Acid Base
advertisement

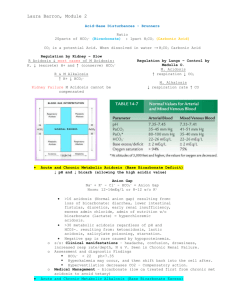
Acid Base Heather Wacholz TCCC Acid-Base Balance (pH) Acid—substance containing hydrogen ions that can be liberated or released Base—substance that can trap hydrogen ions Homeostasis Major Homeostatic Regulators of Hydrogen Ions Buffer systems Carbonic acid–sodium bicarbonate Phosphate Protein Respiratory mechanisms Renal mechanisms Hydrogen Ion Balance Homeostatic Mechanism Plasma pH is an indicator of hydrogen ion (H+) concentration Measures the acidity or alkalinity of the blood Homeostatic mechanism keep pH within normal range (7.35-7.45) The buffer system is the kidneys and lungs The H+ is extremely important The greater the concentration the more acidic the solution therefore the lower the pH and the less the concentration the higher the pH and the more alkaline. Normal values Arterial Blood pH 7.35 7.45 Normal PCO2 Arterial Blood PCO2 35 45 mmHg mmHg Normal PO2 Arterial Blood PO2 80 mmHg 100 mmHg Normal PO2 Arterial Blood HCO3- 22 mEq/L 26 mEq/L The Kidney and Lung Help Regulate pH Role of Lungs The lungs control the CO2 The lungs control the carbonic acid of the extracellular fluid (ECF) This works by adjusting the ventilation in response to the level of CO2 in the blood For example: A patient with a PCO2 80 mmHg (Arterial Blood Gas) may breathe 40 breaths per minute to remove the high CO2. Role of the Kidney The kidneys regulate the bicarbonate level in the ECF The kidney can regenerate or reabsorb bicarbonate During respiratory acidosis and most cases of metabolic acidosis the kidneys excrete H+ ions and conserve HCO3- to help restore balance During respiratory alkalosis and metabolic alkalosis the kidneys hold onto H+ ions and excrete HCO3 If the patient is in renal failure the kidneys can not compensate for acidosis Acid-Base Imbalances Occur when carbonic acid or bicarbonate levels become disproportionate Respiratory acidosis—primary excess of carbonic acid in ECF Respiratory alkalosis—primary deficit of carbonic acid in ECF Metabolic acidosis—proportionate deficit of bicarbonate in ECF Metabolic alkalosis—primary excess of bicarbonate in ECF Tests for Monitoring Acidosis and Alkalosis Monitor with Arterial blood gas (ABG) Monitor with Venous blood gas (VBG) Monitor with Capillary blood gas (CBG) Causes of Metabolic Acidosis and Manifestations Direct loss of HCO3Diarrhea, diuretic use, early renal insufficiency, excessive administration of chloride, Headache, confusion, drowsiness, increased respiratory rate, nausea, and vomiting Example ABG Displaying Metabolic Acidosis Treatment of Metabolic Acidosis Correcting the imbalance Bicarbonate is administered Eliminating chloride With the reversal of acidosis the patient may go from hyperkalemia to hypokalemia (the K+ moves back into the cell as the acidosis corrects) Example the diabetic ketoacidosis patient. Monitor serum K+ level closely With chronic metabolic acidosis treat calcium level first Causes of Metabolic Alkalosis and Manifestations A common cause is gastric suctioning, vomiting, pyloric stenosis, diuretics that promote the excretion of potassium, excessive antacid abuse, and ACTH excretion The kidneys conserve K+ and H+ excretion increases; K+ leaves the cell and H+ enters to try and maintain balance Symptoms of decreased Ca+ ionization, tingling of fingers and toes, dizziness, hypertonic muscles Sometimes decreased respirations Tachycardia Symptoms of chronic the same as acute Example of ABG Metabolic Alkalosis Causes of Respiratory Acidosis and Manifestations Inadequate secretion of CO2 This can cause a decrease in oxygen levels too Symptoms include elevated HR, RR, elevated BP, and VF Confusion Increased ICP Patient's with chronic COPD may not develop symptom of high CO2 because of compensated renal changes Example of Respiratory Acidosis Treatment of Respiratory Acidosis Improve ventilation Bronchodilators and antibiotics Blood thinners if cause of acidosis PE Mechanical ventilation (Intubate patient) Decrease CO2 slowly because the kidneys can not excrete Bicarbonate too quickly Treatment the same for chronic Causes of Respiratory Alkalosis and Manifestations Hyperventilation Extreme anxiety, hypoxemia, early stage of ASA overdose Gram negative bacteria, inappropriate ventilator settings Symptoms include lightheadedness, numbness and tingling of fingers and toes Decreased ability to concentrate Loss of consciousness Tachycardia Example ABG of Respiratory Alkalosis Treatment for Respiratory Alkalosis Monitor electrolytes Treat the underlying cause Instruct the patient to breath slower; give the patient a paper bag to breath in If the cause is anxiety get an order for Xanax or Ativan When You Think of CO2 •Monitor pH LUNGS CO2 •Look at CO2 When you Think of Bicarbonate •Monitor pH Kidneys HC03- •Look at HC03- Alkalosis and Acidosis Five Step Approach 1) First note the pH is it normal, high, or low 2) Next note the primary cause of problem. This is done by evaluating the PaC02 and HCO3- in relation to pH 3) Next look at compensation 4) This means if the patient has both respiratory and metabolic alkalosis or acidosis 5) If metabolic acidosis occurs calculate anion gap (AG) to determine the cause What is AG? This test looks at electrically charged particles in your blood to help your doctor diagnose acid-base imbalances. The test results are calculated from the results of an electrolyte panel, another blood test. The value for the anion gap tells your doctor something about which charged particles besides sodium, chloride, and bicarbonate ions must be in your blood to make it neutral. This test gives clues about different types of acidosis, when your blood is too acidic; and alkalosis, when your blood is not acidic enough. Acidosis in particular can be life-threatening, so it's important to find the cause and treat it as soon as possible Calculating AG AG = Na – (CL + HC03- ) Normal AG = 10 to14 mmol/L For example patient Na = 140, CL = 105 and HC03- = 25 AG = 140 – (105 + 25) = 10 so this would be a normal AG References Hinkle, J. L., & Cheever, K. H. (2014). Brunner & Suddarth's textbook of medical-surgical nursing. Bethlehem, Pennsylvania: Wolters Kluwer/Lippincott Williams & Wilkins. University of Rochester Medical Center. (2015, January 19). Retrieved from http://www.urmc.rochester.edu/encyclopedia/content.aspx?ContentTypeI D=167&ContentID=anion_gap_blood