Musculoskeletal disorders, Nov 6
advertisement

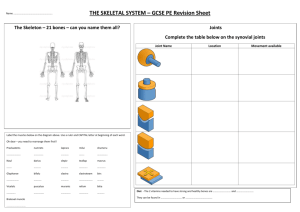
Musculoskeletal Disorders Psych Rehab Nursing Fall 2009 Outline • • • • Overview of anatomy and physiology Diagnostic tests Musculoskeletal trauma Problems of the musculoskeletal system – Osteoporosis – Osteoarthritis – Rheumatoid arthritis – Gout – Other musculoskeletal problems Review • Purpose of the musculoskeletal system - Supporting framework for attachment of muscles and other tissues - Protects vital organs and soft tissues - Joints, bones, cartilage make up the skeletal system - Bones enable movement of the body by acting as levers and points of muscle attachments (muscles ONLY contract: opposing muscles allow flexion & extension. Muscles are conductors of electrical energy) Bones • Function • Framework for the attachment of muscles and other tissues • Protection • Production of blood cells in the red marrow - Which bones are involved in the process? - Facilitate movement by contracting muscles - Storage area for calcium and phosphorus - Lipids (energy sources) are stored in adipose cells of the yellow marrow Bones • Blood cells are produced in bone marrow (see below) • Red marrow in flat bones (sternum, scapulae, skull, ribs, vertebrae, pelvis, epiphyseal ends of long bones, i.e., femur and humerus (marrow runs all the way through the bone, but the cells are released from the epiphyseal ends) Femur head; view of cortex; view of red bone marrow; view of yellow bone marrow (2009) Bones Ligaments (fibrous connective tissue connecting bone to bone) Tendons (connect muscle to bone) Example: Achilles tendon attaches calf muscles to the ankle bone while a ligament holds the calf and thigh bones together at the knee joint (Pollick, 2008) Bones: Types • • • • • • Long bones Short bones Flat bones Irregular bones Sesamoid (or round) bones Sutural or Wormian bones Long Bones • Long bones – – – – Longer than they are wide A shaft with two ends - the shaft widens at the end of the bone Contain yellow bone marrow and red bone marrow Humerus (proximal) ; radius and ulna (distal) of the upper extremity; femur (proximal), tibia (anterior/distal) and fibula (posterior/distal) of the lower extremity Long Bones • Examples of long bones • • • • • • Metacarpals Phalanges 9 14 10 15 11 16 12 13 Red and Yellow Bone Marrow • Half of the bone marrow is red (in adults) • Red marrow is found mainly in the flat bones (hip bone, sternum, skull, ribs, vertebrae and shoulder blades) • Also found in the spongy material in the proximal ends of the long bones – femur and humerus • Yellow marrow is found in the hollow interior of the middle portion of long bones Femur head; view of cortex; view of red bone marrow; view of yellow bone marrow (2009) Bone Marrow • Hematopoesis (blood formation) • RBC storage • Production of WBCs • Platelets (formed in bone marrow; aid in clotting) • High fat content (long bones) fat embolus • “Fat embolism syndrome, a condition characterized by hypoxia, bilateral pulmonary infiltrates, and mental status change, is commonly thought of in association with long-bone trauma. … Although studies suggest that embolization events infrequently result in clinically apparent fat embolism syndrome, clinicians should be vigilant in considering fat embolism as a causative agent for postoperative respiratory distress.” (Glazer & Onion, 2001) Short Bones • Short bones – Cube-like; about as long as they are wide • Contain mostly spongy bone • Outside surface consists of a thin layer of compact bone • Located in the hands and feet (metacarpals) • Patella Long Bones • ?? Flat Bones • Flat bones – Thin and flat – Found where the need is for a broad surface area for muscular attachment or where extra protection is needed – Examples: Skull; Pelvis; Sternum; Rib cage; Scapula – In adults most RBCs are formed in flat bones Bones: Microscopic Anatomy • Osteoprogenitor cells are multipotential skeletal cells; the stem cells for the skeletal system. • Osteoblasts are bone forming cells; they lay down the bond tissue. Can be stimulated in cancer. • Osteocytes are mature bone cells that become trapped at maturity in a matrix; they maintain the bone • Osteoclasts are bone reabsorbing cells that