What’s New in Trauma and
Critical Care
Chet A Morrison, MD, FACS, FCCM
Attending Trauma Surgeon
Lancaster General Hospital
Traumatic Injury: Still the Same Old Problem
Plus ca change….
• From 2000 to 2010, the US population increased by 9.7% and the number of trauma
deaths increased by 22.8%.
• Trauma deaths and death rates deceased in individuals younger than 25 years but
increased for those 25 years and older.
• The largest increases in trauma deaths were in individuals in their fifth and sixth
decades of life. Since 2000, the largest proportional increase (118%) in crude trauma
deaths occurred in 54-year-olds.
• Overall, in 2010, trauma was the leading cause of death in individuals 46 years and
younger. Trauma remains the leading cause of years of life lost
Rhee P et al Ann Surg 2014, 260(1): 13-21
Maybe This is Why
Gunshot Wounds: Unrelenting Violence
Ten Year Retrospective Look at GSW victims
6322 patients
Increase in number of gunshots per patients and body cavity wounds
Increase in Mortality
Total Inpatient cost 115 Million
75% unreimbursed
Livingston D et al J Trauma Acute Care Surg 2014 76(1): 2-11
Gunshot Wounds: Unrelenting Violence
Livingston D et al J Trauma Acute Care Surg 2014 76(1): 2-11
Hemostatic Resuscitation: The Prospective, Observational,
Multicenter, Major Trauma Transfusion (PROMMTT) Study
•Objective: To relate in-hospital mortality to early transfusion
of plasma and/or platelets and to time-varying plasma:red
blood cell (RBC) and platelet:RBC ratios.
•Prospective cohort study documenting the timing of
transfusions during active resuscitation and patient
outcomes. Data were analyzed using time dependent
proportional hazards models.
Holcomb JB Arch Surg. Published online October 15, 2012.
doi:10.1001/2013.jamasurg.387
Hemostatic Resuscitation: The Prospective, Observational,
Multicenter, Major Trauma Transfusion (PROMMTT) Study
•
Setting: Ten US level I trauma centers.
• Patients: Adult trauma patients surviving for 30 minutes after admission
who received a transfusion of at least 1 unit of RBCs within 6 hours of
admission (n=1245, the original study group) and at least 3 total units (of
RBCs, plasma, or platelets) within 24 hours (n=905, the analysis group).
• Main Outcome Measure: In-hospital mortality.
Holcomb JB Arch Surg. Published online October 15, 2012.
doi:10.1001/2013.jamasurg.387
Hemostatic Resuscitation: The Prospective, Observational,
Multicenter, Major Trauma Transfusion (PROMMTT) Study
• Results: Plasma:RBC and platelet:RBC ratios were not constant during
the first 24 hours (P.001 for both).
• In a multivariable time-dependent Cox model, increased ratios of
plasma:RBCs (adjusted hazard ratio=0.31; 95% CI, 0.16-0.58) and
platelets:RBCs (adjusted hazard ratio=0.55; 95% CI, 0.31-0.98) were
independently associated with decreased 6-hour mortality, when
hemorrhagic death predominated. In the first 6 hours, patients with ratios
less than 1:2 were 3 to 4 times more likely to die than patients with ratios
of 1:1 or higher.
• After 24 hours, plasma and platelet ratios were unassociated with
mortality, when competing risks from nonhemorrhagic causes prevailed.
Holcomb JB Arch Surg. Published online October 15, 2012.
doi:10.1001/2013.jamasurg.387
Hemostatic Resuscitation: The Prospective, Observational,
Multicenter, Major Trauma Transfusion (PROMMTT) Study
•Conclusions: Higher plasma and platelet ratios early in
resuscitation were associated with decreased mortality
in patients who received transfusions of at least 3 units
of blood products during the first 24 hours after admission.
Among survivors at 24 hours, the subsequent risk
of death by day 30 was not associated with either ratio
Non constant ratios make this a confusing question!
