Pain and Pain Relief
- a Brief Introduction
Dr. Reino Pöyhiä, MD, PhD
Consultant in Anaesthesiology
Special Competence in Pain Medicine, Cardiac Anaesthesia and
Palliative Medicine, Finland
Associate Professor of Anaesthesiology and Palliative Medicine,
Helsinki and Turku University, Finland
Head of the Dept of Anaesthesia, Helsinki Univ Central Hosp
What is pain?
• PAIN is an unpleasant sensory AND emotional
experience associated with actual or potential
tissue damage OR described in terms of such
damage
• IASP = International Association for the Study
of Pain 1979
→ physiological sensation
→ emotional experience
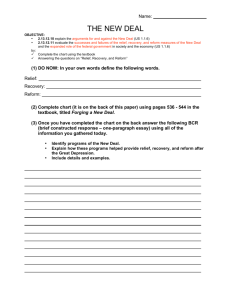
Physiology
Descartes 1677,
Tractus de homini
INHIBITORY DESCENDING TRACT
Different types of pain – different
treatments
Types of pain
Examples
Treatments
Somatic (nociceptive) pain
Rheumatoid arthritis
Visceral pain
Acute postoperative pain
NSAID, paracetamol,
steroids, opioids
Nerve (neuropatic) pain
Postherpetic neuralgia
Antidepressants (AMITR),
antiepileptics (CARBAMAZ)
Psychogenic pain (?)
Psychological problems
Psychological support
Non-cancer chr pain
Ischaemic heart pain
Nitrates, NSAID,
neuropathic pain drugs,
(opioids)
Cancer pain
Bone metasthases
NSAID, opioids, adjuvants
Pain in advanced and
progressive disease
AIDS
NSAID, opioids, adjuvants
- Think mechanisms!
Acute Pain
Labour pain, postop pain
Mechanism based!
Chronic Pain (> 6 months)
Cancer pain, arthrosis
Mechanism based!
Visceral pain
Assess and record pain
• What´s causing the pain?
• Intensity of pain
– when resting/moving
– before and after treatment
• What pain prevents
• Observation of “pain-related behaviour”
• Surrogates of acute pain
– HR ↑
– BP ↑
– RR ↑
Set a goal
• Intensity of pain ALWAYS < 3/10
- if not, something must be done …
• In cancer pain / palliative care
– pain-free night
– improvement in functionality
• Assess and follow
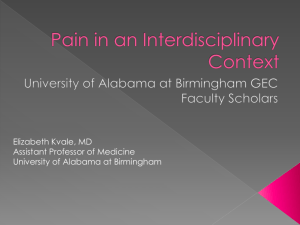
Perception
- brain: ACC, SSC
Effect site of analgesics
opioids
α2-agonists
paracetamol
Modulation
Psychotherapy (CBP)
- spinal cord
Antidepressants, antiepileptics
- brain stem, brain
- serotonin ja noradrenalin ↑ in the
inhibitory descending tracts
- Inhibitory descending tracts
Transmission
- Nociceptive signal ”goes” in
sensory nerves to the dorsal
column in spinal cord →
projection neuron →
spinothalamic tract → brain
TNS, DCS
α2-agonists
opioids
local anaesthetics
Transduction
- nociceptive stimulus in
peripheral nerve endings
-action potential in Aδ/C
fibers
local anaesthetics
NSAID
physical therapy
ointments, gel
Acute postoperative pain
What can acute pain cause?
– respiratory depression
– cardiovascular stress
– endocrine stress
– abdominal irritation (ulcus)
– muscle spasms
– immobilisation, thrombosis
– psychologic distress
– genetic changes in the body ?
Poor postoperative pain relief
•
•
•
•
Ethically wrong!
Prolongs recovery from surgery
May lead to chronic pain!
An international problem
– which could be (easily?) solved (!)
Chronic postoperative pain
Kehlet et al. Lancet 2006; 367: 1618-25
How well are we doing?
Wu & Raja, Lancet 2011
• the number of the patients with moderate to
severe postoperative pain ↓ about 2%/y
1973–1999
• but still 15-40 % patients have moderate to
severe pain after surgery
Postoperative pain relief
www.ebandolier.com, Feb 2003
•
•
•
•
good surgery
preoperative planning
multimodal approach
possibilities:
–
–
–
–
opioids
NSAIDs, paracetamol
antiepileptics, antidepressants
blocks
• choiche depends on
– procedure
– patient
– resources
How to improve postop pain relief?
1. Assessment of pain
2. Protocols
-
must be composed locally – by an expert group
each patient should get NSAID/paracetamol at fixed intervals
tramadol PRN after minor surgery
pethidin or oral morphine PRN
3. Individual tailoring
-
if preoperative pain, consider carbamazepine preoperatively
if protocols fail, ketamine im or orally in small doses
intercostal block with bupivacaine for cholecystectomy
wound injection of bupivacaine
Chronic pain
What can chronic pain cause?
