posgh - ashrae level 2 energy audit report
advertisement

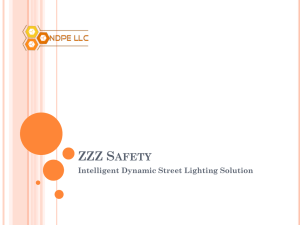
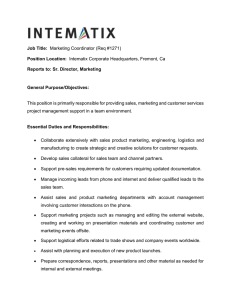
ASHRAE LEVEL 2 ENERGY AUDIT REPORT PORT-OF-SPAIN GENERAL HOSPITAL NORTH BLOCK November 8, 2013 SMART ENERGY LIMITED TABLE OF CONTENTS List of Abbreviations.....................................................................................................................................3 1.0 Executive Summary.........................................................................................................................4 2.0 Background.....................................................................................................................................6 3.0 2.1 Space Types........................................................................................................................6 2.2 Occupancy Use and Schedules............................................................................................6 2.3 Recent Building Upgrades...................................................................................................6 2.4 Billing Data..........................................................................................................................7 2.5 Baseline Energy Consumption............................................................................................8 Audit Activity and Results..............................................................................................................10 3.1 4.0 Audit Process....................................................................................................................10 3.1.1 Data Collection and Measurements....................................................................10 3.1.2 Calculation Methodology.....................................................................................10 3.2 Existing Building Systems..................................................................................................11 3.3 Renewable Energy Assessment........................................................................................15 3.4 Energy Conservation Opportunities..................................................................................16 Operational and Behavioral Guidelines.........................................................................................22 Appendix A – Site Plan...............................................................................................................................25 Appendix B – Floor Plans............................................................................................................................26 Appendix C – Lighting Survey.....................................................................................................................27 Appendix D – Air Conditioning Survey.......................................................................................................28 Appendix E – Measurements and Envelope...............................................................................................29 Appendix F – Equipment Survey................................................................................................................30 Appendix G – Spot Measurements.............................................................................................................31 Page | 2 LIST OF ABBREVIATIONS AC – Air Conditioning ASHRAE – American Society of Heating, Refrigerating, and Air Conditioning Engineers CFM – Cubic feet per minute CO2 – Carbon dioxide ECM – Energy Conservation Measure ENT – Ears, Nose, and Throat HVAC – Heating, Ventilation, and Air Conditioning IAQ – Indoor Air Quality kWh – kilowatt-hour kVA – kilovolt-ampere NB – North Block NWRHA – North West Regional Health Authority OSHA – Occupational Safety and Health Administration POSGH – Port of Spain General Hospital PPM – Parts per million SEL – Smart Energy Limited T8 – Second generation tubular fluorescent lamp with 1” diameter T12 – First generation tubular fluorescent lamp with 1.5” diameter Page | 3 1.0 EXECUTIVE SUMMARY The Port-of-Spain General Hospital (POSGH) is a healthcare facility owned by the Trinidad and Tobago North West Regional Health Authority (NWRHA) and is responsible for providing health care services to the citizens of Trinidad and Tobago. A Level 2 ASHRAE Energy Audit was performed on the North Block (NB) of the POSGH campus by Smart Energy Limited (SEL) in September 2013 to identify cost effective energy conservation measures and operational improvements that would help POSGH reduce its energy consumption. In 2012, POSGH’s total energy consumption was 8.5 million kWh with consistent energy