destroy old bone. Slow process. Inc cancer, these cells are destroyed and not replaced (osteoporosis). • Collagen is soft, strong connective tissue that supports and reinforces the mineralized matrix – stronger than steel. Irregular Bones • Examples are the vertebrae; sacrum; coccyx; temporal; sphenoid; ethmoid (in skull); zygomatic (cheek bone); maxilla; mandible; palatine; inferior nasal concha; and hyoid • Serve as protection (example: vertebrae protects spinal cord) • Allowing multiple anchor points for skeletal muscle (example: sacrum) Bones • Ligaments (bone to bone): fibrous connective tissue connecting bone to bone • Tendons: (connect muscle to bone) Example: achilles tendon attaches calf muscles to the ankle bone while a ligament holds the calf and thigh bones together at the knee joint. Sesamoid (Round) Bones Sutural, or Wormian bones • An example of a Sesamoid bone is the patella • Sesamoid bones are embedded within tendons; Act to protect tendons • Sutural or Wormian bones occur between the sutures of the cranial bones Bones: Types • Long Bones: weight bearing, strong, curved • Short bones: compact on surface, spongy center & cuboidal (metatarsals) • Flat bones: parallel surfaces of the body, protecitve funciton, broad attachment surface (ribs, pelvis, skull, ilium) • Irregular bones: various functions: vertebrae & some facial bones • Sesamoid (or round) bones: embedded in tendons, allow change of direction of movement, like a pulley (patella) • Sutural or Wormian bones: between sutures of skull (between large flat bones of skull) Joints • A diarthrosis joint is a freely moveable joint – always a synovial joint • Types of synovial joints – Gliding (Two sliding surfaces) (Example - between carpals) – Hinge (Concave surface with convex surface) (Example – between humerus and ulna) – Pivot (Rounded end fits into ring of bone and ligament (Example – between atlas (C1) and axia (C2) vertebrae Joints Synovial Joint Diarthrosis Joint (all are synovial joints) Joints, Synovial types, cont. 1. Ball and socket joint (Ball-shaped head with cup-shaped socket) (Example – Between femur and pelvis) 2. Condyloid joint (Oval condyle with oval cavity) (Example – between metacarpals and phalanges) 3. Saddle joint (Each surface is both concave and convex) (Example – Between carpus and the first metacarpal) 4. Hinge joint (interphalangeal joints) 5. Pivot joint (able to rotate – neck, forearm, knees) Muscles • Source of power and movement • Three types… – Skeletal Muscle – Cardiac Muscle – Smooth Muscle Skeletal Muscle • Skeletal Muscle – Attached to bones and causes movements of the body. – Also called striated muscle (actin &??) because of its banding pattern, or voluntary muscle (because muscle contraction can be consciously controlled) Cardiac Muscle • Cardiac muscle – Responsible for the rhythmic contractions of the heart – Muscle is involuntary – Generates its own stimuli to initiate muscle contraction – Microscopically striated like skeletal muscle – Striations join together in bundles to allow coordinated action – Involuntary and autorhythmic. Some cardiac muscles function as built in pacemakers. Smooth Muscle • Smooth Muscle – Lines the walls of hollow organs – (Example: lines the walls of blood vessels and of the digestive tract where it functions to advance the movement of substances. – Contraction is relatively slow and involuntary – Microscopically smooth (not striated) Basic components • Muscles are stimulated by motor neurons. • Richly supplied w/ arteries and veins and have intimate contact w/a rich capillary network b/c of high energy demands. Diagnostic Tests for Musculoskeletal • • • • • • • • • X-ray Electromyogram (EMG) Arthroscopy Arthrogram Computerized Axial Tomography (CT) Magnetic Resonance Imaging (MRI) Bone Scan Arthrocentesis Laboratory Testing – – – – – Antinuclear Antibodies (ANA) Ca+, P Rheumatoid Factor (RF) Erythrocyte Sedimentation Rate (ESR) Uric Acid Chemical action in muscle • ATP – ADP energy cycle. Critical to muscles ability to get energy they need to do the work they need to do. Soft Tissue Injuries • • • • • • • • • Sprains/Strains Sports-related Dislocation/Subluxation Carpal Tunnel Syndrome Rotator cuff Repetitive