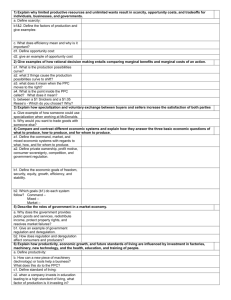
3 Basic Steps in Economic Evaluation
advertisement

Chapter 1: Introduction Health Economics Can we apply the tools of economics to study the health care sector? Outline The 4 basic questions of health economics. The production possibilities curve Economic models Positive and normative analysis Net Benefit calculus The following slides summarize material in Santerre & Neun, Health Economics: Theories, Insights and Industry Studies, Dryden, 2000. Health Economics …studies the supply and demand of health care resources and the impact of health care resources on a population. (Mosby Medical Encyclopedia 1992, p. 361) The 4 Basic Questions 1) What combination of nonmedical and medical goods and services should be produced in the macroeconomy? a) Should the federal government spend more on missile defense or to reduce the number of uninsured children? b) Should the federal government spend more on education or prescription drugs for the elderly? The 4 Basic Questions (cont.) 2) What particular medical goods and services should be produced in the health economy? a) b) Should the federal government spend more on prescription drugs for the elderly or on home health care? Should the federal government spend more on research to cure cancer or on cancer screening programs? The 4 Basic Questions (cont.) 3) What specific health care resources should be used to produce the final medical goods and services? a) b) 4) Should more ambulatory patients be cared for by nurse practitioners instead of physicians? When is medical vs. surgical management of a health condition appropriate? Who should receive the medical goods and services? The 4 Basic Questions (cont.) 4) Who should receive the medical goods and services? a) b) Should all of the elderly receive prescription drug coverage from the federal gov’t, or only the low-income elderly? Should illegal immigrants receive free care in county clinics and hospitals? The Production Possibilities Curve (PPC) A framework for answering the 4 basic questions. Depicts the availability of resources and indicates what can be produced. A PPC for the Federal Gov’t: National Defense vs. Health Care Full-proofness of the U.S. against terrorist attacks 100% Points outside the PPC are not achievable with current technological know-how. Points inside the PPC represent production inefficiency 100% % of Children covered by health insurance A PPC for the Federal Gov’t (cont.) The federal gov’t must make tradeoffs. more on health insurance spending less on defense Tradeoffs the PPC slopes downwards. Spending Tradeoffs imply opportunity costs. The value resources would yield if they were put to an alternative use. The opportunity cost of raising health insurance coverage by 1% could be a 2% reduction in the number of armed forces trained to deal w/ terrorist attacks. A PPC for the Federal Gov’t (cont.) Resources are allocated optimally if the value obtained from a particular expenditure (e.g. raising health insurance coverage by 1%) is greater than its opportunity cost. Who’s value? In this case, one must come up with a valid measure of “society’s value”… A PPC for the Federal Gov’t (cont.) Resources are imperfectly substitutable Each additional unit of production has a rising opportunity cost. • e.g. Raising health insurance coverage from 10 to 20% may reduce the fullproofness of the U.S. defense system from 95% to 94%. But raising insurance coverage from 90% to 100% could reduce the readiness of the U.S. defense system from 10% to 0%. The PPC is concave. A PPC for the Federal Gov’t (cont.): National Defense vs. Health Care Full-proofness of the U.S. against terrorist attacks 100% Identical increases in health insurance coverage require larger reductions in defense readiness as more resources are devoted to insurance. 100% % of Children covered by health insurance A PPC for the Federal Gov’t (cont.) All points on the PPC are efficient, and the point which is chosen will depend on society’s preferences. But is the optimal point “fair”?? To the poor? To those who would die in a terrorist attack? A PPC for the Federal Gov’t (cont.) As we will see in this course, market competition often leads to an efficient allocation of resources. However, a society which is also concerned with equity can redistribute resources, often using taxation. However, taxation leads to inefficiencies. A tradeoff often exists between efficiency and equity. Economic Models “Models are abstractions of reality and are used in economics to simplify a very complex world.” Usually describes a hypothesized relation between two or more variables. Can be expressed in verbal, graphical, or mathematical