rd & 4th 5th & 6th PROBING EDUCATIONHEALTHQNHEPC\LIFE” = DEFINE THE COMMON THEORIES & MODELS OF NHEPC (1) = TERMS & Relations: HEALTH, HEALTH EDUCATION, TEACHING & LEARNING….etc - THE COMMON THEORIES & MODELS OF NHEPC (2) 1st EXAM + Assignments Plan = Smart Exam1 7th & 8th - NHEPC Related COMMUNICATION; COUNSELING & ETHICS = 9th & 10th NHEPC METHODOLOGYIES & TECHNOLOGIES (1) = 11th & 12th NHEPC METHODOLOGYIES & TECHNOLOGIES (2) QNHEPC PLANING TERMS & PROCESS (1) = Smart Exam2 2nd EXAM + Assignment Presentation 13th & 14th 15th & 16th - QNHEPC PLANING CONCEPTS & PROCESS (2) - NHEPC FIELDS \ ASSOCIATIONS & RESOURCES Final Revision + FINAL EXAM = = ASSESSMENT: 2 Monthly Creative Exams + Reflective Assignment (15 Grades each) CHS456 Johali2012 7 The Most Recommended Reference & Source *** Your Smart Lecture Notes, in the Class **Johali, E A (2012) A Concise Nutrition Health Education For Smart Clinical Nutritionists and Dietitians : A Creative Lecturer’s Note (Soon be ready may be Quwafel Centre, King Abdullah Road, near KSU ) Johali, E. A (2012) Health Education and Promotion for All Health Professions the HEPAHP (A Project Book in Press, Damascus) * Johali, E. A (2010\2011) Health Education and promotion for Health Administration and Technicians HEHAT (Qwafel Students Center , King Abedalah Rd from of KSU) JOHALI (2008) A Concise Health Professions History and Ethics, Dar Aawael Damascus; Syria (Specials discount for you SR 35 Al Quwafel Centre, King Abdullah Road, near KSU) CHS456 Internet Resources http://www.dairycouncilofca.org/PDFs/AppToolkitFacGuide.pdf Johali2012 8 NHEPC Reasoning ? نعود لها الحقا REASONING WHY NHEPC? Let us Start with: How to Train to Be a Nutritionist http://www.ehow.com/video_5611014_train-nutritionist.html What is a Dietitian? http://www.ehow.com/video_4979770_what-dietitian.html Dietitians vs. Nutritionists http://www.ehow.com/video_4767643_dietitians-vs_-nutritionists.htm Nutritionist Job Description http://www.ehow.com/video_4958429_nutritionist-job-description.htm http://www.ehow.com/video_7462937_hints-reading-food-nutrition-labels.html CHS456 Johali2012 9 JOHALI CONCISE NHEPC REASONING NHEPC WHY? - CHS 456 Despite that this place is questionable worldwide may be because there are HE Specialists; Nationally, there no wide concern regarding HE specialty and specialists, thus it is a part of the nature of all HPs as it is stated in the HE Guide (MOH 1398) Group Discussion & Dialogue The Place of HE in CN the CNJD? The Place of HE in CNE related courses? ===== • • Play a role of CN working in hospital … Do you have to practice NHEPC (protect, prevent, promote healthful life of you, your colleague & your patients, families and community?) Then, Play a role of CN Student what is/are the most related CN Courses/ Sciences can be use in HEPC ? To conclude; The Major Reason WHY HEPT?, because “HE is a part of CN Professional Duties CJND”; To: - Protect; - Prevent and; - Control; - Maintain, and Promote Quality of Healthful Life for your, your colleagues, your patients and environment ..from Nutrition\Food Hazards, Poising , Imbalance & Overeating\ Habits and related Health Problems.. CHS456 Johali2012 10 The CNJD دور أخصائي التغذية اإلكلينيكية : •التعاون مع أعضاء الفريق الصحي الخاص برعاية المريض من خالل تقديم الرعاية الغذائية. هناك عدة أسباب تسهم في إقصاء أخصائي التغذية عن ممارسة دوره .نذكر منها : رضىعدم وضوح الوصف الوظيفي -فالكثير من أخصائيي التغذية ال يعرفون ما هو مطلوب منهم ،و الكثير من •التوعية الغذائية للوقاية من بعض األمراض للمجتمع وكذلك الم )1 ن ن أخصائيي التغذية تفاجئو حين توظيفهم حيث يرو أن ما تم دراسته في الكليات المتخصصة قد بقي محفوظاً في على حد سواء. الكتب !!و كمثال على هذا فقد سأل أحد األخصائيين ممن توظف حديثاً في المستشفى أحد زمالئه عن دوره وما •وضع البرامج التدريبية واالستشارات وكذلك إعداد الوسائل يمكن له أن يقوم به من أعمال ،فما كان من زميله إال أن قال له :إن أهم عمل تقوم به هو أن تراقب خط سير التعليمية في مجال التغذية للعاملين في مجال الصحة العامة مثل توزيع الوجبات !! الممرضات والعاملين بالوقاية الصحية. )2كثرة المهام و المسؤوليات -تسعى بعض اإلدارات إلى أن ترسم وصفاً وظيفياً لموظفيها ،حيث تقوم بتكليف •وقاية المرضى المنومين من اإلصابة بسوء التغذية الناتجة عن األخصائي عدة أعمال ،و تضع في نهاية هذه المهام فقرة تقول ( أي مهام أخرى تسند إليه )!!و إذا بنا نرى أخصائي التغذية يكون مسؤوالً عن أعمال الشركة ،أعمال إدارية ،أعمال السكرتارية ،متابعة أعمال أخرى نقص الطاقة والبروتين. كضيوف اإلدارة !! •المساعدة على عالج الحاالت المرضية واختيار األغذية المناسبة )3ضعف الثقة -وهي على أربع أنواع :ثقة األخصائي بقدراته .ثقة إدارة التغذية بقدرات األخصائي .ثقة إدارة لها. المستشفى بقدرات األخصائي.ثقة األطباء بقدرات األخصائي.و كمثال على ضعف الثقة نرى بعض األخصائيين •تحديد طبيعة وكمية العناصر الغذائية الالزمة للمريض ومدى يخشى من التحدث مع األطباء ،الممرضة ،أو المريض نفسه. احتياج المريض لألغذية التكميلية (التغذية األنبوبية أو الوريدية) ).4قلة الخبرة -يفتقر بعض األخصائيين للخبرة الكافية في مجال تغذية المرضى . •التحكم بوزن المريض زيادة أو نقصا. )5عدم الرغبة في تحمل المسؤولية -بعض األخصائيين ليس لديه رغبة في أن يتحمل مسؤولية متابعة حالة أحد المرضى ،أو ليس لديه الرغبة في أن توكل له بعض المسؤوليات ،و بعضهم يكتفي بالمسؤوليات التي ال تحمل •متابعة المرضى المنومين من خالل إرشادهم بطبيعة النظام الغذائي ائها أية متاعب !! الواجب إتباعه والتحقق من مدى إقبالهم على الوجبات المقدمة لور هم. مهام أخصائي التغذية ...من النظرية إلى التطبيق •المشاركة في البحوث العلمية . ألخصائي التغذية الدور الحيوي و الهام في المستشفيات ،و ال يمكن إغفال دوره بأي حال من األحوال، •اإلشراف على عيادات التغذية الخارجية كعيادة السمنة والسكري أو و يمكن أن تتمثل مهام أخصائي التغذية في اآلتي: األطفال. أوالً :األستشارة الغذائية و هي أن يكون األخصائي على اتصال دائم بالطبيب المعالج ،و يشارك في االستشارة 11 الغذائية. ثانياً :التقييم الغذائي أهميته : ) 1من خالل التقييم الغذائي يمكن معرفة الحالة الغذائية بالنسبة للشخص السليم و المريض على حد سواء . ) 2من خالل التقييم الغذائي يمكن عمل برنامج غذائي يتماشى مع احتياجات الشخص لتصحيح الحالة الغذائية . Johali2012اإلرشادات الغذائية . ) 3تقديم النصائح و CHS456 Probe HISTORY & DEFINE TERMS Looking for The E ; H & CN that can Assure the Quality of Healthfully Life ? CHS456 Johali2012 12 PROBE NHEPC HISTORY & DEFINE TERMS Place of Health & HE in the Holy Quran & Prophet Medicine ? (Ego Reflective Assignment) Worldwide, the literature of both health and education neglected health education and its facts including the Islamic concepts until the early of this century. It was only in the late 1919 that the term “Health Education” was recognized in the Western literature by: The term “Health Education” was proposed first about 1919 at a conference in New York of leaders of health and education called the Child Health Organization. The word “Hygiene” has become some popular in schools with both teachers and pupils that it was believed a new and more definitive term would be helpful in popularizing health practice. “Health Education” as a term to replace “Hygiene” was advanced by the director of the organization and after much discussion adopted. (Kime et al 1977) CHS456 Johali2012 13 PROBE HE HISTORY & DEFINE TERMS “Nature & History Proper Definition” The above historical statement clarify the nature of modern HE. It indicates that Hygiene (Germ-free, Pure, and Healthful) was the previous term of health education in the Western literature. It confirms the Integrated Relationship between the three Sciences “Education; Health & NHEPC” and their Professions” that can simplified by the following formula: EDUCATION HEALTH QNHEPC\LIFE SO, What is the “EDUCATION” that leads to HEALTH?" & Go ahead to promote the Quality of NHEPC? CHS456 Johali2012 14 Probe HE History & Define Terms -Nature & History Proper Definition” What is the “EDUCATION? that we are looking for ? How did the Old Greece and Muslims Philosophers and Scientists educate (Socrates; Aristotle; Plato & Ibn Khaldon, Al Ghazali; Avicenna & Bin Bazz?) (Ego Reflective Assignment) The term “Education” came from: the Latin words “Educo = To lead out” the & "Educare = Training the mind; the English term "Educe = To draw out". In Islam and Arabic language “Education” means: Breeding & Perfection; reform وإصالح، تهذيب،تربية End 1-2nd week The latest ًWestern educational philosophies such as “the progressivism & the reconstructionism” connect "Education" to the “Freedom = the Democracy”. In the late 17 Century, "Rousseau" a French teacher addressed the following advice: Give your scholar no verbal lessons, he should be taught by experience alone...Put the problems before him and let him solve them himself. Let him know nothing because you have told him, but because he has learnt it for himself. Let him not be taught science, let him discover it. (Johali 1995). CHS456 Johali2012 15 PROBE HE HISTORY & DEFINE TERMS What is the “EDUCATION? That we are looking for ? Also, Albert Einstein" (1878-1955) the German/US Physicist said: "I never teach my pupils; I only attempt to provide the condition in which they can Learn“ (Valcin 2001) These advices formed the foundation of the progressive, freedom or democratic education that produced many modern educational theories and strategies such as: Problem-Solving & Problem Based Learning; Learning by Experience or Experiential Learning ; Learning by Discovery, and finally, "Andragogy” the"Student/Patient Centred Leaning. Eventhough, the Western Philosophers still looking the education that assure the quality.. CHS456 Johali2012 16 PROBE HE HISTORY & DEFINE TERMS What is the “EDUCATION? that we are looking for ? The Optimists (Idealists) of the above philosophies and theories believe in the “Ideal Education” that “: A Perfect Education will Produce a Perfect Society or Heaven on the Earth” As A Muslim; Do you believe ? (If you don’t?!, Your Religion Do) This believe was strongly criticized by many educational philosophies such as, the Realism who reject the terms “perfect or idealist”; the Behaviorism who see “education in their behaviors” and, the Experientialism who connects “education to the experience only”. Reflecting on the above educational concepts with health considerations, the logical definition of “General Education” can be concluded as: “A Lifelong Process ofJohali2012 Growth and Development” CHS456 17 PROBE HE HISTORY & DEFINE TERMS What is the “EDUCATION? That we are looking for ? Self thinking “EGO QUESTION: Modify the above definition of “general education” into an Islamic definition?” ==== “A Growth and Development Process for …….. & the …… …. ” The Ideal Islamic Definition of “GE” is A Growth and Development Process TODAY & for the DAY AFTER OR A Process of Meaningful Learning for Today & the Day After The appropriate “Education” تثقيف/ تعليمthat can be defined as: An intellectual & behavioral process of “Teaching and Learning” activities that influence the growth & development and promote healthful life. Still, “What Teaching &تدريسWhat is Learning ” تعلمthat can promote the QHEHِ? CHS456 Johali2012 18 PROBE HE HISTORY & DEFINE TERMS “Nature & History Proper Definition” What is the “EDUCATION? That we are looking for ? While the traditional “Teaching” is understood as: “A teacher based process of providing and injecting knowledge, attitudes and skills” to inflate memory. The “TEACHING” that we are looking is “a process of promoting and helping other to LEARN. The traditional behaviorism “Learning” is realized as “a process of gaining deep and wide knowledge, attitudes and skills that can control and shape behaviors. Such learning is a form of training rather than education. While, The Millennium “LEARNING” that we are looking for is: “An Independent Process of Growth and Development within the personal science, technology, experience, & behavior CHS456 Johali2012 19 Common Philosophies (Systems) of Education Just look for the Place of Education that we are looking for? Key Concepts Most Common Philosophies & Theories of Education Humanism Transfer Education /NHEPC Process Preserve& Transmit Knowledge Knowledge/ Theory worthwhile Skills/ Practice Relative to safe practice Teacher/HE/CN Centre / Transferor Examination/ Evaluation Vital-theory Student/Patient Passivecontainer Fully-controlled Curriculum/Plan Map of key Subject CHS456 Technocrat Shape Progressivism Travel /Jearny Reconstructionis. Grow Adaptation/ Training Training/Skills/Objec tives relative- essential for safe practice Personal Growth & Development Society-Centered Create better society Life experience Tentative Student interest Life experience Tentative Society interest Vital Vital Vital Instructor & Guide Facilitator Indoctrinator/ Orientator Vital- practical Self interest & evaluation Vital theory-practice for better society Passive- holder Active/ Free-interest practically fully supervised Schedule of Basic Skills/ a kind of Technology Johali2012 Portfolio of Experiences Active Semi-control Agenda of Cultural Issues 20 PROBE HE HISTORY & DEFINE TERMS “Nature & History Proper Definition of HEALTH” WHAT IS HEALTH? that we are look for:? Medics “Curative Medicine” Physical fitness absence of disease harmonious functioning of organs Commodity “Just Feeling Good” Behaviorists ability adapt to “Adaptation” (HBM) Social Scientists Humanists Well social Personal strength\ability function absent of all Self Growth & diseases, Development health problems handicaps & Idealists Perfect wellbeing in every respect Behaviorist also come under Realism = Pragmatic So; What is National Health; Nat & Nut. HE That We Have To Look For ?! CHS456 Johali2012 21 A CONCISE NHEPC “Nature & History Proper Definition of HEALTH” that we looking for? To be appropriate for all nation; the “WHO Constitution 1946”, “Health” is defined as: A STATE OF COMPLETE PHYSICAL, MENTAL AND SOCIAL WELLBEING AND NOT MERELY THE ABSENCE OF DISEASE AND INFIRMITY. --------------- Infirmity = any health problem or defect Complete = Total; Whole; Absolute & Perfect ----------------------Ego Reflective Thinking & Assignment As an ideal religious centred society, how we can create an accepted “Health” Definition with Evidences from Holy Quran & Sunnah ”? ------------------------ Now, start think about Defining HE & HEPT that can grantee the Quality of healthful Life CHS456 Johali2012 22 A CONCISE NHEPC “Nature & History Proper Definition that we looking for WHAT IS HEALTH EDUCATION? As health + education, “HEALTH EDUCATION” has different meanings. Based on the scientific principles of the “Learning and Behavioral Theories & Models” and “the Diagnostic Approach of Planning H. E.”, the most appropriate definition can be a combination of these two definitions: WHO” DEFINITION A PROCESS WITH INTELLECTUAL, PSYCHOLOGICAL, & SOCIAL DIMENSIONS RELATING TO ACTIVITIES THAT INCREASE THE ABILITIES OF PEOPLE TO MAKE INFORMED DECISIONS AFFECTING THEIR PERSONAL, FAMILY AND COMMUNITY WELL-BEING. & BEHAVIORIST DEFINITION ANY COMBINATION OF LEARNING EXPERIENCES DESIGNED TO FACILITATE VOLUNTARY ADAPTATIONS OF BEHAVIOR CONDUCTIVE TO HEALTH. ------------------------- Ego Exercise: So, as an ideal modern religious centred society, how we can create NHEPC Overall Goal CHS456 Johali2012 - An ideal “accepted & promoting “NHEPC Definition”? - Persuasive NHEPC objectives (Drive from WHO & Behaviorist Def) 23 A CONCISE NHEPC “Nature & History Proper Definition of H; E; HEP & NHEPC we have to looking for ? Thus, let us hold a “Learning Debate” Based on these literature, the nature of the Saudi community and culture, the nature and fortitude future of HE, the ideal definition of a “National Health; & National NHEPC that the whole people can understand, accept and react with it positively, is: CHS456 Johali2012 24 A CONCISE NHEPC “Nature & History Proper Definition of NHEPC Objectives H E QUALITY OF HEALTHFUL LIFE HEHA/HEHAT QUALITY OF HEHAT PATIENTS’ & EMPLOYEES’ HEALTHFUL LIFE & THE TWO MAJOR HE OBJECTIVES ARE HELP PEOPLE TO INCREASE THIER ABILITIES TO MAKE INFORMED DECISIONS AFFECTING THIER PERSONAL, FAMILY AND COMMUNITY WELLBEING. FACILITATE VOLUNTARY ADAPTATIONS OF BEHAVIOR CONDUCTIVE TO HEALTH. BY ENCOURAGING, MOTIVATING, PROMOTE ........NOT TEACH/INSTRUCT\ORDER PEOPLE\PATIENTS TO: ACQUIRE .