consumption on a month to month basis throughout the year. The estimated energy consumption for the NB is 1.7 million kWh. Most of the energy consumption was due to air-conditioning (59%), followed by lighting (24%), and hospital equipment (18%) ranging from computers to radiology machines. The NB has two stories and houses the following hospital departments: Main Radiology Department, Physiology Department, ENT Theater, Eye Theater, Eye Clinic, and six wards. All the departments are airconditioned except for the wards. The Physiology Department was recently rehabilitated, while work was under way to convert one ward to a Hemotherapy Department. The building envelope is in poor condition, with gaps and holes in doors and broken windows, allowing for great air infiltration. The airconditioning system is served by both central package systems and several split air-conditioning systems from different manufacturers. Lighting was mixed between older T12 fixtures and newer T8 fixtures. Several of the T12 fixtures were burned out and need replacing. It was also observed that exterior corridor lighting was operating day and night and was controlled by a switch. SEL surveyed all the lighting, air-conditioning, controls, electrical equipment, and mechanical equipment to identify the area of greatest waste in energy consumption. It was determined that the greatest source of waste was due to the usage of outdated lighting technology, lack of awareness of energy conservation, and building envelope issues leading to a great deal of air infiltration. POSGH was originally designed for passive energy systems and the building envelope was not properly updated, when active systems were installed. Recently, the building envelope for the Physiology Department was improved to correct this issue, along with the installation of new central packaged air-conditioning units and ducts to provide ventilation to the spaces for improved indoor air quality. The ducts were not insulated and weatherproofed though and are already being degraded by the climate conditions in Trinidad. The greatest energy savings may be obtained from the upgrade of lighting to more efficient T8 technology, installation of controls to regulate lighting operation, and the improvement of the building envelope by sealing leaks. SEL did not identify any cost-effective renewable energy measures that could be undertaken. A summary of the recommended ECMs may be found in the table on the next page. This table was obtained from ASHRAE and all cost savings are in US$. The measure life is how long we expect a measure to last once implemented before a replacement or update is needed. Page | 4 POSGH North Block ECM Summary Table Annual Energy and Cost Savings Measure Number ECM-1 ECM-2 ECM-3 ECM-4 ECM-5 ECM-6 ECM-7 ECM-8 ECM-9 ECM-10 ECM-11 ECM-12 ECM-13 ECM-14 Measure Description Replace all T12 fixtures with new T8 fixtures Peak Demand Savings (kW) 15.7 Electricity Savings (kWh) 148,298 Gas/Fuel Savings (therms) - Delamp 4-lamp T8 fixtures and install (2) T8 lamps 1.2 10,818 with high ballast factor and reflectors Replace outdoor lighting fixtures with 70W 1.6 16,031 photocell controlled LED wallpacks Replace incandescent lamps with compact 0.3 2,593 fluorescent lamps Install astronomical time clocks in high traffic 109,727 areas with fixed schedules and external corridors Install occupancy sensors in low traffic areas with 6,588 low occupancy such as locker rooms or kitchens Install indoor photo sensors in areas with much 25,093 natural lighting for daylight harvesting Program programmable thermostats for packaged 5,000 AC units for night time and weekend setback. Increase setpoint temperatures on split and 5,000 packaged AC units Install door thresholds for all external doors of air 20,000 conditioned rooms Replace hollow core doors with solid core doors for 20,000 all exterior doors of air conditioned rooms Readjust sensor over sliding door leading to X-Ray 1,500 reception Air sealing of building envelope where leaks are 120,000 present in windows, doors, and walls Central duct HVAC system with humidity control to Level 3 Req Level 3 Req Level 3 Req replace all split units TOTALS (Recommended Measures) 18.8 490,648 - Payback with Incentive Total Cost Savings $ 6,484 Measure Cost Potential Utility Incentive Measure Life (years) Simple Payback (yr) $ 22,710 $ - 10 3.5 $ 474 $ 1,645 $ - 10 3.5 $ 690 $ 2,800 $ - 10 4.1 $ 88 $ 32 $ - 3 0.4 $ 3,539 $ 2,200 $ - 5 0.6 $ 223 $ 500 $ - 5 2.2 $ 1,500 $ 849 $ - 5 0.6 $ 170 $ - $ - 1 - $ 170 $ - $ - 1 - $ 680 $ 1,000 $ - 5 1.5 $ 680 $ 3,000 $ - 10 4.4 - $ - 5 - 4,080 $ - $ 51 $ $ 3,080 $ Level 3 Req $ 17,829 700-900k $ 38,816 NA $ 1.3 NA NA - 2.2 Disclaimer: The