– depression
– insomnia
– mental irritation
– helplesness
– loss of apetite
– loss of social contacts↓
– libido ↓
– human value ↓
– genetic changes in the body ?
Pain in HIV/AIDS
Oral/skin
Visceral
Somatic
Neuropathy/Headache
Kaposi´s
Sarcoma
Oral cavity
Herpes zoster
candidiasis
Tumors
Gastritis
Pancreatitis
Infection
Biliary tract
problems
Rheumatological
disease
Back pain
myopathies
HIV related headaches:
- encephalitis, meningitis
Iatrogenic
- AZT
- DDI, D4T toxic
neuropathy
Peripheral neuropathy
Herpes zoster
Alcohol, malnutrition
HIV unrelated:
- tension headache,
migraine etc
What is causing pain in cancer
patients?
Cancer with different mechanisms!
–
–
–
–
Distension of visceral organs
Arterial/venous embolisms
Bone methastases → algesic substances from the bone
Nerve compression or infiltration
Side-effects of the oncological therapies
– Nerve damage due to radiation therapy/ chemotherapy
– Postsurgical syndromes
Non-malignant pain
– Muscular pain
– Angina pectoris
Cancerpain prevalence
van den Beuken-van Everdingen et al. Oncology 2007; 18: 1437-49
• Prevalence
– at all stages: 53%
– at the end-of-life (methastatic cancer): 64%
• Moderate to severe pain in
> 1/3 of patients during active treatments
> 2/3 of patients at the end-of-life
Undertreatment of cancer pain
- an international problem
•
•
•
•
•
Japani: 75 % Okayama -04
Hollanti: 65 % Enting -07
Saksa: 61 % Felleiter -05
Italia: 10-55 % Apolone -09
Kanada: 40-48 % Krou-Mauro -09
Undertreatment - why?
• patient does not tell about the pain/ask for relief
• doctor does not listen/alleviate
– lack of basic knowledge
– lack of pain specialists
• both – society: fear of opioids
– dependency
– tolerans
– side-effects
• shortage of analgesics
• lack of other resources
NIH Cancer Institute, British Pain Society
WHO cancer pain relief with analgesics
– By the mouth
– By the clock
– By the ladder
1986 Geneve
← concomitant use of different drugs
with different mechanisms
75-80 % can achieve excellent pain
relief with the WHO guide
+ breakthrough pain relief
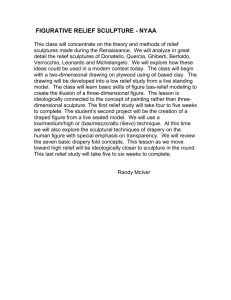
WHO analgesics ladder
3 severe
■ Morphine
2 moderate
■ Tramadol
1 mild
■ (A/Codeine)
■ ASA
■ ± Adjuvant
■ Acetaminophen
■ ± NSAIDs
■ NSAIDs
■ ± Adjuvants
(amitriptyline,
carbamzepine, ketamine)
■ ± Adjuvants
■ ± NSAIDS
IBUPROFEN + DICLOFENAC
TRAMAL + MORPHIN
BUT YES:
IBUPROFEN + (PARACETAMOL) +
(AMITRIPTYLINE) + TRAMADOL
IBUPROFEN + (PARACETAMOL) +
AMITRIPTYLINE + MORPHINE
How to use morphine for cancer/AIDS pain?
–
–
–
–
–
individual tailoring
by the clock + PRN!
dose ↑ → effect ↑
treat side-effects: start always a laxative
when pain increases increase the dosing
•
•
by 30-50 % of the previous daily dose OR
by adding the PRN doses to the maintenance dose
Side-effects of opioids
Addiction?
– Psychological: NEVER!
– Physiological: ALWAYS! → don´t stop opioids immediatedly but
slowly, if needed
Tolerans?
– Vaihtelevasti, valmisteen vaihto voi auttaa!
Other:
– Constipation → laxatives, stool softeners, stimulants
– Nausea, vomiting → antiemetics; haloperidol, metoclopramide,
5HT-inhibitors
– Itching
– Respiratory depression: only in acute use
– Dizziness, sleepiness, hallucinations
Side-effects vs analgesia at E-o-L
• PAIN RELIEF >> SIDE-EFFECTS (unless
untolerable)
Summary
• pain analysis is important
• record the intensity and influence of pain before and
after treatments
• treatments of pain should be based on pain
mechanisms – multimodal analgesia
• undertreatment of pain is common
– may severe effects on recovery
•
•
•
•
defined protocols may improve postop pain relief
WHO cancer pain relief programme is highly effective
don´t be afraid of opioids
pain relief can be increased with supportive methods
 0
0