Print Up to 5 copies
You print copies on the honor system; we trust that you will only make up to 5.
Need more than 5 copies? See other print options.
January 2, 2007
A Single Adulteration Limit for Cleaning
Validation in a Pharmaceutical Pilot-Plant
Environment
By Richard J. Forsyth,Alain Leblanc,Mark Voaden
A well run cleaning-validation program requires a significant amount of planning and
resources. Planning takes into account the size, configuration, and complexity of the
manufacturing equipment; the physical properties of the soils encountered, which directly
affect the cleaning procedure used; the detergent to clean the equipment; the type of swab
or rinse sampling to capture residue levels; the analytical test methods to determine
residue levels; the periodic monitoring of the system to ensure ongoing compliance; change
control to address new residues and equipment; appropriate documentation; and training
for personnel cleaning equipment and performing validation challenges. Required
resources include equipment downtime for the validation, raw materials for the formulations
tested, analytical instrumentation for analysis, detergents for cleaning, solvents for testing,
and personnel to perform the validation.
The entire cleaning-validation program and its execution depend directly on the acceptable
residue limit (ARL) for the formulation residue. The active pharmaceutical ingredient (API)
residue is monitored because it is the most phamacologically active component of the
formulation. The ARL established for a program must be scientifically justified on the basis
of the needs and capabilities of the manufacturing facility. In its Guide to Inspection of
Validation of Cleaning Processes (1), the US Food and Drug Administration stated that
residue limits should be logical, practical, achievable, and verifiable. The agency did not
intend to set acceptance limits for validating cleaning processes. One of the examples cited
as a possible residue limit used in industry, however, was 10 ppm of carryover into the
subsequent batch manufactured.
The purpose of cleaning validation is to prevent the cross-contamination of a drug
formulation. The primary concerns of cross-contamination are an evaluation of the
therapeutic-dose carryover or the toxicity of the potential contaminant. Any contaminant is
undesirable, but one with a pharmacologic or toxicological effect is far more serious. The
Food, Drug, and Cosmetic Act (2) states: "A drug ... shall be deemed to be adulterated if it
consists in whole or in part of any filthy, putrid, or decomposed substance," that is,
something that will cause an adverse pharmacological effect. This definition supports the
pharmacological and toxicological concerns.
If, however, the amount of a residue is below the level at which it would have an
unintended, adverse health effect, what is the allowable level from an adulteration
standpoint? Should a health-based limit be the only limit for equipment cleaning? Should
the analytical-method detection limit be the standard (3)? Or, if an intermediate adulteration
limit exists, what rationale determines that level? In the past, analytical methodology had
limited sensitivity, making health-based and adulteration-based contaminations essentially
equivalent. The increased sensitivity of analytical methodology seemingly has created a
contradictory situation. Modern analytical detection limits are far lower than the
pharmacological levels of drugs, thus creating a divergence between the previously
equivalent health-based and adulteration definitions.
A logical residue limit would be one that demonstrates no pharmacological or toxicological
effect, without regard to analytical sensitivity. This would indicate that residue levels can be
as high or as low as the health-based limit will allow. This approach, however, would allow
equipment to be visually dirty for relatively safe residues, which indicates an inadequate
cleaning procedure. A logical residue limit also should leave the equipment visually clean.
Setting residue limits any lower than the health-based and visible levels does not appear to
be necessary or logical and adds no additional value to the cleaning process.
Several cleaning-validation programs use the dual health-based–adulteration-based
criterion (4–6). Evaluations based on toxicity, tablet weight, number of doses administered,
swab recovery, swab area or equipment surface area, and batch size determined the ARLs
from both an adulteration-based and health-based perspective. The lower of the two limits
was the designated ARL for the formulation and the equipment.