form. Economic Models (cont.) Example: We hypothesize that health care expenditures are dependent upon an individual’s income. • E = f(Y) In stating this hypothesis, we assume that all other likely determinants of E (e.g. prices, tastes, preferences) stay constant. Economic Models (cont.) • We can hypothesize that health care expenditures are linearly related to income. E = a + bY a = expenditures if income is zero. b = slope of the expenditure function. b = E/Y Economic Models (cont.) • We can quantify the linear relation between income and health expenditures. E = 1000 + .1Y $1000 = expenditures if income is zero. • Each $1,000 increase in consumer income raises health care expenditures by .1*(1000) = $100. Annual health care expenditures per household ($1000's) (E) Health Care Expenditure Function: E=1000+.1Y 8 7 6 5 4 3 2 1 0 0 10 20 30 40 50 60 Yearly income per household ($1000's) (Y) Economic Models (cont.) • The economic models states that ceteris paribus, E=1000 + .1Y. • We can incorporate changes in other factors into the model as well. • Suppose that the population has aged, so that yearly medical costs rise by $500 for the typical household. Economic Models (cont.) • We respecify the model as: E = 1500 + .1 Y • In our graphical representation of the model, this represents a shift up in the entire health care expenditure function. Annual health care expenditures per household ($1000's) (E) A Shift in the Health Care Expenditure Function: 8 7 6 E1 = 1500 + .1Y 5 4 3 E0 = 1000 + .1Y 2 1 0 0 10 20 30 40 50 60 Yearly income per household ($1000's) (Y) •We will rely on the results of multiple regression analysis to quantify models like this in this course. Positive and Normative Analysis Positive analysis makes statements or predictions regarding economic behavior. What is? What happened? Normative analysis deals with the appropriateness or desirability of an economic outcome or policy. What ought to be? Which is better? Positive and Normative Analysis (cont.) According to Becker and Murphy (1988), a 10% increase in the price of cigarettes leads to a 6% reduction in the number of cigarettes consumed. The government should increase the tax on cigarettes to prevent people from smoking. Positive and Normative Analysis (cont.) It is in our country’s best interests that the federal government take a more active role in the prevention of AIDS. A study by Hellinger (1991) estimates that the average yearly cost of treating someone with AIDS is $38,300, while the lifetime costs equal $102,000. Positive and Normative Analysis (cont.) To control health care expenditures, the United States should adopt a national health insurance program similar to Canada’s. National health care expenditures per capita in the U.S. equaled $4,094 in 1998. The Net Benefit Calculus Economic models assume that individuals are rational. People can rank their preferences from high to low, or best to worst. People never purposely choose to make themselves worse off. If expected benefits>expected costs for a given choice, it is in the agent’s best interest to make that choice. The Net Benefit Calculus (cont.) NB*(X) = B*(X) – C*(X) X = choice or activity under consideration NB* = expected net benefits B* = expected benefits C* = expected costs B*(X) = Pr(X)•B(X) 1Pr(X)0 The Net Benefit Calculus (cont.) Health care providers, government agencies, and individual consumers use such cost-benefit analysis to make decisions. Explicitly or implicitly. Conclusion Because resources are limited, health economists are concerned with determining what medical services to produce, how they should be produced, and who should receive them. As we will see in this course, the tools of economics can be applied to the health care sector to derive valuable insights about our health care system. Industry Overview Health Economics Health Care Expenditures in the United States, 1960-2001 1960 1970 1980 1990 1995 1999 2001* Nominal health expenditures (billions of dollars) $26.9 73.2 247.3 699.4 987.0 1210.7 1424.2 Annual rate of growth (average annual % change from previous period shown) Nominal per capita health expenditures -- 10.6% 12.9 10.9 6.7 5.2 8.4 $143 341 1,052 2,690 3,686 4,358 5,043 Health expenditures as percentage of GDP 5.1% 7.1 8.9 12.2 13.3 13.0 13.4 *Projected Source: Health Care Financing Administration Homepage: http://www.hcfa.gov/stats/stats.htm The Health Care Industry is Rapidly Evolving. Advances in medical technology and drugs are dramatically improving patient care. But, these improvements are costly. Aging U.S. population. % 65 years+ 1950 8.1 1970 9.8 2000 12.7 The Health Care Industry is Rapidly Evolving. Increased cost containment efforts. Changes