Strain Meniscus Injury Bursitis Muscle spasms Dislocation / Subluxation • Dislocation of joint • Subluxation (partial dislocation of joint) • Candidate joints are shoulders, fingers, kneecaps Trauma to Bone • Highest incidence – MALES 15-24 years of age or elderly females 65 years of age, or older – Why are females in this age group affected? • A result of a blow to the body, a fall, or another accident A rotator cuff injury includes any type of irritation or damage to the rotator cuff muscles or tendons. Causes of a rotator cuff injury may include falling, lifting and repetitive arm activities — especially those done overhead, such as throwing a baseball or placing items on overhead shelves (Mayo Clinic, 2008) Rotator Cuff Injury Meniscus Injury • • • • • • • • • Symptoms of medial meniscus tear A history of trauma or twisting of the knee Pain on the inner surface of the knee joint Swelling of the knee within 24-48 hours of injury Inability to bend knee fully- this may be associated with pain or a clicking noise A positive sign (pain and/or clicking noise) during a "McMurrays test" Pain when rotating and pressing down on the knee in prone position (video). "Locking" of the knee Inability to weight bear on the affected side (SIC, 2008) Muscle Spasm • Inflammation that occurs when a muscle is overstretched or torn • The back is a common area for inflammation to occur • Why? Poor body mechanics • (cold or heat might be effective, reduce inflammation & relax muscles) Bursitis: Inflammation of the Bursa (Pain, fluid build up, calcium deposits & loss of motion in the joint. Prevention is to build up activity gradually. Treatment: avoid what is causing the problem, NSAIDS, steroids, ice. In some cases surgery might be necessary. Types of Complete Fractures • Closed (Simple) • Open (Compound): riskiest due to infection, bone breaks through skin. • • • • • Transverse Oblique Spiral Comminuted Colles’ fracture: fracture of wrist on inside portion of wrist. Treatment is reduce it & cast it. (happens when someone falls down). Responds well to cast. Fractures • Fractures commonly tear blood vessels, producing a hematoma • This area of hematoma is commonly used as an area to anesthetize the periosteum because thisis where the blood vessels are located. • Reduction usually requires anesthesia Healing stages • After several weeks the periosteum is beginning to heal & lay down scar tissue. Trabecular cone has begun to grow over the break. There is callus formation w/ the osteoblasts • After several months….. Healing stages, cont • Remodeling: over the next months or years, the bone shape returns to normal as osteoclasts absorb extra cells and osteoblsats generate new cells and bone. The bone will be thickened somewhat at the fracture… • Fully healed fractures in children are indistinguishable from the original bone b/c the growth plates are open. However, multiple fxs in various stages of healing are a strong indicator of child abuse Closed Simple Fracture • Only bone damage • Little or no soft tissue damage • Does not penetrate skin Open Fracture • Probably need surgery… lot of time spent cleaning the wound • Wound may be left open for a while… Transverse Bone Fracture • Often caused by direct traumatic injury • Bone has been broken giving rise to a transverse break or fissure within the bone at a right angle to the long portion of the bone Oblique Bone Fracture • Extremely rare type of break • An oblique break in the bone which is very unstable (break at an angle) • Bone still together… Spiral Fractures • Bone is broken due to twisting-type motion • Unstable fracture • Looks like corkscrew – runs parallel with the axis of the broken bone Comminuted (crushed) Fracture • More than two fragments of bone have been broken off • Highly unstable with many bone fragments • (Fixed w/ rods & screws after taking all the pieces out) Types of Incomplete Fractures • Greenstick • Torus (closed) (side of the bone bends but does not break) • Bowing • Stress Greenstick fracture • Usually seen in children • Bone is usually “bent” and broken on the outside of the bend • If kept straight, heals quickly • (sometimes doesn’t need a cast… sometimes overtreated) Stress Fracture • Incomplete fracture • Most common symptom is pain • Caused by “unusual or repeated” stress – this • Most are not associated in contrast to other type with swelling or fractures resulting from redness, but tenderness trauma to palpation • Common sports injury • Tibia (shin splintsand among soldiers runners) and from marching metatarsal bones affected in runners • Tiny hairline fractures Stress Fracture • Example of a stress fracture • Common runnertype fracture Other Types of Fractures • Pathologic Fracture – May occur during normal activity or after minimal injury (Is associated with what?) common in elderly w/ osteoarthrits or osteoporosis • Fatigue or Stress Fracture – The muscles associated with the bones are unable to absorb energy as they usually do • Avulsion Fracture – A strong ligament or tendon pulls a fragment of the bone away from the rest of it • Impacted Fracture – Fracture fragments are pushed into each other Clinical Manifestations 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. Pain Loss of normal function Obvious deformity Excessive motion Crepitus (fluid builds up on joint, can be felt at the joint) Edema Warmth Ecchymosis Loss of sensation Signs of shock X-ray evidence Factors that hinder good callus formation • Inadequate reduction of the fracture • Inefficient immobilization • Excessive edema at the fracture site, impeding the supply of nutrients • Too much bone lost at time of injury to permit bridging of broken ends • Infection at the site of injury • Bone necrosis • Anemia or other systemic conditions • Endocrine imbalance (parathyroid not enough Ca) • Poor dietary intake Neurovascular Assessment (5 Ps) • Pain • Paresthesia (tingling, pricking, or numbness of the skin) • Pallor • Pulses • Paralysis Goals • • • • Prevent injury Maintain strength Promote comfort Maintain intact neurovascular status Treatment Objectives for Fracture • Reduction of fracture • Maintenance of fragments in correct alignment • Prevention of excessive loss of mobility and muscle tone Collaborative Management • • • • • Health History X-ray/CT/MRI/Scan Fx Reduction Fx Immobilization MEDS – Analgesics – Antibiotics – Tetanus Toxoid (good for 10 years) Immobilization of Bones • 1) Physiologic Splintage- naturally occurring phenomenon related to pain that causes guarding, muscle spasms, and avoidance of further use. There is a desire to rest the whole body until some repair has occurred. • 2) External orthopedic splintage- with devices such as casts • 3) Internal Fixation with screws, pins, rods or plates to hold the opposing ends of the fracture in place Bone Healing • 1. Hematoma formation (situates between broken fragments) • 2. Fibrin meshwork formation (blood vessels grow into a jelly-like matrix of the blood clot – WBCs are brought to the site • 3. Invasion of osteoblasts (produces matrix that becomes mineralized) • 4. Callus formation (usually shows up by x-ray 6 weeks in adults/less time in children • 5. Remodeling (bones are constantly changing – osteoclasts break down old bone so osteoblasts can replace it with new bone tissue – a process called remodeling. • What can impair bone healing? Bone Healing Fractures: terms commonly used • Reduction: re-establishment of the normal position of .. • Dislocation • Fracture • Internal fixation is the surgical placement of steel material into the bone to hold it in place. Used when healing would be impaired or immobility of the fx is a problem. Factors that Hinder Good Callus Formation • Inadequate reduction of the fracture • Inefficient immobilization • Excessive edema at fracture site, impeding the supply of nutrients • Too much bone lost at time of injury to permit bridging of broken ends • Infection at the site of injury • Bone necrosis • Anemia or other systemic conditions • Endocrine imbalance • Poor dietary intake Immobilization and Care • External fixation devices – Casts (plaster casts can be bi-valved to allow for swelling)-this means it is cut into two pieces, lengthwise, so that the area beneath the cast can be observed. – Splints – Brace or cast-brace • Traction (weights should hang freely) – – – – • Skin traction Skeletal traction Balanced suspension Counter-traction Internal Fixators – Plates and screws – Rods – Prosthetics • Bone Stimulation External Fixator • Used when a cast would not allow proper alignment/immobilization of the fracture • Proper cleaning to prevent infection is required • No cast, just curlex (gauze) Traction • Aligns the ends of a fracture by pulling the limb into a straight position • Helps manage muscle spasm r/t fracture • (weights should hang freely) • Skin traction • Skeletal traction • Balanced suspension • Counter – traction • Skin integrity or back massage might be helpful. Often used pre-op to keep them immobile Bone Stimulation • Used when satisfactory healing is not occurring naturally • Application of a low electrical current to the fracture • Promotes the speed of bone healing Nursing Diagnoses • • • • • • • Risk for Neurovascular Dysfunction Pain Risk for Infection (Risk for) Impaired Skin Integrity Risk for Nutrition Deficit Risk for Injury Knowledge Deficit (teaching about care of the site) • Risk for impaired perfusion Complications • Who is at risk?: 0.5%-2% long bones, 10% hip • DVT Stroke or Pulmonary Embolus – S/S of PE: Hemoptysis (coughing up of blood), pleuritic chest pain, dyspnea, rales • Fat Embolism Syndrome (When fat enters the circulation) – 12-48 hrs after fracture – Usually associated with fx of long bone or pelvis (fx of hip is at highest risk) – Men 20 to 40 years of age and older adults 70 to 80 years of age at greatest risk for development – Mental status changes (hypoxemia), tachypnea, dyspnea, tachycardia, temperature, petechia of upper body and axilla, feeling of impending doom Complications • Compartment Syndrome – 4-12 hrs after fracture – Compartments are areas of the body in which muscles, blood vessels, and nerves are contained within fascia – Progressive pain distal to fracture, 5 Ps (pain, pressure, paralysis, paresthesia, pallor and pulselessness), pressure inside compartment >30mmHg (normal 0-8 mmHg – Fasciotomy (opening in the fascia) Deep Vein Thrombosis Deep Vein Thrombosis Route of DVT embolus Pulmonary embolism Hip Fractures • Currently more than 250,000 hip fractures annually • Associated costs exceed $7 billion • Repair of a fractured hip is the most common procedure performed in people over 85. • 30% of patients with a hip fracture die within 1 year r/t surgery (complications) & immobility • Osteoporosis is biggest risk factor Classification of Hip Fractures • • • • • • Intracapsular Extracapsular Intertrocanteric Subtrocanteric Transcervical Impacted at base of the neck • (Capsular refers to the proximal 1/3 of bone) Signs of Symptoms of Hip Fracture • • • • Medical emergency Severe pain at the fracture site Inability to move leg voluntarily Classicshortening and external rotation of the leg • One-third of elderly individuals with hip fracture die within one year of injury • Typically the bone is rotated externally & shortening of the leg… try to get the leg back into allignment… Medical Management – Hip Fracture • Conservative management – Prolonged immobility - 12-16 wks BR(avoids the risks associated with anesthesia) • Surgical Management – Reduction and stabilization of fracture with insertion of internal fixation device • Stable plate and screw (non-w/b 6 weeks to 3 months) • Telescoping nail (minimal to partial w/b 6 weeks3 months) – Prosthetic implant -replaces femoral head and neck • position restriction 2 weeks->2 months • partial weight bearing 2 months Follow-up Instructions – Hip Fracture • DO NOT – flex more than 90o – force hip into adduction or internal rotation – cross legs – put on own shoes and socks x 8 weeks – sit in chairs that do not have armrests Follow-up Instructions – Hip Fracture • DO – Keep in extension and abduction – use toilet seat raiser – place/use shower chair – use pillow between legs x 8 weeks – notify of increased pain – inform dentist of prosthetic device 5 Ps of neurovascular assessment • May be a test question • Pain • Paresthesia (tingling, prickling or numbness of the skin) • Pallor • Pulses • paralysis Hip Fracture Hip Fracture • Severe pain at the fracture site • Inability to move leg voluntarily • External Rotation Total Hip Replacement –Preoperative care-consider psychosocial issues-family supportcomfort-safety –Postoperative care-hip is