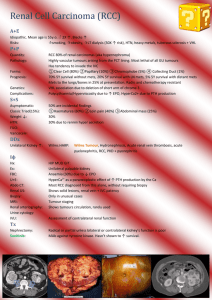
VHL
advertisement

Roma, 22 febbraio 2013 Highlights in the management of renal cell carcinoma Clinical and Molecular Predictive factors to molecularly targeted agents: what we know so far.. Enrico Ricevuto, Eleonora Palluzzi Oncologia Medica Ospedale San Salvatore Università dell’Aquila Renal cell carcinoma Evolution of medical treatment Markers None “One fit (unfit) all” Renal cell carcinoma Evolution of medical treatment Parameters None Bio-Clinical Patient Tumor Drugs “One fit (unfit) all” “One fit some” (>10%) fitness (age, comorbidities) prognostic risk prediction (safety/toxicity, efficacy) ccRCC Predictive markers of target therapy Bio-Clinical Hypertension (>90 mm/hg DBP) LDH Hypothiroidism (increased TSH) Hypertension Biomarker of Efficacy with Sunitinib B Rini, J Natl Cancer Inst 2011; 103:763-773. Diastolic blood pressure Biomarker of efficacy with axitinib in solid tumors OS with landmark at 8 weeks. B Rini, Clin Cancer Res; 17(11); 3841–9.2011 Serum LDH Biomarker with Temsirolimus Andrew J Armstrong et al, J Clin Oncol 30:3402-3407. Hypothyroidism (increased TSH) Biomarker of activity with TKI in solid tumors Objective Remission According to Response Evaluation Criteria in Solid Tumors Based on Increased Thyroid-Stimulating Hormone Levels Schmidinger M, Cancer 2011 Hypothyroidism (increased TSH) Biomarker of efficacy with TKI in solid tumors Schmidinger M, Cancer 2011. Renal cell carcinoma Evolution of medical treatment Markers None “One fit (unfit) all” Clinical “One fit some” (>10%) Monogene “One fit few” (1-10%) VHL Other genetic alterations Heterogeneity (tumor/metastasis) VHL/HIF epigenetics alterations Renal Cell carcinoma Different diseases Different histology Different genes Different clinical courses Different response to therapy Renal Cell Carcinoma Pathology Clear cell (75-85%) Proximal tubule origin Abnormalities in chromosome 3p Chromophilic (15%) 85% of these are diagnosed as stage I tumors Also proximal tubule in origin, but 3p is normal Trisomy 12, 16, 20 can be seen Chromophobic (5%) Oncocytic (uncommon) usually not aggressive Collecting duct origin 11q13 rearrangements in some cases Collecting duct (Bellini’s duct) tumors – very rare Unclassifiable (<3%) – worse prognosis Renal Cell Carcinoma Morphology and Genetics Renal Cell carcinoma Disease of cell metabolism: Biomolecular Complexity Pathways that respond to metabolic stress or nutrient stimulation VHL oxygen and iron sensing MET LKB1-AMPK energy sensing FLCN binds AMPK and might interact with the cellular energy and nutrient sensing TSC1 TSC2 downstream of AMPK and negatively regulates mTOR in response to cellular energy deficit FH central role in the mitochondrial tricarboxylic acid cycle SDH coupled to energy production through oxidative phosphorylation pVHL targets hypoxia-inducible factor (HIF)-α for ubiquitin-mediated degradation Sporadic ccRCC Genetic alterations of the VHL gene LOH 3p 24-25 Intragenic mutations Hypermethylation Biallelic loss 78-96% 51-71% 5-20% 50-75% Sukosd et al, Canc Res’03, 63, 455 Kondo et al, Gene Chrom Cancer’02, 34, 58-68 Banks et al, Canc Res’06, 66, 2000-11 Spectrum of VHL mutations cumulative data of 1244 mutations reported in the literature Young A et al, Clin Canc Res’09, 15; 7582 RCC Spectrum of VHL gene alterations Young A et al, Clin Canc Res’09, 15; 7582 VHL genetic alterations Prognostic relevance Young A et al, Clin Canc Res’09, 15; 7582 Choueiri et al, J Urol. 2008; Rini