Holcomb JB Arch Surg. Published online October 15, 2012.
doi:10.1001/2013.jamasurg.387
Hemostatic Resuscitation: The Prospective, Observational,
Multicenter, Major Trauma Transfusion (PROMMTT) Study
Holcomb JB Arch Surg. Published online October 15, 2012.
doi:10.1001/2013.jamasurg.387
Hemostatic Resuscitation: The Prospective, Observational,
Multicenter, Major Trauma Transfusion (PROMMTT) Study
Holcomb JB Arch Surg. Published online October 15, 2012.
doi:10.1001/2013.jamasurg.387
Hemostatic Resuscitation: The Prospective, Observational,
Multicenter, Major Trauma Transfusion (PROMMTT) Study
PROPPR: Pragmatic Randomized Optimal Platelet and
Plasma Ratios
• ObjectiveThis trial is sponsored by the National Heart Lung and Blood Institute and
others. PROPPR is a multicenter, randomized trial which will compare different ratios
of blood products given to trauma patients who are predicted to require massive
transfusions (greater than 10 units of PRBCs within the first 24 hours). The patients
who have been predicted to require a massive transfusion will receive blood products
based on a 1:1:1 or 1:1:2 ratio of platelets, plasma and red blood cells. A total of 680
patients were enrolled into this study from 12 participating sites in the United States
and Canada. In addition to evaluating the patient outcomes based on ratio of
products, extensive lab analysis will be done to evaluate the influence of fluid
resuscitation on traumatic induced coagulopathy. The PROPPR trial will be conduced
under exception from informed consent. The trial began in August of 2012 and
concluded enrollment on December 2, 2013. Data analysis is currently underway.
http://clinicaltrials.gov/ct2/show/NCT01545232
A Paradigm Shift in Trauma Resuscitation: Evaluation of
Evolving Massive Transfusion Practices
• Objective To evaluate changes in the administration of fluids and blood products,
hypothesizing that a reduction in crystalloid volume and a reduced red blood cell
(RBC) to fresh frozen plasma (FFP) ratio over the last 7 years would correlate with
better resuscitation outcomes.
• Design Observational prospective cohort study.
• Setting Urban level I trauma center.
• Participants A total of 174 trauma patients receiving a massive transfusion (>10
units of RBCs in 24 hours) or requiring the activation of the institutional massive
transfusion protocol from February 2005 to June 2011.
Kutcher ME JAMA Surg. 2013;148(9):834-840.
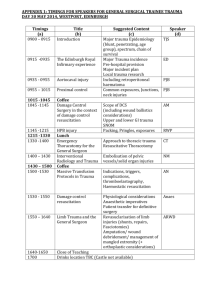
A Paradigm Shift in Trauma Resuscitation: Evaluation of Evolving
Massive Transfusion Practices
A, The mean combined numbers of
red blood cells (RBCs), fresh frozen
plasma (FFP), and pooled donor
platelets given within 24 hours of
admission, by year of study period,
are shown. The bars represent the
product breakdown (P = .03 by test
for trend).
TimeB, The median ratios of RBCs
to FFP transfused within 24 hours
of admission, by year of study
period (P = .20 by test for trend), are
shown.
C, The median volumes of
intravenous crystalloid
administered within 24
hours of admission, by year
of study period (P < .001 by
test for trend),
Kutcher ME JAMA Surg. 2013;148(9):834-840.
A Paradigm Shift in Trauma Resuscitation: Evaluation of Evolving
Massive Transfusion Practices
Kaplan-Meier 72-hour survival plots based on the red blood cell (RBC) to fresh frozen plasma (FFP) ratio
transfused within 24 hours of admission are shown for unadjusted survival (P < .001 determined by log-rank
test) (A) and adjusted for age, Injury Severity Score, Glasgow Coma Scale score, and base deficit at
admission using Cox proportional hazards regression (B).
Kutcher ME JAMA Surg. 2013;148(9):834-840.