The cleaning-validation program in our pilot-plant facility calculated ARLs for both the
health-based and adulteration-based criteria and used the lower of the two (7). The
dynamic nature of the pilot plant and the drug-development process necessitated regular
re-evaluation of the ARL for each API. Each API required a health-based evaluation, but
the majority of development compounds had such low toxicity that their adulteration limits
were lower. A proposed alternative to the constant re-evaluation of adulteration limits was
to use a constant adulteration limit of 100 μg/25 cm2 swab or 4 μg/cm2 . This technique
would streamline the cleaning process and minimize potential errors without compromising
quality or safety.
Health-based risk assessment
To implement an adulteration limit, it must be lower than the associated health-based ARL.
The adulteration limit would be lower at the level at which compounds are not likely to be
potent, highly toxic, or carcinogenic. A corresponding allowable daily intake (ADI) for this
category of material is 100 μg/day (0.1 mg/day) (8).
The calculation for the health-based ARL with an ADI of 0.1 mg/day includes:
in which ADI is the allowable daily intake for the compound, SSA is the shared productcontact surface areas of the manufacturing equipment train, and recovery is the percentage
of spiked material recovered for assay.
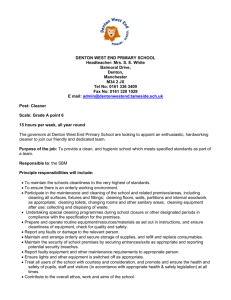
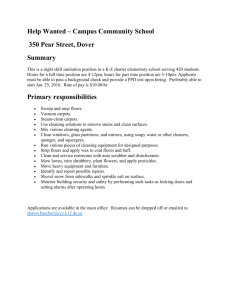
Table I shows the health-based ARLs with associated
parameters for an ADI of 0.1 mg/day, tablet weight from
0.1–1.5 g and maximum daily dose from 1–10 tablets.
The number of tablets per batch ranged from 266–10,000
(small) to 3600–160,000 (medium) to 46,666–1,000,000
(large), based on batch sizes of 0.4–1 kg (small), 5.4–16
kg (medium), and 70–100 kg (large), respectively. It was
assumed that the next batch was manufactured in
equipment with the same SSA.
Table I: Calculated health-based acceptable
residue limit (μg/swab).
The shaded portions of the small, medium, and large batch ranges in Table I fell below the
proposed limit of 100 μg/swab (4 μg/cm2 ). The low end of each range assumed the
smallest batch size, the largest tablet weight (1500 mg), and the highest number of tablets
dosed (10).
In the pilot plants, about 5% of manufactured batches fell below the 100 μg/swab (4 μg/cm2
) limit. The batches that fell below the 4 μg/cm2 limit were typically for clinical studies with
large tablet sizes (>1000 mg), multiple-tablet doses (>6 tablets/dose) or small batch sizes
(<500 g). Small batch sizes generally are for first-in-man studies or preclinical and Phase I
studies. These clinical-trial programs are dosed on small populations to establish dose
levels.
The risk of falling below the 4 μg/cm2 limit for compounds with ADIs >100 μg/day was
small, based on the site data. Also, of the 1225 swab samples taken in support of cleaning
validation, none failed the ARL for the compound tested, greater than 98% of the swabs
were below 1 μg/cm2 , and more than 99.5% were below 4 μg/cm2 , further reducing
potential risk.
Finally, a continuing program for monitoring cleaning effectiveness using visible residue
limits (VRL) was conducted. Of the manufactured batches that fell below the 100 μg/swab
(4 μg/cm2 ) limit, the highest VRL was 1.23 μg/cm2 , which is well below the health-based
limit. Therefore, for compounds with ADIs >100 μg/day, it is extremely unlikely that the
adulteration limit selected will be greater than the health-based limit.
Adulteration-based calculation
The adulteration limit was used when it was lower than the health-based limit. For
development compounds in the pilot plant (7), the adulteration limit originally was
calculated using the following equation:
in which UAL was the upper acceptance limit; SSA the shared surface area, MBS the
minimum batch size for the equipment train, and recovery the fraction of spiked material
recovered for assay. The UAL of 10 μg/g (10 ppm) cited by FDA (1) was used in various
cleaning-validation programs (3, 9, 10). The SSA was the combined product-contact
surface areas of the manufacturing equipment train. The MBS provided the most
conservative limit because any residue would be most concentrated in the subsequent
batch. The swab area of 25 cm2 was used widely (3, 7, 11, 12) in industry.