………………………………...…,. PERCEPT (Accept/ not Reject) .…....... MOTIVATE To (accept) ……….………….. MODIFY\HELP CHANGE voluntary ..........…… & CHS456 Johali2012 PROMOTE SELF / INDEPENDENT / MAINTAIN HEALTH BEHAVIORS 25 A CONCISE NHEPC “Nature & History Proper Definition of A National H; E: P & NHEPC A NATIONAL DEFINITION OF HEALTH; HEP & NHEPC The history of health, education and health education show that health education has many definitions and understanding. These definitions and understanding are varied from generation to other and from nation to nation according to their cultural and social background. To motivate people to accept and react positively with health education message and activities, the early and the religious based definitions were considering the terms "Moral; Spiritual & Emotional"... As an outcome of the Western Age of Reasoning, these morality terms were neglected. At the early of 20 century, there were worldwide debates regarding the most appropriate definitions for health, education, and health education. As a result of these philosophical and scientific debates, the early terms and many other such as “physical and / or intellectual, mental and / or psychological, cultural/environmental and or social….” were discussed for the best health education definition. Beside "Politics" the administrator factor, there are many other factors such as "economical, scientific and technological" factors such as poverty, hunger, hazards that can affect the quality of health full life of people (-ve/+ve). CHS456 Ego (self) Reflective Learning: Johali2012 26 A CONCISE NHEPC “Nature & History Proper Definition of A National H E & NHEPC An Ideal dynamic process of (1) Moral, (2) Spiritual, (3) Physical, (4) Intellectual, (5) Mental, (6) Emotional (7) Psychological, (8) Social, (9) Cultural, (10) Environmental, (11) Economical, with (12) Professional Ethics, that can help people/customers to “grow; develop”, and make informal decisions affecting their personal, family and community well being. “An outcome of NUR/MLT Student Group Work 21/2/1427” An Ideal dynamic process of “(1) Moral, (2) Spiritual, (3) Physical, (4) Intellectual, (5) Mental, (6) Emotional (7) Psychological, (8) Social, (9) Cultural, (10) Environmental including Climate, (11) Economical, (12) Political with (13) professional Ethics, (14) Technological mean and (15) Nutritional” dimensions that can help people/customers to “grow; develop”, and make informal decisions within a specific “Time” affecting their personal, family and community well being. “An outcome of “Has’ Student-Lecturer Dialogue HEHA 28/2/1427”modified 1428 ; and NHEPC 2012” Where Are You ? ; Do you have any addition .. New dimension / factor can affect your health … ?! 27 CHS456 Johali2012 Conclude ?! CHS456 Johali2012 28 Health Promotion the New, the Fashionable the Millennium Name CHS456 Johali2012 29 Health Promotion the Fashionable Millennium ‘New’ Name Definition of Health Promotion Health Promotion is the art and science of helping people discover the synergies (independent discovering) between their core passions and optimal health, enhancing their motivation to strive for optimal health, and supporting them in changing their lifestyle to move toward a state of optimal health. Optimal health is a dynamic balance of physical, emotional, social, spiritual, intellectual health, ….. more... !! Lifestyle change can be facilitated through a combination of learning experiences that enhance awareness, increase motivation, and build skills and, most important, through the creation of opportunities that open access to environments that make positive health practices the easiest choice. Meanwhile; O’Donnell MP. Defined HP as a process of ‘embracing passion, enhancing motivation, recognizing dynamic balance, and creating opportunities’. Am J Health Promot. 2009 Sept Oct;24(1):iv. 30 CHS456 Johali2012 Physical: Fitness; Nutrition; Medical self-care; Control of substance abuse. HP Def. Model: Emotional: Care for emotional crisis. Stress Management Social: Communities. Families. Friends Intellectual : Educational; Achievement; Career development Spiritual : Love; Hope; Charity…. (It is more…..see “Johali 2010 SARMR San Antonio, Texas, US, Jjohali Res. Sites ) http://www.healthpromotionjournal.com/index.html Compare to the above concepts …Is\ Are there missing …factor\dimen. !!? CHS456 With your meta thinking discover & Innovate New DefHPM ?! Johali2012 31 WHO Health Promotion Principles Health promotion initiatives should be planned and implemented in accordance with the following principles: 1. Empowering: Health promotion initiatives should enable individuals and communities to assume more power over the personal, socioeconomic and environmental factors that affect their health. 2. Multi-strategy: Health promotion initiatives should use a variety of approaches, including policy development, organizational change, community development, legislation, advocacy, education and communication, in combination with one another. 3. Participatory: Health promotion initiatives should involve those concerned in all stages of planning, implementation and evaluation. 4. Holistic: Health promotion initiatives should foster physical, mental, social and spiritual health. 5. Inter-sectoral: Health promotion initiatives should involve the collaboration of agencies from relevant sectors 6. Equitable: Health promotion initiatives should be guided by a concern for equity and social justice. 7. Sustainable: Health promotion initiatives should bring about changes that individuals and communities can maintain once initial funding has ended. 8. CHS456 In addition to Advocacy: activities directed at changing policy of32 Johali2012 organizations or governments. HP Optimal Wellness Model Reflect on the previous probing and national definition & Redraw it as Optimal NHEPC Wellness Model , later compare to APCHER NHEPC 33 CHS456 Johali2012 PATIENT \ NUTRITION COUNSELING Counseling ( Resources: 2 | Journals: 3 | Organizations: CHS456 Johali2012 34 COUNSELING Nutrition \ Patient Counseling What Is Counseling; NP Counseling Coun·sel (kounsl) “ N 1. The act of exchanging opinions and ideas; consultation. 2. Guidance, especially as solicited from a knowledgeable person. See Synonyms at advice. 3. A plan of action. 4. Private, guarded thoughts or opinions: keep one's own counsel. 5. A lawyer or group of lawyers giving legal advice and especially conducting a case in court. V coun·seled or coun·selled, coun·sel·ing or coun·sel·ling, coun·sels: 1. To give counsel to; advise. See Synonyms at advise. 