TEG
•Originally used in Cardiopulmonary bypass
•May predict who will require transfusion
•Platelet mapping may be useful
•May decrease blood product use
•May predict pulmonary embolism risk
TEG
Cotton, B J Trauma Acute Care Surg. 2012 72(6):1470-1477
TXA
•Generic relatively cheap fibrinolysis inhibitor
•Demonstrated ‘efficacy’ in CRASH-2
•Easy to administer
•Issues with study
•No benefit 3 hrs after injury
TXA
Valle EJ J Trauma Acute Care Surg 2014 76(1): 1373
From: Declining Case Fatality Rates for Severe Sepsis: Good Data Bring Good News With Ambiguous
Implications
JAMA. 2014;311(13):1295-1297. doi:10.1001/jama.2014.2639
Figure Legend:
Potential Mechanisms of Decreasing Short-term Mortality Among Patients Across a Distribution of Illness Severity
Date of download: 7/16/2014
Copyright © 2014 American Medical
Association. All rights reserved.
Sepsis Care: The ProCESS Trial
Backgound
•In a single-center study published more than a decade ago
involving patients presenting to the emergency department
with severe sepsis and septic shock, mortality was markedly
lower among those who were treated according to a 6-hour
protocol of early goal-directed therapy (EGDT), in which
intravenous fluids, vasopressors, inotropes, and blood
transfusions were adjusted to reach central hemodynamic
targets, than among those receiving usual care.
Trial to determine whether these findings were generalizable
and whether all aspects of the protocol were necessary.
•
The ProCESS Investigators. N Engl J Med 2014;370:1683-1693
Sepsis Care: The ProCESS Trial
Method
•In 31 emergency departments in the United States, patients
with septic shock were randomly assigned to one of three
groups for 6 hours of resuscitation: protocol-based EGDT;
protocol-based standard therapy that did not require the
placement of a central venous catheter, administration of
inotropes, or blood transfusions; or usual care.
•The primary end point was 60-day in-hospital mortality;
sequentially evaluation whether protocol-based care (EGDT
and standard-therapy groups combined) was superior to
usual care and whether protocol-based EGDT was superior
to protocol-based standard therapy. Secondary outcomes
included longer-term mortality and the need for organ
support.
The ProCESS Investigators. N Engl J Med 2014;370:1683-1693
Sepsis Care: The ProCESS Trial
The ProCESS Investigators. N Engl J Med 2014;370:1683-1693
Sepsis Care: The ProCESS Trial
Results
•1341 patients, of whom 439 were randomly assigned to protocol-based
EGDT, 446 to protocol-based standard therapy, and 456 to usual care.
•
•Resuscitation strategies differed significantly with respect to the
monitoring of central venous pressure and oxygen and the use of
intravenous fluids, vasopressors, inotropes, and blood transfusions.
•By 60 days, there were 92 deaths in the protocol-based EGDT group
(21.0%), 81 in the protocol-based standard-therapy group (18.2%), and
86 in the usual-care group (18.9%) (relative risk with protocol-based
therapy vs. usual care, 1.04; 95% confidence interval [CI], 0.82 to 1.31;
P=0.83; relative risk with protocol-based EGDT vs. protocol-based
standard therapy, 1.15; 95% CI, 0.88 to 1.51; P=0.31). There were no
significant differences in 90-day mortality, 1-year mortality, or the need for
organ support.
The ProCESS Investigators. N Engl J Med 2014;370:1683-1693
Sepsis Care: The ProCESS Trial
Conclusion
•The investigators concluded that in a multicenter trial
conducted in the tertiary care setting, protocol-based
resuscitation of patients in whom septic shock was
diagnosed in the emergency department did not improve
outcomes. ProCESS ClinicalTrials.gov number,
NCT00510835.)
The ProCESS Investigators. N Engl J Med 2014;370:1683-1693
Sepsis Care: The ProCESS Trial
Outcomes.
RESULTS
The ProCESS Investigators. N Engl J Med 2014;370:16831693.
Sepsis Care: The ProCESS Trial
Cumulative Mortality.