BI, et al. BJU Int. 2006 Choueiri et al, J Urol. 2008; Rini BI, et al. BJU Int. 2006 Klatte et al, Clin Canc Res’07 Metastatic ccRCC Heterogeneity Gerlinger M et al, N Engl J Med 2012;366:883-92 Metastatic ccRCC Heterogeneity Gerlinger M et al, N Engl J Med 2012;366:883-92 Expanded HIF signal output activates mediators of metastasis CXCR4 expression correlates with poor prognosis and metastasis in ccRCC and is inducted by VHL loss. Vanharanta S et al, Nature Medicine 2013 DNA demethylation allows CYTIP expression in metastatic ccRCC Vanharanta S et al, Nature Medicine 2013 Current renal cell carcinoma biomarker initiatives 1) EuroTARGET 2) SCOTRRCC 3) Predict Consortium 4) TCGA 5) CAGEKID Vasudev et al. BMC Medicine 2012, 10:112 Renal cell carcinoma Evolution of medical treatment Markers None “One fit (unfit) all” Clinical “One fit some” (>10%) Monogene “One fit few” (1-10%) Multigenes “One fit one” (<1%) Multiple biopsies Genetic and epigenetic alterations Multiple drugs anti-angiogenesis mTOR-inh Need of drugable and actionable targets mRCC Angiogenesis inhibitors Sonpavde G Exp Opin Invest Drugs 2008 mTOR inh image Why should we need clinical and biological markers? Individual tumor heterogeneity differential clinical outcome aggressiveness efficacy OS differential biology Biological heterogeneity Genetic alterations VHL M M 1 2 3 4 M M Metastatic ccRCC Heterogeneity Gerlinger M et al, N Engl J Med 2012;366:883-92 Open question Multiple biopsies Hand-foot syndrome (HFS) as a potential biomarker of efficacy in patients (pts) with metastatic renal cell carcinoma (mRCC) treated with sunitinib. Methods: Analyses included pooled data from 770 pts who received single- agent SU as 50 mg/d on a 4-week-on/2-week-off schedule (n=544; 71%) or 37.5 mg continuous once-daily dosing (n=226; 29%). Median PFS and OS were estimated by Kaplan-Meier methods and compared between pts with vs without HFS using a log-rank test. ORR was compared by Pearson's chi-square test. Tumor response was assessed by investigators and adverse events were recorded regularly. Multivariate and time-dependent covariate analyses were performed. Results: Of 770 pts, 179 (23%) developed any-grade HFS, compared with 591 (77%) who did not. Most instances of HFS (63%) initially occurred during the first 3 treatment cycles. Pts who developed HFS had significantly better ORR (55.6% vs. 32.7%), PFS (14.3 vs. 8.3 mo), and OS (38.3 vs. 18.9 mo) than pts who did not develop HFS (p<0.0001). In a multivariate analysis, SU-associated HFS remained a significant independent predictor of both PFS and OS (and of OS by time-dependent covariate analysis). Conclusions: In mRCC pts, SU-associated HFS was significantly and independently associated with improved clinical outcomes. Overall, pts who did not develop HFS still had substantial benefit from SU. However, the presence of HFS identified a subset of pts that manifested highly favorable efficacy results with SU. These findings suggest that development of HFS Michealson MD, J Clin Oncol 2011; 29 Renal Cell carcinoma Disease of cell metabolism Pathways that respond to metabolic stress or nutrient stimulation VHL oxygen and iron sensing MET LKB1-AMPK energy sensing FLCN binds AMPK and might interact with the cellular energy and nutrient sensing TSC1 downstream of AMPK and negatively regulates mTOR in response to TSC2 cellular energy deficit FH central role in the mitochondrial tricarboxylic acid cycle SDH coupled to energy production through