What is ICD-10 and why do I care?

ICD-10
What Is It And
Why Do I Care?
Presented by:
Karen Kvarfordt, RHIA, CCS-P, CCDS
AHIMA Approved ICD-10-CM/PCS Trainer
President, DiagnosisPlus, Inc.
2015
1
ICD-10 Changes Everything!
It will change the way in which we document patient care in our medical records both in the hospital and in our physician practices.
Tell the patient story better!
2
ICD-10
WHO (World Health Organization) owns & publishes ‘ICD’ (International Classification of
Diseases).
WHO endorsed ICD-10 in 1990; members began using ICD-10 or modifications in 1994.
United States is the only industrialized country not using ICD-10 for our coding & reporting of diseases, illnesses, and injuries. Why?
What makes us so different?
3
Countries Using ICD-10
For Case Mix
United Kingdom (1995)
Denmark, Finland, Iceland, Norway, Sweden
(1994 – 1997)
France (1997)
Australia (1998)
Belgium (1999)
Germany (2000)
Canada (2001) ( 30,000 diagnosis codes)
United States (2015)
( Reimbursement + Case Mix )
4
What is ICD-10?
Currently the U.S. health care industry uses ICD-9-CM codes for identifying and reporting diagnoses and procedures.
ICD-10 will replace the existing ICD-9 code sets (diagnosis
& procedure) effective October 1, 2015 .
ICD-10-CM = Diagnosis codes
ICD-10-PCS = Inpatient hospital procedure codes only
No impact on CPT and/or HCPCS codes!
CPT and HCPCS codes will continue to be used for physician and outpatient services including physician hospital visits (Observation & Inpatient) = E&M
5
ICD-10 Impact
ICD-10-CM ( Diagnoses )
Will be used by all hospitals, providers, clinics, lab, radiology, psych, rehab, nursing homes, etc.
ICD-10-PCS ( Procedures )
Will be used only for hospital claims for inpatient hospital procedures
CPT/HCPCS – No change!
Procedures for Hospital Outpatients, Physician
Visits, Lab and Radiology Outpatients, etc.
6
Why Should We Do ICD-10?
What is the benefit to the provider?
Greater specificity in identifying health conditions.
The greater level of detail in the new code sets will include laterality, severity and complexity of disease conditions, which will enable more precise identification and tracking of specific conditions.
Terminology and disease classification are now consistent with new technology and current clinical practice.
7
Additional Benefits…
Share higher-quality data with other health care providers.
ICD-10 increases the amount of “specific” information in every diagnosis code and makes this more valuable to other providers.
For example, ICD-9 has a code for laceration of a finger.
ICD-10 lets you know if that laceration was of the index, little, middle, ring finger or thumb and if it was left, right, or bilateral.
8
Reimbursements will better align with activity & cost.
Payers will reimburse severe & complex cases better and simple cases at lower rates.
How? By the diagnosis codes!
9
Here’s an Example
Imagine you had a patient who was noncompliant with their medical therapy.
In ICD-9, the only code we have available is V15.81 (personal history of noncompliance with medical treatment).
Is the patient noncompliant because of their own personal reason? Or something else?
10
How Will it Look in ICD-10?
Z9111 (Patient’s noncompliance with dietary regimen)
Z91120 (Patient's intentional underdosing of medication regimen due to financial hardship)
Z91128 (Patient’s intentional underdosing of medication regimen for other reason)
Z91130 (Patient’s unintentional underdosing of medication regimen due to age-related debility)
Z91138 (Patient’s unintentional underdosing of medication regimen for other reason)
Shows whether or not the patient’s noncompliance was intentional, but also identifies if the patient needs some form of assistance from social services, etc.
11
Diagnosis Coding
(ICD-10-CM)
12
ICD-10-CM
Allows for greater “ specificity & detail ” which is currently lacking in ICD-9-CM.
Moving from 14,025 ► 69,823 diagnosis codes!
25,000 (36%) of all ICD-10-CM diagnosis codes will now distinguish ‘right’ vs. ‘left’.
Must be documented in the medical record for code capture.