information, calculations, analyses and conclusions included in this report have been provided by the auditing company and solely reflect its findings. Neither the funding Inter-American Development Bank (IDB) nor CAD as contracting authority assume responsibility for the accuracy or completeness of the contents of this report, and expressly disclaim liability for errors and omissions. Page | 5 2.0 BACKGROUND The Port-of-Spain General Hospital is owned by the Trinidad and Tobago North West Regional Health Authority (NWRHA) and is responsible for providing health care services to the citizens of Trinidad and Tobago. The hospital is located near the downtown area of Port-of-Spain and consists of several buildings on one campus. The scope of this energy audit is the NB which houses the ENT Theatre, Eye Theatre, Eye Clinic, Main Radiology Department, wards, and the Physiotherapy Department. The NB was originally constructed in 1936 and had air-conditioning systems added in the 1960s. The building has two stories above grade with external corridors. The building length is oriented toward the north. The total area of the NB is 5,530 m². 2.1 Space Types The ground floor of the NB houses the Main Radiology Department and Physiology Department while the first floor houses the ENT Theater, Eye Theater, and Eye Clinic. Both floors house the Wards, which encompasses the East side of the building. NB Space Types (m²) Floor Air-conditioned Spaces Nonconditioned Wards Non-conditioned Corridors/Small Rooms Total Ground Floor 1,477 571 1,091 3,139 First Floor 568 584 1,241 2,393 Totals 2,045 1,155 2,332 5,532 2.2 Occupancy use and schedules The operating hours for the NB are generally 8:00 am to 4:00 pm on weekdays, with some weekend operations as well. It is mainly used as a day clinic with the main departments being the Eye Clinic, Radiology, and ENT Theater. Only Ward 16 operates past 4:00 pm. While performing the building audit, we observed that most rooms were vacant by 4:00 pm. There is an average of 68 staff members at this site and 434 patients per day. 2.3 Recent Building Upgrades The NB is currently undergoing renovation to update several areas, but this is being done to improve the hospital’s service offerings and not for energy efficiency. Recently, they gutted and rehabilitated the Physiotherapy Department installing new ductwork and a packaged air-conditioning unit with a digital thermostat. Although the room is currently unoccupied due to construction, we observed the AC unit was operating. Ward 2 is currently being renovated as well to be converted to the Hemotherapy Department Page | 6 Figure 1. Physiotherapy Department with new ductwork Figure 2. Temperature in the Physiotherapy Department while unoccupied (°F) 2.4 Billing Data A breakdown of POSGH annual energy consumption from December 2011 until May 2013 is shown in Table 1 below: POS General Hospital Month kWh 2011 2012 2012 2013 December January February March April May June July August September October November December TOTAL January February March April May 672,600 657,400 606,600 670,800 679,300 732,900 No Data 736,200 740,100 729,600 776,300 754,400 747,000 8,503,200 723,200 646,700 732,500 743,000 803,100 Energy Charge (TT$) kVA kVA Demand Shortfall 146,626.80 143,313.20 132,238.80 146,234.40 148,087.40 159,772.20 No Data 160,491.60 161,341.80 159,052.80 169,233.40 164,459.20 162,846.00 1,853,697.60 157,657.60 140,980.60 159,685.00 161,974.00 175,075.80 1,498 1,438 1,441 1,482 1,565 1,546 No Data 1,564 1,529 1,657 1,717 1,701 1,592 1,561 1,589 1,532 1,637 1,630 1,673 0 0 0 0 0 0 No Data 0 0 0 0 0 0 0 0 0 0 0 0 Demand Charge (TT$) 74,900.00 71,900.00 72,050.00 74,100.00 78,250.00 77,300.00 No Data 78,200.00 76,450.00 82,850.00 85,850.00 85,050.00 79,600.00 936,500.00 79,450.00 76,600.00 81,850.00 81,500.00 83,650.00 Total (TT$) Bill 255,813.82 248,553.18 235,990.12 254,442.56 261,346.01 273,691.03 No Data 275,553.34 274,518.57 279,246.22 294,403.91 287,993.58 279,870.90 3,222,481.24 273,731.74 251,275.69 278,823.25 281,053.10 298,592.67 A billing analysis was conducted for this site using the above billing data. The electric rate for the POSGH is US$0.035 per kWh and US$8.00 per kVA. The hospital is charged for its demand every month Page | 7 instead of their reserve capacity of 1,290 kVA since they have exceeded it every month and do not have a shortfall. We were not able to obtain the billing data for June 2012, which is the reason for gap shown in the chart below. The billing data that SEL has received was for the entire hospital campus, rather than just the NB based on the total floor space of this block, the area of air-conditioned spaces, and the equipment surveyed. The resulting energy intensity