2. To recommend: counseled care in the forthcoming negotiation It can be also, a “Road map”: a detailed plan or explanation to guide you CHS456 in setting standards or determining a course of action; 35 NUTRITION COUNSELING Nutrition counseling is an ongoing process in which a health professional, usually a registered dietitian, works with an individual to assess his or her usual dietary intake and identify areas where change is needed. The nutrition counselor provides information, educational materials, support, and follow-up to help the individual make and maintain the needed dietary changes. In NURSING INTERVENTIONS CLASSIFICATION; Nutritional counseling defined as the use of an interactive helping process focusing on the need for diet modification CHS456 (later applied case studies if there is a time) Johali2012 36 NHEPC The Applied Sciences The Most Related Theories & Models Do you belief in science ?, are all sciences can applied ?; why ? This learning unit helps you to realize the most appropriate Philosophical & Scientific Concepts. REMEMBER, during planning, you have to practice every thing, all the sciences that you have learn. CHS456 Johali2012 37 PERSONALITY (Self) DEVELOPMENTAL THEORIES (PDT) Personality Theory of Development CHS456 Johali2012 38 PDT: A Creative Integrated Global Model Personality Environment Heredity Physiological Process (Repro & Growth) SocioCultural Genetic DNA Physical Attributes Socialization SELF Determine Development Concept Experiential Identity – Esteem – Effectiveness Learning Worth – Copy – Express – Aware – Autonomy CHS456 Johali2012 Response – Behave – Attitude - Belief – Value – Actualization 39 PDT: What is Personality Essential for Johali HEHAP Communication, there is no QC; QHEHAP without PDT) A Person and Personality are the centre of human communications and health education. Therefore, it is important to understand these terms before studying the personality development theories. * A Person is a human being considered as having a character of his or her own. * Personality is the whole nature or character of a particular person or individual. It is the dynamic organization within the individual of those psychological systems that determine his/her characteristic behavior and thought. “By Critical thinking, you can estimate a simple Definition from IM” In our Integrative modified Model (IM); ** PERSONALITY is a dynamic process of three basic forces “Heredity, Environment CHS456 Johali2012 and Self. 40 PDT PDT is the base and the master theory that builds and shapes the whole personal characteristics. Heredity shapes the physiological development process of the fetus from conception to birth and, the “Chromosomes” which made up of Deoxyribo-Nucleic Acids (DNA) carries the genes that determine the personal physical attributes. Environment consists of many surrounding geographical, cultural and social forces that are originated outside the individual and shaping his/her personality development including the “Religion”. Socialization is a state of living with others in successful manner, social process starts immediately after the birth. Culture is the vital force which shapes and control our live, all people are molded by the particular culture in which they reside. Culture in the Western literature means religions, beliefs, ethics, norms, traditions, values, attitudes, thoughts, learning or education, actions and the wisdom of the people. These and other cultural forces are preserved, transmitted and developed from generation to generation by the process of socialization and every society has its culture or social system **In Saudi Arabia…, personality and its developmental process shaped by Islamic Principles. CHS456 Johali2012 41 SELF THEORIES SELF is the whole being of a person who has specific nature, character and ability or the structure of the personality. The term “SELF” denotes how individuals perceive or understand and accept themselves in terms of identity, worth, esteem, and effectiveness - In terms of realistic, knowing, doing, achieving, and being. It denotes how they experience events and interpret them either to reinforce or alter earlier perceptions; how they develop consistency and continuity of purpose; and whether they see their own selfhood as unique (Ross & Mico, 1980, 36). Many psychologists and sociologists holds the fact that the person who has healthy reproduction and growth, genetic and environment patterns will have healthy characters (behavior and thought) or healthy personality. CHS456 Johali2012 42 Self-Concept of Learning Self-concept is defined as an organization self images perceived through the appraisals or feedback of others by which the individual develops a concept of adequacy or effectiveness. The observed self and adequate self together make up the self-concept, it is a process of “how to behave in order to be effective”. Due to the fact that experience is an early stage of personality development, Beatty identifies four areas of organizing experience and learning with other related HE becomes Fix areas (5S): Self Worth: By experiencing love or other inclusion, to gain a sense of self-worth without an accompanying sense of defensiveness. Self Copying: by learning how to do something that previously could not be done, to feel more able to cope effectively. Self Expressing: by means of affective (pleasant or unpleasant), by experiencing sensations, to become more self-expressive and relatively free of tension and anxiety. Self Awareness: Be aware and perceptive Self Autonomy: making autonomous choices, to develop a greater range of choices. CHS456 Johali2012 43 Self-Determinism - Development theories Self-determinism is based on believe that “human beings are unique in their individual: - Responses; - Behaviors; - Attitudes and; - Values; These concepts are potentially the Selfactualizing . Both self theory of learning & self theory of determinism integrate many theories such as experience and learning (Beatty), personality development (e.g; Coleman's Model), perception and motivation (e.g; Maslow’s Hierarchy of Needs & H B Model). CHS456 Johali2012 44 MASLOW HIERACRCHY (Ladder) BASIC HUMAN NEEDS CHS456 Johali2012 45 COLEMAN P DEVELOPMENT STAGES (CDS) Comparative Summary CDS/ Maslow 6 Later Age 60+ Retirement/ new live 5 Middle Age 36-60 Full Responsible self realization 4 Early Adulthood 18-35 Be Responsible self estimation 3 Adolescence 12-18 Identity/Ego 2 Middle C 6-12 Social needslearning 1 Early Child hood 0-6 Basic needs Learn to Live social safety physiological Ego Ref Qs: - Why Maslow with Coleman ?; Why M & C for HEHAP ? -Learn to live is essential at late age ( T / F) correct - Self esteem/Ego raised at adolescence ( T/F) correct if F CHS456 Johali2012 46 PSYCHO-LEARNING THEORIES PERCEPTION & MOTIVATION THEORIES CHS456 Johali2012 47 PERCEPTION THEORY The base of Human Behavioral Model (HBM) & Assertive HEPT Perception (Awareness) is a mental and psychological process. It is a dynamic process of thinking - learning and, memorizing (learn by heart). It is the common “Five Human Senses". It denotes how things “Look; Sound; out side Feel; smell and Taste. It explains “why individual perceived "accept or reject" HEPT Messages. It is the first and the most important element of HEPT Process. If you welling to achieve the quality, you have to use the “ATAPE (5) Stages Plan” (Tindall1994,34): Anticipate different perceptions (Mainly: Persons/individuals; Message & Share dif. Perceptions”. Try to be aware Ask for feedback from receiver the patients Provide feedback to the sender the health educator Evaluate level of perception CHS456 Johali2012 48 MOTIVATION THEORY Traditionally, Motivation is a process of encouraging perception towards a positive health behavior. There are six sub- theories of motivation: Reinforces -Needs -Cognitive dissonance or conflict -Attribution (why) - Personality affiliation or achievement & Expectancy. Generally, this theory comes after perception to initiate, direct, maintain and promote behavior to fulfill ‘Basic Needs’. Today & in this course, we hope to use “Perception & Motivate” to “initiate and promote our self & Patients to move toward the Optimum Quality of HEMLT Optimum Quality of Healthful Life. CHS456 Johali2012 49 MOTIVATION THEORY Motivation takes two major forms: 1) Drives: motivators: the Internal / physical PRIMARY Drives e,g; hunger-eating, thirstdrinking. LEARNED Behaviors (desire-smoking) which become functionally autonomous through repetition and reinforcement. 