Survival
The ProCESS Investigators. N Engl J Med
2014;370:1683-1693.
Other Recent Attempts at Sepsis Therapy
•HFOV
-Found to be ineffective at one trial; increased mortality
in another
• Statins
-Also not effective; no significant mortality decreases
•CytoFab
-CytoFab, a polyclonal anti–tumor necrosis factor
antibody (ClinicalTrials.gov number, NCT01145560)
Work halted, proposed trial canceled
Prone Positioning in Severe ARDS
Guerin et Al NEJM 2013 www.NEJM.org
Cognitive Impairment as a Long Term Problem
(Whisker Plot)
Cognitive Impairment as a Function of Delirium Duration
Nutritional Interventions for Critically Ill Patients, According to Data from Randomized,
EnteralControlledENteralTrials.
Feeding Summary
Casaer MP, Van den Berghe G. N Engl J Med 2014;370:1227-1236.
Comparison of Macronutrient Intake and Outcomes of Five Randomized,
Controlled Trials Evaluating Nutrition during Critical Illness
Trial of the Route of Early Nutritional Support in
Critically Ill Adults
Pragmatic, open, multicenter, parallel-group, randomized, controlled trial;
33 ICU in England participated
Patients who were at least 18 years of age were eligible if they were
expected to require nutritional support for at least 2 days, as determined
by a clinician within 36 hours after an unplanned ICU admission that was
expected to last at least 3 days.
Could be fed either way
Harvey SE et al. N Engl J Med 2014;371:1673-1684
Daily SOFA Score and Protein and Caloric Intake from Days 1 to 6.
Harvey SE et al. N Engl J Med 2014;371:1673-1684.
Daily SOFA Score and Protein and Caloric Intake from Days 1 to 6.
The target nutritional value of 25 kcal per kilogram per day was
NOT achieved for the majority of patients in the two study groups,
although caloric intake was similar in the two groups.
Harvey SE et al. N Engl J Med 2014;371:1673-1684.
Nutrition: The EDEN trial
• Designed to answer the question of trophic vs Full Feeds in ALI
• Randomized, open-label,multicenter trial conducted from January 2,
2008, through April 12, 2011.
• 1000 adults within 48 hours of developing acute lung injury requiring
mechanical ventilation whose physicians intended to start enteral
nutrition at 44 hospitals in the National Heart, Lung, and Blood Institute
ARDS Clinical Trials Network.
• Participants were randomized to receive either trophic or full enteral
feeding for the first 6 days. After day 6, the care of all patients who were
still receiving mechanical ventilation was managed according to the full
feeding protocol.
• Main Outcome Measures Ventilator-free days to study day 28.
Rice TW et al JAMA 2012;307:795-803
The EDEN trial: Results
• Initial trophic feeding did not increase the number of ventilator-free days
(14.9 [95% CI,13.9 to 15.8] vs 15.0 [95% CI, 14.1 to 15.9]; difference,
−0.1 [95% CI, −1.4 to 1.2];P=.89)
• 60-day mortality 23.2% vs 22.2% [95% P=.77) compared with full
feeding.
• No differences in infectious complications between the groups.
• Despite receiving more prokinetic agents, the full-feeding group
experienced more vomiting (2.2% vs 1.7% of patient feeding days;
P=.05), elevated gastric residual volumes (4.9% vs 2.2% of feeding
days; P.001), and constipation (3.1% vs 2.1%of feeding days; P=.003).
• Meanplasma glucose values and average hourly insulin administration
were both higher in the full-feeding group over the first 6 days.
Rice TW et al JAMA 2012;307:795-803
The EDEN trial: Results
The EDEN trial: Results
The EDEN trial: Results
Recommendations for Clinical Nutritional
Practice in the ICU and for Future Research.
Recommendations
Casaer MP, Van den Berghe G. N Engl J Med 2014;370:1227-1236.
ICP Monitoring: On Trial
• Intracranial-pressure monitoring is considered the standard of care for
severe traumatic brain injury. Efficacy of treatment based on monitoring
in improving the outcome has not been rigorously assessed.
