Telligen Cardiac Learning Network
Anna Astalas, MPA, RN, CPHQ
Illinois Cardiac Primary Point of Contact
1
This material was prepared by Telligen, Medicare Quality Innovation Network Quality
Improvement Organization, under contract with the Centers for Medicare & Medicaid
Services (CMS), an agency of the U.S. Department of Health and Human Services. The
contents presented do not necessarily reflect CMS policy. 11SOW-IL-B1-5/2015-11035
Telligen QIN QIO
•
2
Telligen: Quality Innovation Network-Quality Improvement Organization
(QIN-QIO) for Colorado, Illinois and Iowa
Telligen QIN QIO
• Quality Improvement Organization in Illinois
– We are contracted with Medicare to provide technical assistance,
facilitation, and support services to IL healthcare providers AT NO COST
– We are inviting 100 provider/practices and 200 HHAs to participate in a
Cardiac Learning and Action Network
– We will focus on (and follow) the four Million Hearts® ABCS measures:
3
Aspirin therapy, when appropriate (PQRS #204)
Blood pressure control (PQRS #236)
Cholesterol management (PQRS #316)
Smoking assessment and cessation counseling (PQRS #226)
Promoting Disease Management and Prevention
of Cardiac Disease
• Partners:
– Beneficiaries and Families, Partners and
Stakeholders, Providers, Practitioners,
Clinics, Home Health Agencies
• Our shared goals:
– Align with Million Hearts Initiative to prevent
one million heart attacks and strokes
– Improve ABCS
– Reduce health disparities
4
Benefits of Participating with Telligen
• How Will Telligen Help?
–
–
–
–
–
–
–
–
–
5
QI process/plan to improve measures
Local/national benchmark cardiac reports for comparison
Assistance with analyzing data trends for QI
Staff and patient resources, tools and toolkits
Educational events (monthly recorded webinars, live conference, etc.)
Sharing best practices and network among healthcare peers
Current Medicare rules and regulations
Improve Star ratings
Help with workflow improvement, engaging patients, team-based care and overall
patient outcomes!
Benefits (Continued)
• Assistance With Other Tasks
–
–
–
–
–
Diabetes
EHR/MU measures
PQRS measures
Value-Based Modifier
Immunizations
If interested, contact:
anna.astalas@area-d.hcqis.org
(630)928-5832
6
A M.A.P. for improving blood pressure
Donna Daniel, PhD
Director, Improving Health Outcomes
American Medical Association
Mike Rakotz, MD
Director, Chronic Disease Prevention
American Medical Association
IMPROVING HEALTH OUTCOMES: BLOOD PRESSURE
Telligen Cardiac LAN
May 26, 2015
Disclosures
Donna Daniel, PhD
No disclosures
Michael Rakotz, MD
No disclosures
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
8
What we hope to accomplish today
• Provide background on the AMA-Johns Hopkins collaboration
• Summarize a program to engage your leaders and staff in improvement
• Describe a framework for improving blood pressure control
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
9
Prototyping new tools and resources
Partner: Johns Hopkins Medicine
•
Armstrong Institute for Patient Safety and Quality
(Dr. Peter Pronovost)
•
Center to Eliminate Cardiovascular Health Disparities
(Dr. Lisa Cooper)
Advisory group of national experts in HTN care
Patient and family advisory group
10 Diverse Practice Sites
•
•
From solo practitioner to multispecialty practice with 14 physicians
Diverse patient panels ranging from 95% African-American to 87%
Latino, 60% Medicaid to 55% Medicare
Feedback on a framework, tools and resources and curriculum
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
10
Patient involvement in program design
•
•
Advisory group charged with reviewing tools,
advising on how best to meet patient and family
needs
Suggest new ideas, help prioritize tool
development
Emphasis on improving health equity
• Tapped into expertise of Johns Hopkins Center to Eliminate Cardiovascular Health
Disparities
• BP control performance reporting stratified by race/ethnicity
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
11
The M.A.P. framework
Measure blood pressure accurately
Act rapidly to manage uncontrolled hypertension
Partner with patients, families and communities
to promote self-management
Actionable data
Evidence-based tools
Adaptive change
Monthly reports on blood
pressure control rate, stratified
by key patient demographics
A toolkit for implementing the M.A.P.
framework: checklists, fact sheets,
posters, audit tools, patient engagement
tools, etc.