oxidative phosphorylation ccRCC Prognostic and Predictive Biomarkers DNA RNA Protein FISH IHC Elisa Mutations Western VHL HIF1 alfa X X CAIX X VEGF X sVEGFR-2 X TIMP-1 X Ras p21 X Bui, Clin Canc res’03 Atkins et al, Clin Canc Res’05 VHL genotype in ccRCC Structural alteration Point mutations Methylation Prevalence of mutations Functional relevance Diagnostic strategy 60% Gain of function Direct Sequencing Scanning for unknown mutations Clinical implications Predictive anti-VEGF VHL gene Structural Features Chromosomal locus 3p24-25 Exons 3 mRNA 4.7 kb. Proteins pVHL30 213 aa. (28-30 KD) pVHL19 160 aa. (18-19 KD) Hypoxia-inducible factor (HIF)-α Transcriptional activity: Pathways and Genes Energy metabolism: increase in glycolytic pathway Glut-1 Angiogenesis VEGF VEGFR PDGF Ang-2 FGF Tie-2 PH regulation CA IX Proliferation TGF-alfa/beta CXCR IGF Apoptosis p53 NIX BNIP-3 Erythrocitosis EPO Hypoxia-inducible factor (HIF)-α Transcriptional activity: Pathways and Genes Energy metabolism: increase in glycolytic pathway Glut-1 Angiogenesis VEGF VEGFR PDGF Ang-2 FGF Tie-2 PH regulation CA IX Proliferation TGF-alfa/beta CXCR IGF Apoptosis p53 NIX BNIP-3 Erythrocitosis EPO Renal Cell Carcinoma Evidence for VHL initiation Both sporadic and VHL disease-associated ccRCC display loss of VHL HIF activation is found in early renal lesions including cysts and dysplasias Features of ccRCC are consistent with overexpression of HIF target genes and pathways Predictive Value Rini et al, BJU’06 Gad et al, Target Onc’07 VHL status and Clinical Outcome to VEGFtargeted Therapy •182 patients with metastatic RCC who received initial anti-VEGF therapy at CCF and UCSF between 2003 and 2006. •59 patients excluded: -Missing key data (n=3) -Pure non-clear cell histology (n=8) -Insufficient tissue for DNA extraction (n=12) -Unavailability of tissue (n=36) Clinical impact of VHL mutations in ccRCC Summary VHL mutations in ccRCC 60% HIF activation as a result of VHL loss is tightly correlated with tumor phenotype and may play a direct role in tumor growth HIF target gene activation is associated with the earliest stages of renal tumorigenesis and correlates with survival VHL mutation correlates with improved TTP in patients treated with inhibitors of the HIF target VEGF angiogenesis signaling pathway Association of FGFR2 Polymorphism with OS (P = 0.01) Selected genes associated with RFI Rini, ASCO’10 CSS in JCO’10, 28: 4501 ccRCC – localised disease (I-III) Pathways Signatures Genes associated with outcome (RFI) N. % Genes 732 Genes significantly associated with outcome (RFI, OS) 448 (69%) (unadjusted univariate analysis) Increased expression associated with better outcome 366 (82%) Covariate analysis Significant association with necrosis 503 Fuhrman grade 494 Pathologic Stage 482 T-size Rini, ASCO’10 CSS in JCO’10, 28: 4501 492 N-status ccRCC – localised disease (I-III) Genes selected for further analysis Total 72 Associated with RFI after covariate adjustment 29 Most significant before covariate adjustment By Pathway Cluster Analysis to identify genes from additional pathway 17 Member of VEGF/mTOR pathways 12 14 Rini, ASCO’10 CSS in JCO’10, 28: 4501 ccRCC – localised disease (I-III) Genes expressions and Recurrence Risk Expression Angiogenesis L Immune Response L IL6, IL8 H ECM/Cell adhesion H Cell cycle H I: Increased D: Decreased L: Low H: High Recurrence Rate I I I I I Rini, ASCO’10 CSS in JCO’10, 28: 4501 ccRCC – localised disease (I-III) Molecular Stratification