kept in extension and abduction to prevent dislocation of the hip Osteomyelitis • Acute or chronic infection of bone (confirmed by positive wound culture) – Usually staph aureus – Direct or indirect • • • • Pain, temperature, swelling, warmth, redness Wound culture, bone scan, CT, MRI Aggressive antibiotics 6-8 wks (my pt at Speciality) Nursing diagnoses: Pain, Impaired physical mobility, Ineffective therapeutic regimen, Risk for impaired skin integrity • Nursing care: Aseptic technique, no heat or exercise to affected area which will increase circulation Osteomyelitis Osteoporosis • A disorder in which bone mass is lost to the point where the skeleton is no longer able to withstand unexpected or normal mechanical forces. Most common skeletal disorder and second only to arthritis as a cause of musculoskeletal morbidity in the elderly. A/K/A porous bone • Bone resorption > bone formation Osteoporosis Osteoporosis Risk Factors • • • • • • • • Aging Gender (female) Race (white) Family History Postmenopausal (and not taking calcium supplement) Chronic calcium deficiency Sedentary lifestyle (wt bearing exercise) Small frame-low body weight Osteoporosis – Related Risk Factors • Chronic smoking • Diet high in protein and fat (phosphorous depletes calcium – found in animal fat/protein) • Chronic alcohol use • Excessive caffeine intake (phosphorous depletes calcium) • Postmenopausal (estrogen helps body absorb calcium) • Glucocorticoids (involved in protein and fat metabolism; Aluminum containing antacids (reduce amount of calcium in the body) • Horonal imbalances (estrogen and testosterone) are the primary causes of osteoporosis Osteoporosis – Secondary Risk Factors • Endocrine disorders: Hyperthyroidism, hyperparathyroidism • GI Disorders – malabsorption syndrome, Hyperthyroidism, parathyroidism • COPDglucocorticoids • Drug – Glucocorticoids, heparin, anticonvulsants, loop diuretics, barbiturates Osteoporosis Clinical Manifestations • Back Pain- (fx of vertebra) – Chronic dull ache – Sudden onset of acute pain greatly intensified with coughing, sneezing or movement • Fracture – – – – Proximal femur Distal radius Proximal humerus Ribs • Thoracic kyphosis (Dowager’s hump) • Loss of more than 2 in. standing height Osteoporosis Collaborative Management • Diagnosis – – – – Labs may not be helpful X-rays (at 30-50% loss) CT , MRI, Bone Scan Bone Mineral Density Measurement • Medication – – – – Estrogen Replacement: Prevention Calcium Supplements Calcitonin : Nasal spray->irritating Fosamax, Boniva (1X/ month) Actonel: Before breakfast without food, sit upright X 30 min., full glass water • Vertebroplasty, Kyphoplasty Osteoporosis Nursing Management • Nursing diagnoses: Pain, Impaired physical mobility, Risk for injury, Imbalanced nutrition: less than body requirements • Promote calcium intake • Review diet to include: – Decrease caffeine • Excess calcium loss – Decrease protein and fat • High protein diet causes bone loss secondary to calcium loss • Promote exercise – active weight bearing, walking Paget’s Disease • Excessive bone resorption followed by bone formation leading to weakened bone, bone pain, arthritis, deformity leading to pathologic fractures and osteogenic sarcoma • Bone marrow replaced by vascular fibrous connective tissue leading to formation of larger, disorganized, weaker bone • X-ray, increased alkaline phosphatase, positive bone scan • Medication (Fosamax, Actonel) with slowing of disease with early diagnosis Paget’s Disease Osteoarthritis (DJD) • • • • Degenerative Joint Disease Most common form of arthritis in the elderly #1 cause of disability and limitation in those over 74 Non-inflammatory disease of moveable joints – Deterioration in articular cartilage and formation of new bone at the joint Osteoarthritis (DJD) Osteoarthritis Osteoarthritis Risk Factors • • • • Age Obesity Repetitive joint injuries Genetics Osteoarthritis Cardinal Symptoms • Pain – After movement relieved by rest – Characterized as aching – Poorly localized – On motion with weight bearing Osteoarthritis Cardinal Symptoms • Stiffness – On awakening and in AM – After activity – Of relatively short duration Osteoarthritis Other Signs and Symptoms • • • • Crepitus Limitation