Expanded # of characters of the ICD-10-CM diagnosis codes will provide greater specificity to identify: Etiology, Anatomical site, & Severity
13
Why Are There So
Many New Codes?
Main difference between ICD-9-CM and ICD-
10-CM codes, outside of structural changes, is the “SPECIFICITY” of the code.
ICD-10-CM diagnosis codes will range anywhere from 3 to 7 characters which will allow us to capture this greater detail.
But it must be documented in the record!
14
ICD-10 Documentation
Concepts
Stage or grade of disease
Specific anatomical location
Acute vs. chronic
Severity: mild, moderate, severe
Episode of care: initial vs. subsequent vs. sequela
Injuries, Fractures, & Poisonings
Laterality: right, left, or bilateral
15
ICD-9-CM vs. ICD-10-CM
ICD-9-CM
◦
◦
◦
◦
◦
◦
3 - 5 digits or characters
1st character is numeric or alpha (E or V codes)
2 nd – 5 th characters are numeric
Decimal placed after the first 3 characters
17 Chapters and “V” & “E” codes are ‘ supplemental ’
14,025 diagnosis codes
ICD-10-CM
◦
◦
◦
◦
◦
◦
3 - 7 digits or characters
1 st character is alpha (all letters used except “U”)
2 nd – 7 th characters can be alpha and/or numeric
Decimal placed after the first 3 characters (the same!)
21 Chapters and “V” & “E” codes are ‘ not ’ supplemental
69,823 diagnosis codes
16
Level of Detail Example
ICD-9-CM (irregular astigmatism) (367.22)
Only 1 code currently in ICD-9-CM
ICD-10-CM (irregular astigmatism)
Will have four choices:
H52.211 (irregular astigmatism, right eye)
H52.212 (irregular astigmatism, left eye)
H52.213 (irregular astigmatism, bilateral)
H52.219 (irregular astigmatism, unspecified eye)
Physicians are likely documenting “laterality” now, but coders aren’t looking for it.
Biggest Change in ICD-10-CM
LATERALITY
For bilateral sites, the final character of the codes in
ICD-10-CM indicate laterality.
Right side is always character 1 ( RT )
Left side is always character 2 ( LT )
Bilateral code is always character 3 ( RT & LT )
But be careful! Not all codes will have a ‘bilateral’ distinction, i.e., carpal tunnel, etc.
“Unspecified” side code is also provided should the side not be documented in the medical record.
Did we just lose our specificity?
18
Diagnoses That Will
Require Laterality
Joint pain
Joint effusion
Injuries
Fractures
Dislocations
Arthritis
Cerebral infarction
Extremity atherosclerosis
Pressure ulcers
Injuries
Seventh (7 th ) character identifies the patient encounter type, with “ A ” for the initial encounter, “ D ” for the subsequent encounter and “ S ” for sequela encounter.
Initial = Patient is receiving ‘active’ treatment
First time being seen for the injury, i.e., ER visit, surgery, evaluation by new physician
Subsequent = Follow-up care
Sequela = Complication of a previous injury
20
Examples of ICD-10-CM
Emergency Room
I10 Essential (primary) hypertension
S01.02
x A Laceration with foreign body of scalp, initial encounter
S01.02
x D Laceration with foreign body of scalp, subsequent encounter
S02.2
xx A Fracture of nasal bones, initial encounter for closed fracture
H65.0
1 Acute serous otitis media, right ear
H65.0
2 Acute serous otitis media, left ear
H65.0
3 Acute serous otitis media, bilateral
21
Procedure Coding
(ICD-10-PCS)
22
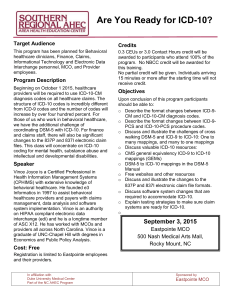
ICD-10-PCS Characters
(Medical and Surgical Section)
1
Section
2 3
Root
Operation
4 5
Approach
6 7
Qualifier
Body Body
System Part
Device
23
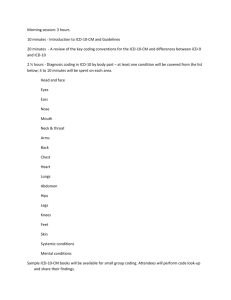
Dissect ICD-10-PCS Code
Endoscopic Esophageal Excision via Natural or Artificial Opening
ICD-9-CM: 45.16 Esophagogastroduodenoscopy (EGD) with Closed Biopsy
0
Section
(Medical/Surgical)
D
Body System
(Gastrointestinal)
B
Root
Operation
(Excision)
5
Body Part
(Esophagus)
8
Approach
(Via natural or artificial opening endoscopic)
Z
Device
(No Device)
X
Qualifier
(Diagnostic)
24
Here’s Another Example…
1
Section
(Obstetrics)
Extraction of Products of Conception, Low Cervical,
Open Approach
ICD-9-CM: 74.1 (Low Cervical Cesarean Section)
0
Body System
(Pregnancy)
D
Root Operation
(Extraction)
0
Body Part
(Products of
Conception)
0
Approach
(Open)
Z
Device
(No
Device)
1
Qualifie r
(Low
Cervical)
25
What’s New In ICD-10?