Risk of Recurrence Low Intermediate High Increased Increased Angiogenesis Immune Response KDR1 IL6 EMCN IL8 Cell-mediated Cycle cytotoxic response CD8A Cell TPX2 CX3CL1 BUB1 Invasion CX CL10 MMP14 Rini, ASCO’10 CSS in JCO’10, 28: 4501 LAMB1 Select RNA gene expression data to clinical / pathologic variables enhances prediction of recurrence of localized RCC Renal Cell Carcinoma Angiogenesis and VEGF Inhibition Oudard S et al, Cancer Treat Rev 2012. Renal Cell Carcinoma Resistance to VEGF Inhibitors Casanovas O, et al. Cancer Cell. 2005;8:299-309 Rationale for combined Met and VEGFR inhibition • Met activation causes cells to proliferate and migrate • VEGFR activation initiates angiogenesis • Combining anti-tumour and anti-angiogenic activities may be a valid treatment strategy University of L’Aquila Department of Biotechnological and Applied Clinical Sciences Medical Oncology Corrado Ficorella Enrico Ricevuto Katia Cannita Gemma Bruera Eleonora Palluzzi Azzurra Irelli Valentina Cocciolone 65 Chow LQM, Eckhardt SG. J Clin Oncol. 2007;25(7):884-896 Eskens FALM, AACR; 2008. abst# LB-201 Spectrum and potency of TKIs versus VEGF receptors C.Sternberg. Sixth European International Kidney Cancer Association, May 6, 2011. Metastatic renal cell carcinoma MSKCC prognostic factors KPS <80 Time from diagnosis to treatment <12 months Hemogobin <lower limit of lab’s reference range LDH > 1.5x upper limit of lab’s reference range Corrected serum calcium > 10.0 mg/dl Metastatic renal cell carcinoma MSKCC Risk groups Favorable no poor prognostic factors Intermediate 1 or 2 poor prognostic factors Poor >2 poor prognostic factors Renal Cell Carcinoma VEGF Pathway G Korpanty et al, Journal of Oncology 2010 VEGF Inhibition Bevacizumab G Korpanty et al, Journal of Oncology 2010 Metastatic RCC Identification of biomarkers-Rationale ..may help determine patient prognosis ..identify patients most likely to benefit from specific treatments ..help monitor response to treatment ..guide clinicians in designing personalized treatment strategies Hypertension Biomarker of Efficacy with Sunitinib B Rini, J Natl Cancer Inst 2011; 103:763-773. Hypertension Biomarker of Efficacy with Sunitinib B Rini, J Natl Cancer Inst 2011; 103:763-773. Hypothyroidism in patients with renal cell carcinoma Schmidinger M, Cancer 2011. VHL genotype Prognostic relevance Choueiri et al, J Urol. 2008; Rini BI, et al. HIF-α protein expression and response to Sunitinib Patel et al, ASCO’08 RCC cell lines HIF-α protein expression Not all VHL mutations correlate with increased HIF-α expression Patel et al, ASCO’08 Metastatic ccRCC Heterogeneity PrognosticSignatureGenes Gerlinger M et al, N Engl J Med 2012;366:883-92 Mechanism of action of mTOR inhibitors Everolimus Temsirolimus Cen and Amato . OncoTargets and Therapy 2012:5 217–224 Serum LDH Biomarker with Temsirolimus Kaplan-Meier estimates for overall survival distribution by treatment group in the analyzed population (n 404). Kaplan-Meier estimates for overall survival distribution according to baseline lactate dehydrogenase (LDH) category. Kaplan-Meier estimates for overall survival distribution by treatment group and lactate dehydrogenase (LDH) levels, for (upper) normal level of LDH and (lower) Andrew J increased ArmstrongLDH. et al, J Clin Oncol 30:3402-3407. Metastatic ccRCC Heterogeneity Metastatic ccRCC Heterogeneity Gerlinger M et al, N Engl J Med 2012;366:883-92 Metastatic ccRCC Heterogeneity Gerlinger M et al, N Engl J Med 2012;366:883-92