Calculation of an allowable adulteration level was a logical cleaning limit for a pilot plant but
in the long term proved to be impractical. The number of factors that went into the pilotplant production schedule, the drug-development formulations, and the residue
determination made an adulteration assessment a constantly changing number.
Pilot-plant issues
Number of pilot-plant programs. The pilot plant manufactured varied formulations of
numerous compounds. The programs in the pilot plant increased with new compounds and
decreased as programs ceased development or were transferred to commercial
manufacturing. Schedulers, formulators, equipment cleaners, analytical chemists, and
quality personnel were involved. The number of programs and personnel along with the
associated ARL calculations, documentation, and communication made it difficult to
maintain a consistent, compliant program.
Number of new compounds. The number of new compounds entering the pilot plant was
significantly greater than the number of new compounds entering a commercial
manufacturing facility. These new programs had to be included in the overall cleaningassessment program. Validating a new compound required significant analytical method
development and validation. In addition, the small, early-phase manufacturing equipment
was in great demand, and extended downtime for cleaning validation support was
problematic.
Subsequent product. The manufacturing schedule in the pilot plant was variable.
Equipment was scheduled for use several weeks in advance, but other programs
sometimes took priority. Even knowing the subsequent product was no guarantee that a
particular formulation was the same as the previous one manufactured for the product.
Calculating an ARL based on the subsequent product manufactured in the equipment was
problematic.
Current equipment train versus subsequent equipment train. The equipment train was
the order in which equipment was used to manufacture a formulation. Blending,
granulation, roller compaction, drying, and tablet pressing were examples of unit operations
that together manufactured a clinical formulation. The ARL calculation for the equipment
train assumed that the same train was used for the subsequent product. This almost never
was the case in a pilot plant, which made the value of the ARL limited. An alternative ARL
calculation considered each individual piece of equipment without regard to the
manufacturing train. This type of ARL consideration became exceedingly cumbersome
without adding increased value to the ARL process.
Formulation-development issues
Formulation changes. The formulation for each research compound evolved during
development. A dry-filled capsule for a Phase I compound became a film-coated tablet in
Phase II. Refinements in formulation composition also were common. Excipient levels
changed to optimize the physical properties of the formulation. Formulation changes also
resulted from scale-up issues. Formulation modifications often changed the ARL for the
subject compound.
Establishing effective dose. The effective dose of an API was unknown when clinical
trials began. Dose levels could cover several orders of magnitude for early clinical trials.
The results of the ongoing trials determined the dose for the next phase of testing and the
eventual market-dose level. Formulations of early-development compounds had different
dose levels and batch sizes. The amount of API in a formulation had a direct effect on the
ability to clean the equipment. Therefore, cleaning could be assessed after every batch,
based on the API factors involved.
Scale-up. Each clinical trial required a larger batch size than the previous trial, which
necessitated equipment with a larger capacity. The physical interactions of the formulation
components for larger batches often resulted in changes to the formulation or required a
different type of manufacturing equipment. Each time the batch size or the equipment train
changed, the ARL was reassessed.
Adulteration-determination issues
Effect of small batch size or unit operations. In the pilot-plant environment, initial batch
sizes were very small, often on the order of several hundred grams. Calculating an ARL
based on the smallest batch size reduced the cleaning limit to a low level and potentially
affected a Phase II compound manufactured just before a Phase I compound. Similarly,
calculating an ARL for each individual piece of equipment in the manufacturing train
resulted in very low cleaning limits for small surface-area equipment.
Rather than calculate the ARL for every clinical batch manufactured, certain assumptions
were made to generalize the equation. The most conservative assumption used the
minimum batch size for the equipment. This assumption made the generalized ARL lower
than a specifically calculated ARL under most circumstances.