for the NB would be extremely high at 1,500 kWh per square meter and unusual for a hospital this size, even if it was inefficient, if the billing data received was for the NB only. Daily Energy Consumption - Entire Hospital 30,000 kWh/day 25,000 20,000 15,000 10,000 5,000 2012 2013 0 For the entire hospital, the energy consumption increased by almost 3,000 kWh per day in 2013 versus 2012. This may be due to the addition of the packaged air-conditioning system in the Physiotherapy Room. 2.5 Baseline Energy Consumption The end use energy consumption for the POSGH NB is shown in the table below and is based on a survey of the AC systems, lighting systems, control systems, hospital equipment, site measurements, billing analysis, and interviews conducted with site staff. Based on our survey of AC equipment, the building type, and our observations, we assumed the AC was running 24/7. We were able to confirm in staff interviews that the major AC systems which comprise over 60% of the total cooling energy consumption do run 24/7. The lighting load was determined from the various lighting fixtures in place and their estimated operating hours. The hot water energy consumption was based off the number of hot water heaters and their estimated energy consumption per year. Page | 8 Port-of-Spain General Hospital NB End Use End Use Annual Electricity (kWh) % Total Use Cost (USD) 1,000,000 59 36,333.33 Domestic Hot Water 10,000 1 363.33 Lighting 406,000 24 14,751.33 Hospital Equipment & Plug Loads 274,500 16 4,959.60 1,690,500 100 56,407.59 Space Cooling Totals A breakdown of POSGH’s energy consumption is shown in the pie chart below. Water Heating 1% Other Plug Loads 16% Lighting (Interior) 22% Cooling 59% Lighting (Exterior) 2% As expected, the greatest end use for POSGH NB is cooling, followed by lighting, and plug loads. Great savings may be obtained with simple measures related to building envelope improvements, and cooling as well as lighting measures which will be discussed later. The total infiltration, which is the air leakage into the hospital, for the NB was estimated to be 430,000 kWh annually. This figure was arrived at by calculating latent and sensible heat gains based the on condition of envelope, air changes per hour, volume of space, and design dry bulb temperature. Page | 9 3.0 AUDIT ACTIVITY AND RESULTS 3.1 Audit Process This section will detail our onsite data collection, measurements, calculation methodology, analyses and assumptions. 3.1.1 Data Collection & Measurements Prior to the site visit, SEL was given preliminary findings and over one year of billing data for the Port-ofSpain General Hospital. The energy audit was conducted in September of 2013 and detailed information was collected including: nameplate information of all AC units (when possible), the quantity and type of all lighting fixtures, building controls, survey of hospital equipment, building operating hours, building occupancy schedules, and building envelope properties. Spot measurements were also taken at the electrical panels that serve the AC, lighting, and hospital equipment during typical work hours. We took these measurements in order to get an idea of the various equipment loads and an idea of the total power demand. While installing data loggers for a period of two weeks to one month is preferable to determine the building’s typical energy consumption patterns, we were unable to do so due to time constraints. In addition, we interviewed building staff to determine operating and maintenance procedures, as well as gather information on recent and future renovations being undertaken by the hospital. 3.1.2 Calculation Methodology Cooling The nameplate information and associated run times were collected for all HVAC units. The baseline energy consumption has been determined by current operating schedules for the AC units and their associated loads. Due to the current HVAC system in place, an ASHRAE Level 3 audit is recommended for a whole building simulation analysis to determine the energy savings associated with removing all the split and unitary air conditioning units and replacing them with a central chiller plant. Lighting The quantity, types, and operating hours of all lighting fixtures were collected. The baseline power demand was determined by using standard fixture wattages for the existing equipment and the recommended energy efficient equipment. Operating hours will also be estimated based on current operating strategies and for controls, standards will be used for the reduction in operating hours. Building Envelope Recommendations will be made on potential building envelope upgrades to address infiltration. A whole building computer simulation is necessary to