26
Obstetrics
Under ICD-10-CM diagnosis codes will be based on the stage of pregnancy:
First trimester
Second trimester
Third trimester
Trimesters are counted from the first day of the last menstrual period, and defined as:
First trimester: Fewer than 14 weeks
Second trimester: Fourteen weeks
Third trimester: Twenty-eight weeks
27
Nicotine Dependence
ICD-10-CM contains a separate category for nicotine dependence with subcategories to identify the specific tobacco product and nicotine-induced disorder(s). For example:
Cigarettes
Chewing tobacco
Cigar, etc.
ICD-9 has only one diagnosis code (305.1) for tobacco use disorder or tobacco dependence.
28
Underdosing
New diagnosis code in the ICD-10 world!
Identifies situations in which a patient has taken less of a medication than prescribed by the physician and captures those reason(s).
Must be documented in the record!
Financial
Non-compliance*
29
Burns and Corrosions
Burn codes identify:
Thermal burns, except for sunburns, that come from a heat source
Burns resulting from electricity and/or radiation
Addition of the term “ corrosion ” is new in
ICD-10-CM:
Corrosions are burns due to chemicals
30
Physician Documentation
31
Top 10 Documentation
‘Pearls’
5.
6.
7.
8.
1.
2.
3.
4.
9.
10.
Laterality (left vs. right)
Stage of Care (initial or follow-up)
Specific Diagnosis (acute vs. chronic)
Specific Anatomy (specific bone in the hand)
Associated and/or Related Conditions
Cause of Injury (hit by baseball, fall)
Documentation of Additional Symptoms or Conditions
Dominant vs. Non-Dominant Side
Tobacco Exposure or Use
Gustilo-Anderson Scale
32
Documentation Tips
For Specific Diagnoses
33
GERD Documentation
ICD-10-CM will include 2 diagnosis codes but does not include the abbreviation “GERD”
K21.0 (Gastro-esophageal reflux disease with esophagitis)
K21.9 (Gastro-esophageal reflux disease without esophagitis)
Barrett’s now broken down:
With or without ulcer
With or without dysplasia
Staging of dysplasia
Low grade
High grade 34
Digestive Ulcer
Documentation needs to include the specific location:
Gastric
Duodenal
Peptic
Gastrojejunal
Further specificity needs to identify:
Acute or chronic
With hemorrhage
With perforation
With hemorrhage and perforation
Without mention of hemorrhage or perforation
35
Asthma Documentation
Document the Severity (3 levels):
1.
Mild (more than two times per week)
2.
3.
Moderate ( daily and may restrict physical activity)
Severe (throughout the day with frequent severe attacks limiting the ability to breathe)
Clarify whether acute, chronic, intrinsic or extrinsic
Specify exercise-induced or other forms
Specify when chronic state asthmatic bronchitis exists and when acute exacerbation occurs
Document tobacco exposure or history of
36
Congestive Heart Failure
Documentation in ICD-10-CM needs to identify whether the CHF is acute or chronic and the specific ‘type’ of heart failure:
Combined systolic & diastolic
Diastolic
Systolic
Left ventricular
37
Bronchitis
Need to include specificity such as:
Acute or subacute
Further specify with bronchiectasis, COPD, etc.