A simple model for promoting
teamwork, communication and a
culture of quality improvement
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
12
Applying evidence to improve
blood pressure control
Mike Rakotz, MD
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
13
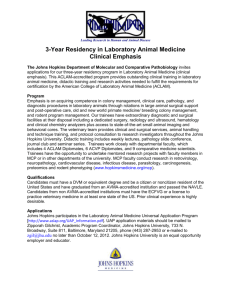
Why controlling BP is important
Ischemic Heart Disease
Ischemic Stroke
Ischemic Heart
Disease and
Stroke Mortality
due to elevated
blood pressure
1 Million Adults,
61 Prospective Studies
Lewington S. et al. Age-specific relevance of usual blood
pressure to vascular mortality The Lancet, 2002
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
14
Why controlling BP is important
• Morbidity and mortality due to cardiovascular diseases are directly
related to BP.
• In people with hypertension and elevated BP, when BP is lowered
there is less vascular damage to organs (kidneys, heart, eyes, brain).
• Treatment of high blood pressure lowers risk of cardiovascular disease
and death.
Kaplan and Victor Kaplan’s Clinical
Hypertension. 111th Edition. 2015
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
15
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
16
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
17
Why measuring blood pressure accurately is important
• Each 1 mm Hg rise in blood pressure above normal
reduces life expectancy by one year on average
• Even small changes in BP have significant impact on the
health of patients
How does this impact clinicians in practice?
Summary report: National High Blood Pressure Education Program (NHBPEP)/NHLBI and AHA working
meeting on blood pressure measurement. Bethesda: National Institutes of Health; 2002. Available at:
http://www.nhlbi.nih.gov/health/prof/heart/hbp/bpmeasu.pdf
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
Braunwald Hypertension 2014
18
Why measuring blood pressure accurately is important
We need accurate, reliable blood pressures to make
strong clinical decisions.
Braunwald Hypertension 2014
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
Braunwald Hypertension 2014
19
What are the most accurate techniques
for BP measurement?
• 24-Hour Ambulatory Blood Pressure Monitoring (ABPM)
• Self-Measured Blood Pressure (SMBP) monitoring
(home blood pressure monitoring)
– Occurs outside of clinical setting, eliminating white
coat effect
– Allows for multiple readings over time
– Provides asleep blood pressures (in the case of
ABPM)
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
20
The most accurate techniques for BP measurement
Until these options are more available, we must effectively
screen for and confirm elevated BPs in our practices or
health centers
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
21
How many errors in BP
measurement do you see?
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
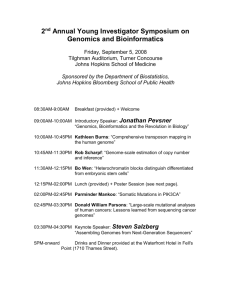
22
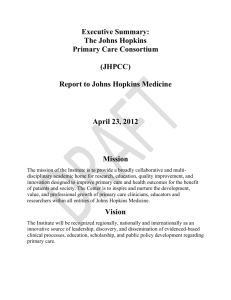
How many errors in BP
measurement do you see?
1.
2.
3.
4.
5.
6.
7.