determine energy savings associated with general building envelope improvements such as new fenestration and is outside the scope of an ASHRAE Level 2 Energy Audit. Therefore an ASHRAE Level 3 Energy Audit is recommended. Page | 10 3.2 Existing Building Systems Below are descriptions of the existing building systems. Cooling The NB is served by a combination of packaged air-conditioning units, split systems, and window units to meet its cooling demands. While the split systems and window units had varying make and models, the larger packaged units were typically made by Carrier. The packaged units typically served one hospital department, such as the Eye Clinic, while the split systems and window units served one room. About 1/3rd of the total floor area of the Block is conditioned (when external corridors are taken into account). (20) Split systems and window units along with five packaged units were counted. A number of issues were encountered with the cooling equipment and distribution system including: Most of the ductwork for the packaged units is running outdoors and is exposed to direct sunlight and the elements, and damage and leaks were visible in many places. The condenser coils on many condensers were either flattened or badly deteriorated resulting in inefficient heat transfer. The insulation to the refrigerant lines is in bad repair also resulting in unnecessary energy consumption. Due to the condition of the building envelope and the air-conditioning system installed, the relative humidity was too high in most spaces that were measured. There are a number of condensing units installed too close to the wall which does not allow sufficient airflow across the coils of the condensers, so as to allow for effective heat transfer. There is no consistency of brand for the split systems. We registered at least ten different brands throughout the block. Air-conditioning units were simply added over time as spaces within the hospital required cooling. The number and various types of AC units and vendors leads to high operation and maintenance costs for the hospital. Figure 3. Leaking external duct Figure 4. Uninsulated external ductwork Page | 11 Ventilation The original building was built before mechanical systems became commonplace, and therefore made use of natural ventilation. For the now conditioned spaces, the natural vents were closed up to accommodate air conditioning. Some spaces, like the Physiotherapy Department are recycling air without mixing in fresh air. The Radiology Department, which is mostly served by split units, is mixing fresh unconditioned outdoor air with a blower fan. This is due to the fact that the original compressor is broken and needs to be replaced. We took CO2 readings for several rooms and found that occupied rooms, such as the Eye Clinic, were above the upper limit for indoor CO2 levels according to OSHA and ASHRAE standards (https://www.osha.gov/dts/osta/otm/otm_iii/otm_iii_2.html), which recommend that CO2 levels remain below 1,000 ppm for properly ventilated spaces. There is no provision for adequate air changes in many areas resulting in high carbon dioxide levels. Some rooms measured as high as 1,370 PPM of CO2. Figure 5. Blower serving Radiology Department Figure 6. Ductwork leading from blower to Radiology Building Controls There is no centralized control system for this building, such as an Energy Management System. The central AC units are typically controlled by programmable thermostats (which were not programmed) while each split unit has its own remote control. Lighting is controlled by manual switches. Lighting There are T12 and T8 lighting fixtures mixed throughout the entire building. Whenever a T12 fixture burns out, the maintenance staff replaces it with a T8 fixture. Several burned out and broken fixtures were observed however. For exterior lighting, metal halides and halogens were used. Exterior and corridor lighting operate during the day as well resulting in wasted energy. Ample opportunity was observed in several rooms for natural daylighting. Page | 12 Figure 7. Lights on during the day Figure 8. Burned out lighting fixture Electrical Metering The entire hospital campus is served by one electrical meter. Prior to the visit, we were told that the NB had its own meter. After discussions with the electrician asking him to show us the main supply line, he showed us the two transformer kiosks serving the NB. After reviewing the equipment we found onsite, the area of the NB, and our spot measurements, we believe that the hospital bills we received cover the entire campus. Below are some measurements that were taken during standard operating hours. The measurements were taken at 10:00 am, a few hours