2) Incentives: the External motivators: Facilitative, to satisfy needs and realize potentials Coercive/persuasive, to impose behaviors strange to person’s needs or potentials. CHS456 Johali2012 50 P&M THE GENERAL TWO PRINCIPLES READINESS: Learning is Most Effective when a Learner is Ready and Welling to learn. (Are you?) INCENTIVE LEARNING ENVIRONMENT & PROCESSES: Good place and atmosphere, effective teacher and teaching lead to cooperative and effective learner and outcomes. CHS456 Johali2012 51 THEORY OF BEHAVIORAL EDUCATIONAL OBJECTIVES Learn to behave BLOOM s’ TAXONOMY OF LEARNING OBJECTIVES the Domains Simple / Dependent / Passive COGNITIVE Know – Knowledge AFFECTIVE Think – Value – Response - Judge PSYCHOMOTOR/ACTION Intellectual Skills Behaviors (Doing): Reflect – Adapt - Modify - Decide – Move Complex CHS456 / Independent Johali2012 / Active 52 THEORY OF BEHAVIORAL EDUCATIONAL OBJECTIVESLearn to behave The BLOOM s’ TAXONOMY OF LEARNING OBJECTIVES Domains Verbs Simple Class / Dependent Area / Behavioral Objective Cognitive Knowledge Knowledge Int. Ability Reflect/Move Reason Respond Communicate Plan to solve Value/apprise Act Format Organize/character Adapt Understand Create/Interpret Develop Inter Judge Ext Judge Decide Int. Skills Evaluation Complex CHS456 / Action/ Psycho Receive Analysis Synthesis Affect Remember Comprehension Application Passive Independent / Active Johali2012 / Deep understanding 53 HBM CHS456 Johali2012 54 Health Belief Model (HBM) Because, HBM bases on the concepts of “perception, motivation, Behavioral objectives theories as well experiential learning theories”. Thus, HBM can be considered as “an integrated and interactive health learning model”. HBM is a paradigm used to predict and explain health behavior based on value-expectancy theory. It affirms that individuals are not likely to take a health action unless they are: Well Motivated Learns = Who have (Background) + (Perceptions-Threat & Expectations) + (+ve Behave) The HBM was first developed in the 1950s by social psychologists Godfrey Hochbaum, Irwin Rosenstock, and Stephen Kegels working in the U.S. Public Health Services. The model was developed in response to the failure of a free tuberculosis (TB) health screening program. --------------------------RQs HBM is Health, . . . . . . Model, it is a . . . . . . . . Used to . . . . . . . Explain health . . . . . . . . Based on . . . . . – expectancy CHS456 Johali2012 55 HBM the Modified Model the Schematic Diagram Background + Socio Demographics Factors Age; Edu status; gender… Perception + Action Threat Cues • P Susceptibility • P Severity Media Influence Reminder + Expectations Behavior to Reduce T based on E P Benefits P Barriers + S efficacy CHS456 Johali2012 56 HBM the Model HBM = Background + Perception - Action Perception = Threat - Expectation Expectation = Benefits + Barriers + S efficacy HBM outcome = +ve Behavior by Reduce T based on E Draw ………….. CHS456 Johali2012 just see ( ( ( ( ) ) ) ) 57 •Define & Apply HBM Concepts Concept 1. Perceived Susceptibility Definition One's belief of the chances of getting a condition Application Define population(s) at risk and their risk levels Personalize risk based on a person's traits or behaviors Heighten perceived susceptibility if too low 2. Perceived Severity One's belief of how serious a condition and its consequences are 3. Perceived Benefits One's belief in the efficacy of the advised action to reduce risk or seriousness of impact Define action to take — how, where, when Clarify the positive effects to expected Describe evidence of effectiveness 4. Perceived Barriers One's belief in the tangible and psychological costs of the advised behavior 5. Cues to Action Strategies to activate "readiness" 6. Self-Efficacy CHS456 Confidence in one's ability to take action Specify and describe consequences of the risk and the condition Identify and reduce barriers through reassurance, incentives, and assistance Provide how-to information Promote awareness Provide reminders Provide training, guidance, and positive reinforcement Johali2012 58 HBM Predict & explain Sick Role & Predict Preventive H Behavior CHS456 Johali2012 59 NHEPC Related ETHICS & COMMUNICATION Bases Can Facilitate Quality of Plan NHEPC CHS456 Johali2012 60 ETHICS THE MOAJOE ISLAMIC ETHICAL BASES ISLAMIC ESSENTIALS Individual/Personal Nature & Educational Development: from fetus - later age & day after التربية والتطور الطبيعي للفرد Social Security/Welfare & Relationships التكافل واألمن والعالقات االجتماعية COMMUNICATION RIGHTS حقوق التعامل والتواصل (As a Muslim learner; You have to write Evidence from Holly Qura’an & Sunnah) CHS456 Johali2012 61 THE MOAJOE ISLAMIC ETHICAL BASES ISLAMIC FOUNDATIONS HUMAN NOBILITY / Dignity - Identify اإلنسانية الكرامة JUSTICE & EQUITY واملساواة العدالة HUMAN COOPERATION التعارف والتعاون اإلنساني FORGIVENESS/COMPASSION/AFFECTION / التسامح الرحمة واملودة HONESTY / FIDELITY/Loyalty اإلخالص BENEFIT/ USEFULNESS املنفعة واملصلحة/البر/اإلحسان CHS456 Johali2012 الوالء/ /األمانة 62 THE MOAJOR ISLAMIC ETHICAL BASES GLOBAL MORAL REASONING THREE MAJOR LEVELS + 6 STAGES PRE-CONVENTIONAL LEVEL STAGE 1: Moral Realism STAGE 2: Individual & Instrumental Morality CONVENTIONAL LEVEL STAGE 3: Interpersonal Normative Morality STAGE 4: Social System Morality POST-CONVENTIONAL LEVEL STAGE 5: Human Rights & Social Contract Morality STAGE 6: Universal Ethical Principles (because People seen as having value in themselves rather than as agent of social values, thus it emphasis the “Self chosen for best Justice; Human dignity & Rights → Optimum Quality CHS456 Johali2012 63 THE MOAJOE ISLAMIC ETHICAL BASES GLOBAL ETHICS PRINCIPLES BENEFIENCE : Act in the best interest of the patient, it is a moral (religious) principles, the Western traced to Hippocratic pledge. Meanwhile, it is one of the major Islamic Principles. AUTONOMY: Patients rights to self-determination; to chose what will be done to them. HONESITY : Patients have the right to the truth about their medical conditions, the course of their disease, the treatments recommended & alternative treatment available. INFORMAL CONSENT : this is a part of Autonomy & honesty principles. The patients have the right to be informed about all the relevant medical aspects including the treatment. CONFIDENIALITY : based on the human dignity, patients have the right to assure that all the information about their medical conditions & treatment will not be given to other without their prior permission. FIDELITY/LOYALTY: Your responsibilities should be directed toward the “Patients Welfare”, not to the physician interests CHS456 Johali2012 64 THE MOAJOE ISLAMIC ETHICAL BASES THE ETHICAL SEVEN SEAS (7C’s) 1st Step towards QUALITY NHEPC COMMUNICTION 1. Credibility: You the source “the Sender (S)” must be competent and reliable to Motivate 2. 3. 4. 5. Context: HE Message (HEM) must be relevant to the receiver Content: HEM must have genuine meaning “meaningfulness” Clarity: the R “Patient” must be able to understand the message Continuity: Though repeated with variations, HE Message must be consistent (steady reliable) enough NOT to Confuse the R 6. Channels: HEM must use the most acceptable communication channels\media (HE methodology & technology) to the R 7. Capability: The R must be able to communicate effectively with Least amount of Effort CHS456 Johali2012 65 NHEPC related HUMAN COMMUNICATION CHS456 Johali2012 66 Related HE COMMUNICATION THEORIES & SKILLS Interaction Theory Interaction is the act of having an effect on each other. Thus, it is a process of exchange = communication. It is based on a consideration of three main elements: - Activity, refers to the act or behaviors that the group undertakes - Interaction, pertains to the reaction or the exchange that occur among group members. - Sentiment or Attitude, to the feelings members have their communicating or working to gather. CHS456 Johali2012 67 Related HE COMMUNICATION THEORIES & SKILLS Attitude Change Theory In order to produce effective HE communication: and to change attitude, this theory gives Three main conditions: 1. 2. 