Back is not supported
Arm is not supported near heart level
Cuff is over sweatshirt
Legs are crossed
Legs are not both flat on the stool
She is talking
She is listening
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
23
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
24
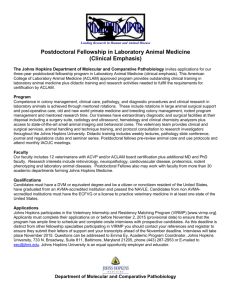
Correct patient position for BP measurement
For screening BP measurement
•
Automated validated device
•
Sitting in a chair with back and arm supported (1)
•
Legs uncrossed, feet on the ground or a stool (2)
•
Cuff over a bare arm (3)
•
Correct Cuff Size
•
No talking or texting
If the screening BP is > 140/90 mm Hg, obtain confirmatory BP
measurements
For confirmatory BP measurements, same as above, plus
•
Ensure patient has an empty bladder
•
Rest for at least 5 minutes
•
Obtain the average of at least 3 measurements
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
25
Why use office BP measurement?
•
Opportunity to obtain BPs
•
Technology has improved measurement reliability
(validated, automated machines less human error)
•
Protocols improve standardization, reduce variability and errors, and can
improve workflow efficiency
•
Obtaining confirmatory measurements increases diagnostic accuracy and
reduces misclassification
•
By reducing errors and increasing reliability of BP measurement, clinicians are
less likely to hesitate when initiating or escalating treatment (clinical inertia)
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
26
Measure accurately checklist
When screening patients for high blood pressure:
Use a validated, automated device to measure BP
Use the correct cuff size on a bare arm
Ensure patient is positioned correctly
If BP is ≥140/90 mm Hg, obtain a confirmatory measurement:
Repeat screening steps above
Ensure patient has an empty bladder
Ensure patient has rested quietly for at least five minutes
Obtain the average of at least three BP measurements
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
27
How single-pill combination therapy can help
Single-pill combination therapy gets patients to goal more quickly by
•
•
Expediting escalation of therapy
Using fewer prescriptions
Non-adherence to medications, another barrier to achieving blood
pressure control, is reduced with single-pill combinations
•
Using single-pill combination therapy improves adherence rates 26%
compared to non-combination medications
Bangalore et al The American Journal of Medicine (2007) 120, 713719
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
Handler. J Clin Hypertens.
Most common factors contributing
uncontrolled hypertension
1. Miss opportunities to treat a patient with a BP > 140/90
• Fail to initiate or escalate therapy during an office visit
• Fail to stress frequent follow up until BP is controlled
2. Non-adherence to treatment plan
• Usually due to not taking medications as instructed
CLINICAL INERTIA
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
29
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
30
Factors leading to clinical inertia
CLINICIAN
•
Failure to initiate treatment
•
Failure to titrate to goal
•
Failure to recommend follow-up
•
Failure to set clear goals
•
Underestimating patient needs
•
Failure to identify and manage comorbid conditions
•
Not enough time
•
Insufficient focus or emphasis on goal attainment
•
Reactive rather than proactive
Adapted from Milani RC et al J Am Coll
Cardiol. 2013; 62: 2185-2187
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
31
Factors leading to clinical inertia
PATIENT
•
•
•
•
•
•
•
Medication side effects
Failure to take meds
Too many medications
Cost of medications
Denial of disease
Forgetfulness
Perception of low susceptibility
•
•
•
•
•
Absence of symptoms
Poor communication
Mistrust of clinician
Mental illness
Low health literacy
Adapted from Milani RC et al J Am Coll
Cardiol. 2013; 62: 2185-2187
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
32
Factors leading to clinical inertia
HEALTH SYSTEM
•
•
•
•
•
•
•
Lack of clinical guideline
Lack of care coordination
No visit planning
Lack of decision support
Poor communication
between office staff
No disease registry
No active outreach
Adapted from Milani RC et al J Am Coll
Cardiol. 2013; 62: 2185-2187
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
33
Why standardized treatment protocols are important
In hypertensive patients with systolic BP >150 mm Hg,
treatment delays are associated with an increased risk
of acute cardiovascular events or death
• Delays in medication intensification >6 weeks
• Delays in follow-up appointments >10 weeks after
medication intensification