Allergic
Asthmatic
Chronic
Obstructive
Viral
38
Diabetes Mellitus
ICD-9 features 59 codes for diabetes, while
ICD-10 offers more than 259 and adds a provision of “poorly controlled” to categories of controlled or not controlled.
Diabetes mellitus codes expanded to include the classification of the diabetes AND the manifestation.
Needs to be clearly documented in the record!
39
More on Diabetes
Identify Type 1, Type 2, due to other secondary cause, i.e., gestational, etc.
In Type 2 or secondary cause, identify when using insulin long-term.
Identify all body systems affected by the diabetes, i.e., neuropathy and its manifestation, retinopathy and proliferative or nonproliferative, nephropathy and stage of CKD, vasculopathy, etc.
Identify all manifestations, i.e., ulcer, coma, gangrene, osteomyelitis, etc.
40
Chest Pain
Medical record documentation must include the specific location of the chest pain:
Anterior wall
Atypical
Intercostal
Musculoskeletal
Non-cardiac
Precordial
41
Fracture Documentation
Documentation will need to include the following to accurately code a fracture in ICD-10-CM:
Displaced or non-displaced
Open or closed
Laterality (left vs. right vs. bilateral)
Specific bone and location of the bone
Distal, proximal, mid-shaft, etc.
Type of Encounter
Initial, subsequent, sequela
42
Fracture “Subsequent”
Encounter
Subsequent encounter for open and closed fractures:
Used for encounters after active fracture treatment has been completed and the patient is receiving routine care during the healing or recovery period.
Closed Fracture 7 th Character Extensions:
D ► Routine healing or aftercare
G ► Delayed healing
K ► Nonunion
P ► Malunion
43
What is Gustilo-Anderson Scale?
Gustilo-Anderson classification identifies the ‘ severity of soft tissue damage ’ in open fractures – may be new to coders and physicians:
Type I : Wound is smaller than 1 cm, clean, and generally caused by a fracture fragment that pierces the skin (low energy injury)
Type II : Wound is longer than 1 cm, not contaminated, and w/o major soft tissue damage or defect (low energy injury)
Type III : Wound is longer than 1 cm, with significant soft tissue disruption. The mechanism often involves highenergy trauma, resulting in a severely unstable fracture with varying degrees of fragmentation.
44
Hernias
Specify location, i.e., inguinal, femoral, umbilical, ventral, diaphragmatic; all other abdominal hernias default to “other”, etc.
Specify unilateral (which side) or bilateral
Specify with obstruction when present
Specify with gangrene when present
Specify when recurrent hernia (defaults to primary)
45
Malignancy Example
Malignant Neoplasm Breast
54 choices for male/female breast
Documentation must include:
Laterality
Location (site)
Use of an additional code to identify estrogen receptor status
Example: C50.422 (Malignant neoplasm of upper-outer quadrant of the left male breast)
46
And Another…
Malignant Neoplasm Lung/Bronchus
63 choices available in ICD-10-CM
Documentation must include:
Specific site/location
Hilus, lingula, main bronchus, lower lobe, middle lobe, upper lobe, etc.
Example: C34.2 (malignant neoplasm of middle lobe, bronchus or lung)
Laterality
Physician Practices
ICD-10-CM diagnosis codes will impact every physician practice large or small!
Look at all areas that will impact your practice and identify each one that will be affected:
Practice Management System
Electronic Medical Record (EMR)
Paper record
Superbill/encounter form – does it have diagnosis codes on it?
Lab requisitions/orders
48
Task Is Not As Huge
As It Appears!
Although the coding book is “huge”, many physician practices use only a small set or # of diagnosis codes.
Start developing crosswalks between ICD-9-
CM & ICD-10-CM codes you use most frequently in the office.
49
That’s ICD-10!
50
Contact Info:
Karen Kvarfordt, RHIA, CCS-P, CCDS
AHIMA Approved ICD-10-CM/PCS Trainer
President, DiagnosisPlus, Inc.
PO Box 486
Pocatello, ID 83204
(208) 221-5486 diagnosisplus1@live.com
51