3. The Nature of communication: eg. Sender characters The Validity of communication source: e,g; Massage. The Characteristics of the audience the receiver. It is based upon the foundations: The Greater the Prestige and Credibility of communication & HE process, the Greater Effectiveness “quality” and Attitude Change’. The Greater the Fear aroused by HE Message, the Less likely were the Patients to Accept it. CHS456 Johali2012 68 Related HE COMMUNICATION THEORIES & SKILLS Types & Skills of Human Communication Non Verbal Symbols Verbal Speech Language Written 1. 2. Facial Movement Destine & Body M. 3. Gaze & Eye Contact 4. Body poster & contact 5. Use of Space 6. Use of Time 7. Appearance & Cloths 1. Jargon Trap M. T 2. Use +VE words for hope 3. Be Rationale to: Conceal, justify, explain, cover other feelings describe and Correct y feelings, and share other Meta Communication Deep thinking-understanding - truth CHS456 Johali2012 69 National–International INTRA&INTER Social & Cultural Organizational Group INTERPERSONAL INTRAPERSONAL Adapted HUMAN COMMUNICATION & HE LEVELS 1. Self interact to interpret reality & create messages. At this basic level, the central 2. 3. communicative processes of encoding & decoding are performed to help us coordinate our meanings and messages at 2. Interaction, negotiation and relations between two individuals, its effectiveness based on level 1, this level is the most important to health communication and, thus, it is important to gain at least the “Seven Top Health Communication Skills (Pagano & Ragan, 1992, 29) . Interaction of three or more individuals to adapt & achieve common tasks, its effectiveness based on 1. & 2. e.g; medical team. 4. Encompasses 1, 2, & 3, it is important to develop effective formal channels and informal networks e.g; hospitals & health centres. 5. Intra & Inter Social/Cultural joints all the above, it can be within more than two different groups, communities in one organization, nation or nations. 6. This is the highest level of communications, e.g; national and international CHS456mass media & satellites. Johali2012 70 HCP COMPONENTS & STEPS The Sending Person who has an idea, thought, feeling, value, attitude, information. The Encoding Process: the sender mental perception by which he/she thinks, translates and codes the communication message. The Message the product of the encoding process which formulated in a certain order hoping that it will be understood by receiver. The Channel of sending the message, our senses (sight, sound, touch, taste, smell) are the common channels at the basic intra- & interpersonal levels and, the most used are sight and sound or speech. The Interference the step of preventing the sending message from distortion (the message sent being the message received). To prevent your message, you have to understand the receiving personality and to use the appropriate codes and channels for him/her. The Receiving/ Responding Person : as sender …. have to interpret the sent message without any distortion. The Decoding Process the receiver mental perception by which he/she thinks and translates the encoding massage as it is being sent. To do so, the sending message must be coded according to the receiver’s needs, knowledge and characteristics. The Making of Meaning the massage which attempts to avoid expected outcomes. If you are passive you have negated and sat on your own feelings at some cost to yourself. Johali2012 71 CHS456 The Feedback & Evaluation: checkout & promote feeling NHEPC HCP NETWORK 2. Thinks 3. formulates massage Encoding Process0 Or: he has not got my massage try again 7. Decoding Process 8 Makes meaning 4: sends via 5. Interference 1 Sender Channel : Feelings Sight Sound Touch Smell Either Keep it Receiver 6 OR 9a: I well lat him Know how 9b: feedback Ed : checkout Mansour Artist 10 th.Hajah 31 Discover: - Who is CN & P ? - HC Components & Steps - Where is: the Health Profession ?; Patient; Who usually Decode and who Encode Source: Johali2012 CHS456 72 THE SEVEN (7) TOPS HEALTH COMMUNICTION SKILLS Give accurate & Adequate Feedback Listening Carefully Interpreting Accurately Giving Clear Directions Treating Others in Professional Manner Communicating Information Clearly Establishing One’s Credibility CHS456 Johali2012 73 APCHER QUALITY Assertive Patient Centred HE’R with Best Evidence CHS456 Johali2012 74 Managerial NHEPC Communicative Styles The Highest the Most Trusted Styles “Ethically – Humanity” the Highest Quality +VE ASSERTIVENESS (Confidence, Self assure, Be empathic – Other Feelings; Communicate & Educate without Attack..): Give patient freedom for direct expression of ideas, opinions ands desires. The intent of Assertive CN behavior is to communicate in an atmosphere of TRUST. It is “how to communicate straight without hurting others”. It focuses “On What we should Do rather than What we want others to Do”. The Assertive communicate message caries Feeling, Behavior and Effect”: Example: I Feel Angry (Feeling), when you are not comply with medication (Attitude/Behavior) and/thus, I blame You (Effect) PASSIVE AGRESSIVENESS (Indirect Attack, non assertive): Indirect attack, who has the intent to attack, but is carried out in an indirect avoiding way. Passive behavior designed to avoid conflict at all cost; The Passive or non assertive do not say what they really think out of fear, that other may not agree. PT “hides” at corner or behind window of Pharmacy..The recipient/Receiver is often left Puzzle & Confused?! OFFENSEVE AGGRESSIVE (Direct attacker; Not friendly, non peaceful/ not healthy): Agg. People seek to “win” in conflict situation by dominating or intimidating (threatening) other. Offensive is the direct attack behavior by which PTs decide to hit out others using blame and putdown words. e g:“As usual you are being hopeless”. Aggressive/Offensive PT, the persons who promote their own interests or points of view indifferent way or hostile to the feeling, thoughts and needs of others. CHS456 Johali2012 The Lowest the Less Trusted Styles “Ethically – Humanity” the Less Quality -ve 75 Reasoning APCHER NHEPC QUALITY APCHE’R based on the Assertive Style the FEELING of others the patients “PT as a patient” this is the Ideal way to grantee quality In addition to ”PT caries patients’ feelings”, It covers all related scientific concepts that we have learn with (e.g Carol Rogers father of Person Centred Psychotherapy”; Jean Piaget; Bloom; Dewey....etc) It is arranged “Highest to the Lowest” effect on the quality of human communication & education Its overall goal is Quality, the intent goal, the desire and the need for every person, patient and every community and nations. APCHE’R Quality Model consists of “Three Major Models”: Patient Centred NHEC the P Self Awareness Assertive based NHEPC the Style Best Evidence NHEPC the scientific research & assessment Patients and any health education "Persons or customer the Centre of any NHEPC planning and activities. P's nature, characters, abilities, needs, interests, problems, risk factors and all the related information are the foundation "the Best Evidences" by which we promote, motivate and grantee its "Readiness and Willingness. By scientific research we collect these best evidences. All of these HE processes are done under "Assertiveness" concept by which: CN feels that he is the Patients carrying his sickness and healthful feelings. CHS456 Johali2012 76 NHEPC APCHER Quality CHS456 the Model Johali2012 77 NHEPC METHODOLOGIES & TECHNOLOGIES CHS456 Johali2012 78 METHODOLOGIES & TECHNOLOGIES Define & Reasoning CHS456 the Scientific Bases: Why & How to choose the appropriate ? Johali2012 79 M & T MAJOR METHODS CHS456 Johali2012 80 MAJOR CHS456 TECHNOLOGIES Johali2012 81 Example of HEMLT Strategies ( CAP Objective Based Methodologies) Teaching Objectives O kinds Strategy (M \T) Patient Status 1. Present \Provide Information - Cognitive - Lecture - AVAs - Reading Passive 2. Encourage understanding - Cognitive - Affect - Problem Solving - G work - Programme d learning Active 3. Encourage investigation of attitude and value - • G. work • Share experiences Active • Demonstrati on • Games • Simulation Active 4. Develop psychomotor and interpersonal skills, Affect Cognitive -Cognitive -Affect -Psycho Advantages • Economic times and resources • Large patients & information Disadvanta ges • Quantity only • Passive Think/Prom ote - Example (Recommend) • Large group of patient at 1st visit M TYPES WITH KINDS OF LEARNING; STATUS OF LEARNERS PLUS ADVANTAGES & CHS456 Johali2012 82 DISADVANTAGES 82 HEALTH PROBLEM AND BEHAVIOR BASED CHARACTERS M & T RELATION TO OBJECTIVES & COMPLEXITY Diagnostic Criterion HEMLT Strategies Prevalent category Desired Cognitive Educational Outcomes Affect Audiovis ual aids Lecture Individual instruction Mass media Programm ed Learning \ ETV Inquiry Learning Simulation s and games Peergroup discussion √ √ √ √ √ √ √ √ √ √ √ Psycho. HI Simple √ √ Modeling Behavior modificati on √ √ √ Complexity Complex HB Simple Complexity Complex HB Duration Short √ √ Frequency HB Extent Infrequent √ √ √ √ √ Long HB √ √ √ √ √ √ √ √ √ √ √ √ Frequent Rare Widespread HB Nature Additive √ √ √ Substantive CHS456 √ Johali2012 √ 83 agnos Recommended HEMLT Strategies To Age; Believe & Socioeconomic Status Prevalent category terio e lieve HBM cioec omic tue HEMLT Strategies Audiovi sual aids Lectur e Individu al instructi on Mass media Program ed Learnin g \ TV Inquiry Learnin g Simulati ons and games √ √ √ √ √ √ √ √ √ √ Infants and preschool children Primary school children √ √ √ √ Secondar y school √ √ √ √ √ √ Adults Moderate √ √ Weak √ √ √ Peergroup discussio n Modelin g Behavio r modifica tion √ √ √ √ √ Strong √ High intermedi ate CHS456 √ Johali2012 84 TECHNOLOGIES 1 ADVANTAGES _ DISADVANTAGES & PRACTICE WITH DIFFERENT SITUATIONS Technology Advantages Disadvantages 1.Pilnted materials (leaflet; folder; poster; pamphlet ; booklet; books, handouts • Allows self-pacing. • Learners can relay to when required . • Reduces need for note-taking • Hand-outs can be made special to individual learning needs. • Supplements teaching session •Books expensive and rapidly out of date. • Hand-outs must be carefully planned and used appropriately should not replace teaching. • Copyright law prohibits mass duplication of copyrighted material. In discussion of nutrition, Hand-outs about essential Food groups and how to assess if family members are eating properly 2.Models of life, e.g. skeleion . •Three-dimensional • Resemble reality. • Allow for close examination • Allow for practice. • Visual and tactile senses stimulated. •Ma/be expensive • Cannot replace reality • Useful for small groups only. Use of doll in antenatal class demonstrations for expectant parents. 3. Real specimens • Present reality • Three – dimensional • Visual and tactile senses stimulated • Not easily available • Useful for small groups only • May be expensive, difficult to store. 4.Graphicscharts,posters, drawing, photographs • Visual sense stimulated • Promote organization and correlation of material • Help to approximate reality • Easily stored, retrieved • Production of materials should be of high standard • Useful for small groups only CHS456 Johali2012 Example Used for discussion different behavioral health problems: e.g. drugs, alcohol, smoking, accidents …. 85 TECHNOLOGIES 2 Advantages _ Disadvantages & Practice with different situations Technologies Advantages Disadvantages Example 5. Boards: Flannel, magnetic, bulletin and e-black boards • Larger audience • Easy to assemble and use • Can use repeatedly • Others may participate • Visual sense stimulated • Limited usefulness • Inappropriate for certain purposes and audiences • Work erased For young diabetics , choosing correct food items and creating a daily menu 6. Field Trips • Motivating • Active involvement • Presentation of reality • costly in time for organization and accomplishment • Transport needed • For small appropriate groups only For psychiatric patients , visits to shops to assess appropriate selection of clothing items 7. Overhead projection • Visual sense stimulated • Easy to prepare and use • Available to large audiences • Can be preplanned or used on spot • can illustrate process stages and develop material • Allow participation of learners • Electricity required • Equipment costly • Transparencies need to be carefully planned for effective use With renal failures patients, to explain the mechanism of kidney function and to illustrate what renal allure means 8. Slides, film strips • Available to large audiences • Can be adapted to self – learning programmer • Easy reproduction • Visual and auditory senses stimulated • Need partial darkness for viewing • co lour slide duplication expensive • Need careful presentation / side order planning for effective use For patients with recent colostomies , slide presentation of appliance management CHS456 Johali2012 86 TECHNOLOGIES 3 Technique s Advantages Disadvantages 9.Filme , video , television • Resemble ‘look like’ reality • Available to large audiences • Effective illumination of attitudes and values , can demonstrate skills • Visual and auditory senses stimulated • Need careful selection and previewing • Need meaningful introduction and follow – up discussion • costly • Electricity required • All information in film may not be appropriate • No self – pacing • Need proficient with equipment With high – school students , cases of drug dependency can be viewed and used as basis for discussion 10. Tape recordings • Auditory sense stimulated • Self – pacing • Available to large audiences • Small recorders can be inexpensive , • Can be used for a variety of reasons • Quality recordings may be difficult to obtain • Person using must be proficient with equipment Tape initial session of a group in which health attitudes are discussed . Play back in later session to assess any changes 11. Expert contributo rs • Present reality • May provide a point of comparison • May command respect because of knowledge • May not be easily available • May be expensive • May not be appropriate Inviting an adolescent diabetic who is coping well to speak to a group of new juvenile diabetics about how he feels in relation to his condition CHS456 Johali2012 Examples 87 87 NHEPC HYPER TECHNOLOGY Moving QHEPHAP in Moving from Printed Material & Blackboard to Digital CHS456 Johali2012 88 88 NHEPC PLANNING FOR ZD NHEPC CHS456 Johali2012 89 PLANNING Defining Terms just the most repetitive CHS456 Johali2012 90 Planning Defining most constant Terms CHS456 Johali2012 91 Planning Defining most constant Terms CHS456 Johali2012 92 PLANNING Definition & Principle CHS456 Johali2012 93 TRADITIONAL PLANING (TP)? VS PLANNING FOR QUALITY NHEPC? WHY PLANNING FOR HEALTH EDUCATION?: To prepare well, manage, validate and grantee the quality of H. E. activities & o utcomes LEARNING & PLANNING FOR QUALITY CAN BE SIMPLIFIED AS: LEARN TO UNDERSTAND LEARN TO PLAN QUALITY OF HEALTH As we have taught and may be learnt, for understanding the boundaries and its concepts, normally, we have to start by defining health education; its goals and objectives; its philosophical and theoretical concepts; methodologies, technologies and research and finally, the planning process. The TP is: Inputs Outcomes QUALITY EDUCATION/WHAT QUALITY HEALTH/WHY Does it male sense?; Does it assure quality? In order to plan for the quality of health of clients, people and community, it is recommended to “start from the end or bottom, from the field (patient, clients, people, community) as follow: Inputs Outcomes QUALITY EDUCATION /HOW Johali2012 QUALITY HEALTH /WHY CHS456 Further use of these Quality Planning Concepts in the PRECEDE 94 NHEPC PLANNING The PRECEDE Administrative Diagnosis Education al Diagnosis Behavioral Diagnosis Epidemiology & Social Phase 6 Phase ----5--,--4-Phase 3 Phase 2 , 1 Impact Outcomes Predisposing HEP(HEMLT) Components Reinforcing Behavior \ non Behave Healthy - non Healthy Healthful Life Quality Enabling 7. Evaluation Process Impact Factors Outcomes PRECEDE is P……….; .