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
34
Act rapidly checklist
If patient has BP ≥ 140/90 mm Hg confirmed:
Use an evidence-based protocol to guide treatment
Re-assess patient every 2–4 weeks until BP is controlled
When possible, prescribe single-pill combination therapy
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
35
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
36
Use evidence-based communication strategies
• Engage patients to improve compliance with therapy
• When clinicians talk less and listen more, they can gain relevant
information, including details that can help us determine a preferred
treatment approach
• When patients use this kind of communication, they are more
engaged/committed, and as a result, are more likely to adhere
• Using these communication techniques does not lengthen visits (it
actually shortens them), especially if all practice staff are using them
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
37
Use evidence-based communication strategies
STRATEGY
Begin with open-ended questions about adherence, including
recent medication use
Explore reasons for possible non-adherence
Elicit patient views on options and priorities to customize a
care plan for each patient
Remain non-judgmental at all times
Use teach-back to ensure understanding of the care plan
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
38
Why self-measured BP (SMBP) is clinically useful
SMBP better predicts CV morbidity and
mortality than office BPs
• Reduces variability and provides
more reliable BP measurement
• Provides better assessment of
hypertension control
• Empowers patients to self
manage their HTN
• May improves medication
adherence
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
Slide from the American Society of HTN 2014 Review Course
39
Lifestyle changes for hypertensive patients
•
Healthy diet, such as DASH diet
•
Reduced sodium intake
•
Weight loss
•
Aerobic exercise
•
Moderate alcohol consumption
•
No smoking
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
Taking a pill to lower BP
40
Impact of lifestyle changes for improving blood
pressure in patients with HTN
LIFESTYLE CHANGE
CAN LOWER SBP/DBP UP TO:
DASH diet, compared with typical American diet
11.6/5.3 mm Hg
Reduce sodium intake by average of 1150 mg/d
4/2 mm Hg
Average weight loss of 11 lbs
4.4/3.6 mm Hg
40 minutes of moderate intensity aerobic
physical activity, 3–4 times a week
5/4 mm Hg
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
41
Partner with patients, families and
communities checklist
To empower patients to control their blood pressure:
Engage patients using evidence-based communication
strategies
Help patients accurately self-measure BP
Direct patients and families to resources that support
medication adherence and healthy lifestyles
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
42
AMA-JHM IHO: BP program tools
Includes a set of tools to support each checklist
“Measure accurately assessment” tool
“Act rapidly assessment” tool
“Partner with patients, families and communities assessment” tool
Posters, flyers, fact sheets, audit tools and “self-measured blood
pressure” program guide
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
43
Adaptive change in ambulatory
practice program (ACAP)
• Supports culture change necessary to implement and sustain the
M.A.P. checklists
• Engages all clinical and non-clinical staff to take ownership in patient
care
• Taps into the wisdom of all staff members to drive improvement efforts
• Improves teamwork and teamwork for better and consistent patient
care
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
44
Thank you
Any questions?
© 2015 American Medical Association and The Johns Hopkins University. All rights reserved .
Announcements
• Wednesday, May 27 at 12:00 PM EDT – “A Team Approach:
Integrating tobacco dependence treatment into routine clinical
practice”, Dr. Chad Morris, PhD
– Register: https://cc.readytalk.com/r/3pf7g6vgxjxi&eom
• Friday, May 29 at 8:30 AM-2:00 PM CST - Go Red for Women
Community Expo at the Great Hall, Union Station, 500 West Jackson,
Chicago - FREE
– Register: Contact the AHA at 312-476-6679 or
GoRedChicago@heart.org
• Tuesday, June 23 at 11:30A - Home Health Cardiac Kick-off: Get
Started with Cardiac Data!
46
Conclusion
• Would you like Telligen to provide additional information
and webinars (or podcasts) on the M.A.P. BP program?
• Help us improve – please complete the survey
• If not registered…. COME JOIN US!
http://www.telligenqio.org/initiatives#cardiachealth
47
Contact
anna.astalas@area-d.hcqis.org
(630)928-5832