in government reimbursement of health care providers. Private insurers are exercising more control over patient care. Increased competitive pressures. Mergers of existing providers. Entry of new competitors. Where are the most promising business opportunities? HOSPITAL CARE 32% of all health care expenditures in 1999. But insurers moved from cost-based reimbursement to fixed price reimbursement in the 1980’s. Slower revenue growth In order to attract patients, many hospitals overspent on high-tech equipment. HOSPITAL CARE Improved surgical techniques led to shorter stays in hospital after surgery, more outpatient surgery. Lower demand for hospital beds and operating room time. 1998 community hospital occupancy rate = 62.5% A glut of hospital beds and high-tech services has led to too many hospitals competing for too few patients. NYT 10/25/96 Modern Healthcare 2/8/99 If hospital revenues are shrinking, which sectors of the industry are growing? America’s Top 100 Fastest-Growing Companies FORTUNE, September 4, 2000 100 RANK 16 23 COMPANY VISX EPS GROWTH REVENUES (millions) RATE 100% $266.8 78% $1968.4 WHAT THEY DO Holds 150 patents for laser technology, charges a perprocedure licensing fee. Prescription-drug benefit 23 Advance Paradigm Forest 105 % $959.9 Licenses drugs developed by other companies & markets them. 28 Minimed 71% $252.1 30 Polymedica 48% $156.9 30 Sunrise 124% $280.6 Infusion pump worn like a pager for diabetes patients to avoid injections. Sells diabetes-testing equipment to seniors covered by Medicare. Assisted Living Homes Laboratories manager Assisted Living 69 Biogen 60% $881.1 Biotech drug company, leader in MS drugs. 92 Impath 38% $99.0 Collects and interprets Cancer data PHARMACEUTICAL INDUSTRY U.S. prescription drug expenditures reached $99.6b in 1999. Industry highly dependent on research and development (R&D). $300m to bring a new drug to market. Aggressive marketing to physicians, hospitals, pharmacists, and even the patient. PHARMACEUTICAL INDUSTRY Merck $40.4b in sales in 2000 50% of sales come from Merck-Medco (pharmaceutical benefits management) 50% of human health sales come from 5 drugs: Vioxx, Zocor, Fosamax, Cozaar/Hyzaar, and Singulair WSJ 2/10/99 MANAGED CARE Systems which manage the quality and cost of patient care. Most common: Health Maintenance Organization (HMO) Consumer pays a fixed annual capitation fee, for which HMO agrees to provide comprehensive medical services. 60% of U.S. population (66.8m) enrolled in 2000. MANAGED CARE ADVANTAGE: If capitation fee > costs, HMO keeps the profit. DISADVANTAGE: HMO responsible for cost overruns. Subject care. to lawsuits if provides sub-optimal WSJ 2/17/98 Integration and Disintegration On One Hand... Between 1995 and 1998, over 2,800 hospitals were involved in mergers, acquisitions, joint ventures, long-term leases, and other partnerships. Hospital Consolidation Trends 1,000 750 768 735 687 627 Facilities Involved Number of Deals 500 250 230 235 217 198 0 1995 1996 1997 1998 Source: Modern Healthcare. January 11, 1999. “Deals” include mergers, acquisitions, joint operating companies, joint ventures, long term leases, and system affiliations. On the Other... Who? – – – – Allegheny Health, Education and Research Foundation (AHERF) At Their Peak… Today… 345 hospitals throughout the U.S. $20B in annual revenue $1B in annual home-health revenue Acquires Value Health (pharmacy, IT, managed care services) for $1B Sells off hospitals en masse in an attempt to extinguish nearly $9B in debt Sells off nearly all non-hospital businesses – 13 acute-care hospitals throughout Pennsylvania and in New Jersey – St. Christopher’s Children’s Hospital – Allegheny University of the Health Sciences, including Medical College of Pennsylvania July 1998, filed for Chapter 11 protection owing creditors over $1.5B Philadelphia hospitals sold to Tenet Pittsburgh hospitals to Western Pennsylvania Healthcare System – Over 7,500 physicians, with locations in 25 states – $3.5B in net revenue $1.2B net loss in 4Q 1998 Merger with PhyCor falls through March 1999, California regulators seize physician operations in the state September 1999, renamed Caremark Rx reflecting new focus on pharmaceutical services; 12 physician practices remain – Over 1.5M enrolled members – $176.5M in earnings on $3.1B in net revenue in 1996, increases of 90 and 75 percent over 1995, respectively – Rated #1 in customer satisfaction in NY for HMO and POS products Computer glitch leads to nearly $1B in losses in 1997-1998 Subpoenaed by the SEC and New York state earlier this year to “review market conduct” LONG-RUN KEY TO SURVIVAL Be an efficient provider of highquality patient care.