• Multicenter, controlled trial in which 324 patients 13 years of age or
older randomly assigned to one of two specific protocols: guidelinesbased management in which a protocol for monitoring intraparenchymal
intracranial pressure was used or a protocol in which treatment was
based on imaging and clinical examination.
• The primary outcome was a composite of survival time,impaired
consciousness, and functional status at 3 months and 6 months and
neuropsychological status at 6 months;
Chesnut RA N Engl J Med 2012; 367:2471-2481
ICP Monitoring: On Trial
• There was no significant between-group difference in the primary outcome, a
composite measure based on percentile performance across 21 measures of
functional and cognitive status (score, 56 in the pressure-monitoring group vs.
53 in the imaging–clinical examination group; P = 0.49).
• Six-month mortality was 39% in the pressure-monitoring group and 41% in the
imaging–clinical examination group
• The median length of stay in the ICU was similar in the two groups (12 days in
the pressure-monitoring group and 9 days in the imaging–clinical examination
group; P = 0.25)
• The number of days of brain-specific treatments (e.g.administration of
hyperosmolar fluids and the use of hyperventilation) in the ICU was higher in the
imaging–clinical examination group than in the pressure-monitoring group (4.8
vs. 3.4, P = 0.002).
• The distribution of serious adverse events was similar in the two groups.
Chesnut RA N Engl J Med 2012; 367:2471-2481
ICP Monitoring: On Trial
Conclusions
•For patients with severe traumatic brain injury, care focused
on maintaining monitored intracranial pressure at 20 mm Hg
or less was not shown to be superior to care based on
imaging and clinical examination
•So wither ICP monitors?
•Still part of BTF recommendations
CDC New Definition VAE
•Multiple Stakeholders (none of them surgeons)
•Tiered System
•Variety of Clinical, radiologic and microbiologic criteria
•Concerns raised about under/overdiagnosis and ‘gaming
New CDC Definition of VAP
New CDC Definition of VAP
New CDC Definition of VAP
How We are Denied Money
Rib Fractures
Rib Fracture Fixation: Prospective Trial
•Traumatic flail chest injury
•A prospective randomized study compared operative fixation of fractured ribs in the flail
segment with current best practice mechanical ventilator management. In-hospital data, 3month follow-up review, spirometry and CT, and 6-month quality of life (Short Form-36)
questionnaire were collected.
•Patients in the operative fixation group had significantly shorter ICU stay (hours)
postrandomization (285 hours [range 191 to 319 hours] for the surgical group vs 359 hours
[range 270 to 581 hours] for the conservative group; p = 0.03) and lesser requirement for
noninvasive ventilation after extubation (3 hours [range 0 to 25 hours] in the surgical group
vs 50 hours [range 17 to 102 hours] in the conservative group; p = 0.01). No differences in
spirometry at 3 months or quality of life at 6 months were noted.
•Operative fixation of fractured ribs reduces ventilation requirement and intensive care stay
in a cohort of multitrauma patients with severe flail chest injury.
Marasco S J AM Coll Surg 216 (5) 2013
Rib Fracture Fixation: Prospective Trial
Marasco S J AM Coll Surg 216 (5) 2013
Rib Fracture Fixation: Prospective Trial
Marasco S J AM Coll Surg 216 (5) 2013
RIB Fracture Fixation: Cost Analysis
Costs of Procedures and Diagnoses Based on 2010 National Medicare Reimbursement
Procedure/diagnosis
ORIF
Flail chest
Wound infection
Sepsis
Bleeding
DVT
PE
Intubation<96 h
Intubation>96 h
Tracheostomy with intubation <96 h
Tracheostomy with intubation>96 h
VAP
Cost, $
3,961.16
484.02
4,894.69
5,627.73
4,894.69
3,281.29
5,390.61
11,279.68
26,123.17
11,661.63
26,505.12
3,679.84
Bhatnagar A - J Am Coll Surg - 01-AUG-2012; 215(2): 201-5
RIB Fracture Fixation: Cost Analysis
•
Mean cost effectiveness of open reduction and internal fixation for flail chest (ORIFFC) vs standard of care (SOC).