………. ; …….. Causes in ……….. Diagnosis ………. PRECEDE is Predisposing; Reinforcing; Enabling Causes in Educational Diagnosis Evaluation CHS456 Johali2012 - Draw or Fill gaps ….. Focus on Phases; PER & Behavior ? 95 PLANNING the PRECEDE PRECEDE is P……….; .………. ; …….. Causes in ……….. Diagnosis ………. PRECEDE is Predisposing; Reinforcing; Enabling Causes in Educational Diagnosis Evaluation - Draw or Fill gaps ….. Focus on Phases; PER & Behavior ? CHS456 Johali2012 96 PLANNING The PRECEDE Apply & Evaluation process CHS456 Johali2012 97 PLANNING The PROCESS PLANNING CYCLE MODEL (PPCM) CHS456 Johali2012 98 Johali Concise QNHEPC The QHL CHS456 Johali2012 99 NHEPC Turning Theory Into Practice التطبيقات العملية ممارسة معتمدة على براهين علمية ...ال جودة لعمل بال علم Practice & Turn APCHER to Best Evidence ANHEPC ”دون وهيئ ذاتك أول بأول وفق تسلسل المقرر“ 100 Johali2012 CHS456 Let us read, observe and think What this means ? Individual ‘write’ – Peer ‘write’ – Small Groups “write-compare’ February 27, 2012 Latest from Dr. Michael Cutler The Nutritious Food That Can Transform Your Health » If you're worried about how many carbohydrates you eat, you're worried about the wrong part of your diet. Don't think about food in terms of carbs, focus instead on eating raw, whole foods. Fruits and vegetables offer the promise of optimal wellness. Their nutrients can spell the difference between enjoying great health or succumbing to chronic disease. More » Easy Health Digest™ continues below... The invisible health destroyer - making you feel so miserable... Dangerously high acid levels in your body may be the hidden cause behind your age-related health problems. And if you drink soda... eat meats and dairy products... patronize fast food joints... and enjoy sugary deserts—the typical American diet—I can almost guarantee it! Leading research institutions and medical journals agree that balancing your pH can help put an end to heart problems... joint pain... high blood pressure... uncontrollable cholesterol... blood sugar problems …fatigue CHS456 Johali2012 101 problems... More.. Play Inpatients & NC roles How do you feel ? What do you want … like and dislike ? Who, How , When & Where do you need counseling ….. Do you ? When you visit PHC or Hospitals ….. Do You Notice Which “Styles; Strategies & Methods Do You ….like ‘Top three’ Dislike ‘Top three” … Why ? Which more meaningful ? Which “Technologies” Do You ….like ‘Top three’ Dislike ‘Top three” … Why ? Which more meaningful ? CHS456 Johali2012 102 Set NHEPC Plans ? CHS456 Johali2012 103 Set NHEPC Plans ? http://www.youtube.com/watch?v=q8jX0CA1ALY&feature=related Dining Programs in Patient Centered Care - Part 1 – 6 CHS456 Johali2012 104 Diabetes Education Diabetes is a chronic, complex disease that changes over time. Through self-management individuals make the majority of decisions and actions that determine their level of blood glucose control. To be an effective manager of your disease, knowledge and experience are necessary. The amount and type of knowledge required depends on the goals each individual sets for themselves as to the level of diabetes control they desire. Diabetes is a disease in which good control can help prevent or delay complications. The Marshfield Clinic Diabetes Education program is recognized by the American Diabetes Association (ADA) and adheres to national standards for diabetes selfmanagement education. Our team consists of registered nurses and registered dietitians who are experienced in diabetes management. Many of the team members are certified diabetes educators (CDEs), which indicates an advanced degree of education and experience in diabetes education. Diabetes management is an individualized program, providing education and training as needed. Diabetes education is an ongoing process, since the need for education will continue to change as lifestyles change and new technologies become available. The role of Marshfield Clinic Diabetes Education is to help individuals understand and use self-management tools to achieve optimal blood glucose levels. CHS456 Johali2012 105 Others CHS456 Johali2012 106 HE FIELDS & SPECIALTIES; ASSOCIATIONS; RESOURCES & References CHS456 Johali2012 107 HE FIELDS & SPECIALTIES; ASSOCIATIONS; RESOURCES & References CHS456 Johali2012 108 HE FIELDS & SPECIALTIES; ASSOCIATIONS; RESOURCES & References CHS456 Johali2012 109 HEALTH EDUCATION FIELDS & SPECIALTIES HE is a part of any health professions, institutions & activities; Health Education has many (FEILDS/TYPES) Specialties, The Majors Are: Health Promotion, Health Promotion & Education, the new the Millennium name General/Public Health Education (G/PHE) Hospital Health Education (HHE): Patient & Outpatients Primary Health Care Education (PHCE) Community Health Education (CHE) School Health Education (SHE) Nursing Health Education (NurHE or HENUR Clinical Nutrition Health Education (CNHE or HENUT) Environmental Health Education (EHE) Occupational & Safety Health Education (OSHE) Chronic Diseases Health Education (CDHE): Diabetic, HBP, Cancer…. HEMLT; HEHA; HEPT; HERT………… HE CN\NutHE These specialties can be reorganized as: Individual or Personal; Group, Community; Public; Institutional or Organizational ….Health Education (Only the first … the rest Just for General Information) CHS456 Johali2012 110 LOCAL HE ASSOCIATIONS RESOURCES In Saudi Arabia, despite that there is no special “Association or Board”… as it is the case of global HE, there are many HE Resources. In addition to a department within every government and private health service sectors, the major HE government sectors are: Department of Health Education, General Directorate of Preventive Health, Ministry of Health, which is located at “Al Suliamnia, King Abdul Azis Road. Department of Health Education, King Khalid Eyes Specialist Hospital, Riyadh. The most active HE hospital department now, mainly in regarding of HE symposium. Department of Health Education, Kin Fahd Specialist Hospital, King Abdul Aziz Medical City, National Guard. Department of Health Education, Riyadh Military Hospital. It is the oldest department, and it was the most active hospital HE department mainly with HE researches & materials. Department of Health Education, King Fisal Specialist Hospital & Research Centre. Department of Health Education, General Directorate of Schools Health, Ministry of Education, “the place of “Uniceef HE Seat Fond”. Department of Health Education, Security Force Hospital, Riyadh. Academic Department of Health Education, College of Applied Medical Sciences, King Saud University, Riyadh. The lonely academic department. It establishes at 1403 AH. Saudi Health Specialties Council (Association), It services all health professions including heath education specialists & heath educators. Our Live: the Saudi Volunteer Association for Health Education “independently, you have to discover the activities of these sectors and other national sectors” CHS456 Johali2012 111 Our Live حياتنا الجمعية الخيرية السعودية للتثقيف الصحي Independently, you can discover this NA if still (R Ring Road Ex10 & 11East)?!! As Reflective Assignment CHS456 Johali2012 112 Global Associations & Resources CHS456 Johali2012 113 NHEPC Summary CHS456 Johali2012 114 The Lecturer Publications Further Future References HEPAHP in Press CHS456 Johali2012 115 With My Great Best Wishes CHS456 Be Excellency in ever think Be Critical Thinkers Be Creative; & Meaningful Assertive PTs & Learners Lifelong and Day After Johali2012 116