The adulteration limit calculation was the following:
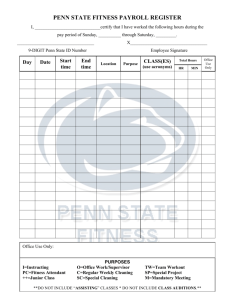
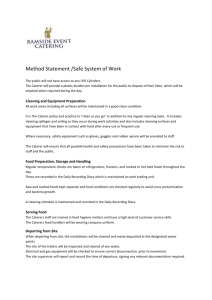
Table II shows the product-contact surface areas for a
typical equipment train for Phase I (small), Phase II
(medium), and Phase III (large) formulations. Table III
shows the range of ARLs for a constant UAL of 10 μg/g, a
swab area of 25 cm2 , and a recovery of 100%. The
calculated adulteration limit varied from 17 to 216
μg/swab for the same compound, depending on the
manufacturing train. The adulteration limit varied from
batch to batch for the same compound, making
reassessment a routine occurrence.
Table II: Product-contact surface areas (SSA)
for typical equipment trains by phase.
The variable adulteration limit also brought into question
the value of the calculated limit to the overall cleaning
Table II: Product-contact surface areas (SSA)
for typical equipment trains by phase.
program. For small batches, the limit was far below the 10
μg/g level. For larger batches, the calculated adulteration limit was greater than the visually
clean level, thus making it obsolete.
Analytical limits. High-performance liquid chromatography and total organic carbon
methods were used most frequently. Each analytical test method had very low detection
limits, either in the ppm or ppb range. Analytical limits were lower than the calculated
health-based and adulteration-based limits. On the basis of instrumental capabilities, the
use of analytical limits was considered for the adulteration limit.
Using 0.1% of the subsequent API as the adulteration limit was not appropriate. The 0.1%
limit, determined during release testing, was intended for qualifying impurities that were
associated with the manufacturing process or related compounds, and not for extraneous
impurities caused by cross-contamination. Acceptance limits should reflect the capability of
the cleaning processes (13).
Visible residue limits
The determination and use of VRLs demonstrated that the vast majority of formulations and
APIs had VRLs lower than 100 μg/25 cm2 swab (4 μg/cm2 ) (14, 15). Of the 54 formulations
evaluated to date, all were well below 100 μg/25 cm2 swab. Of the 102 APIs, excipients,
and detergents evaluated, only five excipients and one API had VRLs greater than 100
μg/25 cm2 swab. Limited applications of VRLs have saved resources without sacrificing
quality (16, 17).
Swab area. An often cited adulteration limit was 10 ppm or 100 μg/swab, using a swab
area of 25 cm2 for cleaning validation. This amount was a feasible limit. The swab area was
not as important as the scientifically justified limit but was a practical compromise to obtain
a representative residue sample against the occasional need to swab smaller pieces of
equipment.
Conclusion
The factors that affect the adulteration calculation made it an impractical situation for a
pilot-plant application. A constantly changing adulteration limit caused documentation
problems and made compliance difficult to enact and enforce.
An alternative single adulteration limit was proposed for compounds with ADIs >100
μg/day. An adulteration limit of 100 μg/25 cm2 swab (4 μg/cm2 ) was satisfactory as long as
the equipment was visually clean. This limit ensured that there were no toxicity crosscontamination problems and that the equipment was visually clean. A single, scientifically
determined adulteration limit is logical, practical, achievable, and verifiable, making it a
justifiable adulteration limit for a pilot-plant facility.
Richard J. Forsyth* is an associate director in global clinical GMP quality with Merck &
Co., Inc., WP53C-307, West Point, PA 19486, tel. 215.652.7462, fax 215.652.7106,
richard_forsyth@merck.com [richard_forsyth@merck.com]
Alain Leblanc is a facility manager at Merck Frosst Canada's Center for Therapeutic
Research. Mark Voaden is head of service for validation and compliance for facilities with
Merck, Sharp & Dohme in the United Kingdom.
*To whom all correspondence should be addressed.
Submitted: June 20, 2006. Accepted: Aug. 24, 2006.
Keywords: adulteration limit, cleaning validation, compliance, pilot plant.