Bhatnagar A - J Am Coll Surg - 01-AUG-2012; 215(2): 201-5
The Future: Suspended Animation
Killing a Patient to
Save His Life
The Future: Suspended Animation
Emergency Preservation and Resuscitation for Cardiac
Arrest from Trauma (EPR-CAT)
• Systematic preclinical studies at the Safar Center for Resuscitation Research under
the direction of Drs. Safar, Sam Tisherman, and Pat Kochanek demonstrated the
feasibility of inducing profound hypothermia (50ºF or 10ºC) to provide a prolonged
period of cardiac arrest after exsanguinating hemorrhage.
• Dr. Tisherman is now leading the Emergency Preservation and Resuscitation for
Cardiac Arrest from Trauma (EPR-CAT) Study. This study is a feasibility and safety
study designed to see if hypothermia is beneficial in this setting. In EPR, body
temperature is lowered to about 50ºF (10ºC) by administering a large volume of cold
fluid through a cannula placed into the aorta. A heart-lung bypass machine would be
used to restore blood circulation and oxygenation as part of the resuscitation
process. The study will be conducted at the University of Pittsburgh and the
University of Maryland.
• Estimated Completion by Dec 2016
Under Fire: Gun Violence is not just an Urban Problem
• C. Morrison1, K. Bupp1, B. Gross1, K. Rittenhouse1, F. Rogers1 ; 1Lancaster General
Hospital, Trauma, Lancaster, PA, USA
•Introduction: Gun violence continues to be a source of
trauma patient morbidity and mortality annually in U.S.
communities. Recent research suggests increasing gunshot
violence severity in urban centers. We sought to
characterize gun violence in the combined suburban and
rural county of Lancaster, PA, to compare it to gun violence
results obtained in urban areas.
Under Fire: Gun Violence is not just an Urban Problem
Methods: In a Pennsylvania-verified, level II trauma center, treated gunshot wounds
(GSW) from January 2000 to December 2013 were queried from the trauma registry.
BB/pellet GSWs were excluded. Data collected included mortality, ISS, and number of
GSW per patient. Cost data was obtained for patients from 2004-2013, and costs
were calculated using cost-charge modifiers. A binary logistic regression was
performed to assess mortality over time. Linear trend tests assessed the change in
percent of patients with 3 or more GSWs, with ISS≥15 and ISS≥25 over the 14-year
study period. Significance was defined as p<0.05.
Under Fire: Gun Violence is not just an Urban Problem
Results: A total of 478 patients met inclusion criteria. Of these patients, 83.3%
sustained interpersonally-inflicted GSWs, while the remaining 16.7% sustained selfinflicted GSWs. The population was 62% white, 35% black, and 3% other.
Risk-adjusted mortality (for age, ISS) showed no significant change in mortality over
time (p=0.999).
Linear trend tests revealed no significant changes in percent of patients with 3 or
more GSWs (p=0.693), with ISS≥15 (p=0.546), or with ISS≥25 (p=0.342) over time.
No significant change in cost per case was found (p=0.380), however percent
reimbursement significantly increased (p=0.009).
Under Fire: Gun Violence is not just an Urban Problem
Conclusion: Even the fairly suburban and rural communities of
Lancaster County, PA are not sheltered from the problem of gun violence,
although the rate seems to be stable in a non-urban environment.
Despite advances in pre-hospital and hospital care, including damage
control techniques, the mortality from GSW has not changed.
Future efforts to improve the outcome for GSW Must primarily include
preventative efforts.
71
Summary Thoughts: Where are we at?
•Trauma Still qualifies as an unrelenting problem
•Liberal use of blood and factors in resuscitation
•We continue with a long list of sepsis interventions that are
of limited use
•There are opportunities to improve quality of life in the
Critical Patient
Thank You for Your Attention