of motion Weight-bearing joints weaken (asymmetrical) Heberden nodes – Lateral enlargements of the distal phalangeal joints • Bouchard’s nodes (found at the proximal interphalangeal joints) Bouchard Nodes Heberdan Nodes Osteoarthritis – Diagnosis • X-Ray – Decreased joint space, bony sclerosis, spur formation • Fluid analysis Osteoarthritis - Treatment • Symptomatic relief and minimization of further joint destruction – Exercise – Rest – Weight-loss – NSAIDs • Gastric irritation, bleeding • Disturbance in platelet formation Rheumatoid Arthritis • Chronic, systemic inflammatory disease of moveable joints • 6 million Americans • Prevalence increases with age for both men and women Rheumatoid Arthritis Rheumatoid Arthritis Rheumatoid Arthritis – Cardinal Symptoms • Unexplained periods of exacerbation and remission • Painful, swollen joints, – Bilateral, symmetrical • Morning stiffness – Lasting longer than 1 hour – In AM and after inactivity Rheumatoid Arthritis – Cardinal Symptoms • Abnormal labs – Elevated ESR (sed rate) – Rheumatoid factor – Anemia – WBC in synovial fluid • X-Ray – Bone degeneration Rheumatoid Arthritis – Diagnosis • Based on cluster (4 for 6 weeks) – Morning stiffness – Arthritis in three or more joints – Arthritis of hand joints – Symmetrical – Rheumatoid nodules – Serum rheumatoid factor – Radiographic changes Rheumatoid Arthritis Treatment Goals • • • • • • Reduce inflammation Alleviate pain Preserve function Prevent deformity (treatment is the same as OA, pretty much) Both RA & OA cause severe loss of quality of life Rheumatoid Arthritis – Management • • • • • • Rest PT Aspirin Corticosteroids Gold salts Disease modifying antirheumatic drugs (DMARDs) – Plaquenil, Azulfadine – Methotrexate Rheumatoid Arthritis Comparison of OA to RA OA • Degenerative joint dz • Affects articular cartilage • Need to add more RA • Autoimmune joint dx “inflammatory arthritis” • Affects synovial membrane • Membrane thickens and immobilizes the joint Gout: Gouty Arthritis • Affects middle aged to elderly men • Associated with renal stones r/t sodium urate crystal deposition • Treated with drugs that promote uric acid excretion (allopurinol and probenicid) • Treated with diet-limiting protein(organ meats, red meats, i.e., high purine food) (Gout is associated with increased uric acid in the body; Purines increases uric acid levels in the body) • Unlike other forms of arthritis absolute rest of the joint is necessary. So painful it causes extreme pain just to touch the joint. • Primary form is inherited • (aspirin not indicated, can make the uric levels higher) Mandible Fracture – Preoperative care-history of injury, pain control, gentle oral care, psycho-social – Postoperative care-pain control, observe for s/s infection, suction equipment at bedside, liquid diet, careful monitoring of airway, ready to cut wires if client vomits or has respiratory emergency(wirecutters at bedside) Mandibular Fracture Amputation – Preoperative care-nurse does history(how it occurred if trauma), concurrent illnesses, habits, ie. Smoking, current meds, psychosocial – Postoperative care-pain management including phantom pain, prevent infection, observe for adequate tissue perfusion – Nursing dx: prevention of infection, promotion of mobility, preparation for prosthesis… Amputation Accidental Surgical Bone Cancer –Multiple Myeloma –Osteogenic sarcoma,Osteoclastoma, Ewing’s Sarcoma, Metatastic Bone Disease Primary Bone Cancer – Multiple Myeloma (Plasma cell myeloma) • Invades sternum, ribs, spine, clavicles, pelvis, long bones. Sx: back pain, anemia, thrombocytopenia. – Osteogenic sarcoma • Metaphyseal area of long bones, esp. distal femur, proximal tibia, proximal humerus. • 10-25 y/o males – Osteoclastoma (Giant cell tumor) • Cancellous bone: distal femur, proximal tibia, distal radius. • 20-35 y/o. • Swelling local pain, bone destruction on Xray – Ewing’s Sarcoma 3rd most common • Males under age 30 • Medullary cavity of long bone esp. femur, pelvis, tibia, ribs. • Mets to lung – Metastatic bone lesions from breast, GI tract, lungs, prostate, kidney, ovary, and thyroid Other Musculoskeletal Problems • Muscular Dystrophy • Low Back Pain-Laminectomy • Herniated Intervertebral Disk