References
1. US Food and Drug Administration, Guide to Inspection of Validation of Cleaning
Processes, (Rockville, MD, Office of Regulatory Affairs, 1993).
2. Food, Drug and Cosmetics Act, Chapter V, Section 501(a)(1), 1938.
3. FDA, CDER Human Drug CGMP Notes, 9 (2) (Rockville, MD, Division of Manufacturing
and Product Quality, Office of Compliance, Center for Drug Evaluation and Research,
2001).
4. G.L. Fourman and M.V. Mullen, "Determining Cleaning Validation Acceptance Limits for
Pharmaceutical Manufacturing Operations," Pharm. Technol. 17 (4), 54–60 (1993).
5. A.O. Zeller, "Cleaning Validation and Residue Limits: A Contribution to Current
Discussions," Pharm. Technol. 17 (10), 70–80 (1993).
6. K.M. Jenkins and A.J. Vanderwielen, "Cleaning Validation: An Overall Perspective,"
Pharm. Technol. 18 (4), 60–73 (1994).
7. R.J. Forsyth and D. Haynes, "Cleaning Validation in a Pharmaceutical Research
Facility," Pharm. Technol. 22 (9), 104–112 (1998).
8. D.G. Dolan et al., "Application of the Threshold of Toxicological Concern Concept to
Pharmaceutical Manufacturing Operations," Regul. Toxicol. Pharmacol. 43 (3), 1–9 (2005).
9. R. Baffi et al., "A Total Organic Carbon Analysis Method for Validating Cleaning Between
Products in Biopharmaceutical Manufacturing," J. Parenter. Sci. Technol. 45 (1), 13–19
(1991).
10. R.J. Romanach et al., "Combining Efforts to Clean Equipment in Active Pharmaceutical
Ingredient Facilities," Pharm. Technol. 23 (1), 46–58 (1999).
11. M.A. Stege et al., "Total Organic Carbon Analysis of Swab Samples for the Cleaning
Validation of Bioprocess Fermentation Equipment," BioPharm 9 (4), 42–45 (1996).
12. D.A. LeBlanc, "Establishing Scientifically Justified Acceptance Criteria for Cleaning
Validation of Finished Drug Products," Pharm. Technol. 22 (10), 136–148 (1998).
13. FDA, CDER Human Drug CGMP Notes, 6 (2), 5–6 (Rockville, MD, Division of
Manufacturing and Product Quality, Office of Compliance, Center for Drug Evaluation and
Research, 1998).
14. R.J. Forsyth, V. Van Nostrand, and G. Martin, "Visible Residue Limit for Cleaning
Validation and its Potential Application in a Pharmaceutical Research Facility," Pharm.
Technol. 28 (10), 58–72 (2004).
15. R.J. Forsyth and V. Van Nostrand, "Application of Visible Residue Limit for Cleaning
Validation in a Pharmaceutical Manufacturing Facility," Pharm. Technol. 29 (10), 152–161
(2005).
16. R.J. Forsyth and V. Van Nostrand, "Using Visible Residue Limits for Introducing New
Compounds into a Pharmaceutical Research Facility," Pharm. Technol. 29 (4), 134–140
(2005).
17. R.J. Forsyth, J. Hartman, and V. Van Nostrand, "Risk-Management Assessment of
Visible-Residue Limits in Cleaning Validation," Pharm. Technol. 30 (9), 104–114 (2006).
Table I: Calculated health-based acceptable residue limit (μg/swab).
Table II: Product-contact surface areas (SSA) for typical equipment trains by phase.
Table II: Product-contact surface areas (SSA) for typical equipment trains by phase.
2007 Advanstar Communications Inc.. Permission granted for up to 5 copies. All rights reserved.
You may forward this article or get additional permissions by typing
http://license.icopyright.net/3.7458?icx_id=397397 into any web browser. Advanstar Communications
Inc. and Pharmaceutical Technology logos are registered trademarks of Advanstar Communications Inc. The iCopyright
logo is a registered trademark of iCopyright, Inc.