after the NB opened and tells us the AC units are consuming the most electricity as we expected. The electrician said they had a 3-phase Delta system. Location Served Equipment Served Physiology (New Const); Eye Clinic X-Ray Department & Eye Theater X-Ray Department Central AC Split AC, Lighting, Plug loads X-Ray Equipment Line Ph 1 Voltage V 225 NM Ph 2 V NM Ph 3 V NM Ph 1 A 130 Ph 2 A 99 Ph 3 A 123 225 110 110 197 174 276 101 440 NM NM NM 4.40 5.00 4.90 Building Envelope The orientation and design of the building facilitates the use of passive energy such as natural ventilations and day lighting. The external corridors overhangs provide shade to the internal spaces along the South façade. The roof overhang also provides shade to the internal spaces along the east and west facades. A new roof was installed with mineral wool insulation and heat insulation foil and the Page | 13 external corridors also have heat insulation foil with PVC soffits. All air-conditioned spaces have ½” mineral fiber acoustic ceiling tiles and internal ceilings are white which provides good light reflectance. It was observed that surfaces in the NB are predominantly durable and require minimal maintenance. Although, these existing finishes have low thermal insulation properties, the heat gains are dissipated quickly because the spaces are naturally ventilated. Some issues encountered were that new external doors do not have floor thresholds and as a result have substantial gaps between the door and the floor which cause heat gain into the air-conditioned spaces. In addition, the external doors of air-conditioned rooms are aluminum hollow core. The colonial style windows which are double casement windows with fixed louvers (jalousies) surrounding were originally designed to facilitate natural ventilation. When it is sunny, the casement windows can be opened to allow maximum wind flow through the opening and closed during rain fall. The jalousies allow wind to penetrate into the building. A majority of the original wooden jalousies have been removed, due to physical deterioration, and replaced with triple casement steel framed windows. This change in the window layout, though not applied universally in the whole building, was observed in rooms with and without air conditioning. This substitution has had two main effects; one effect is the increase in control of air flow in spaces that are not air conditioned. However, during periods of heavy rainfall these windows must be closed which completely restricts natural ventilation but allows more natural daylighting into the rooms than the jalousies. It can be therefore assessed that despite the advantage of increased airflow to these non-air conditioned rooms during dry periods and increase daylighting in rainy periods, one weakness is the loss of ventilation during rainy periods. Conversely, however, the steel casement windows prevent the loss of cooled air from the air conditioned rooms, a function that would not have been possible with the original wooden jalousies. This change increases the potential for ventilation when the windows are open, but restricts air flow through the building when they are closed which has inhibited the natural ventilation. Incidentally, this condition is desirable for spaces which are air-conditioned, such as the offices or technical rooms, as the steel windows prevent the loss of cooled air to the outside, while providing the occupant with the ability to get fresh air when the AC unit is not functioning. In some cases, there are incidents where air-conditioned spaces have colonial style windows on its exterior walls and Plexiglas has been used to cover the gaps in the jalousie with the intention of sealing the openings; however, air leakage is still prevalent, because the installation is not fixed properly. Nonetheless, this is a very good solution for keeping the architectural aesthetic while renovating or upgrade the facility. There are also instances where the window glass panels have been painted on the interior side of offices and technical rooms. The intended purpose of this alteration may have been to block the natural light coming into the space or create privacy in that specific room. Page | 14 Figure 9. Roof insulation Figure 10. Jalousie window with AC unit Domestic Hot Water Two 40-gallon electric hot water tanks serving restrooms provide the only hot water for the NB. Previously, black plastic water tanks outside were used, but these have been disconnected. 3.3 Renewable Energy Assessment The NB has little opportunity for renewable energy measures that have short payback as the building only uses two 40-gallon electric hot water tank systems for the bathrooms and one electric heater for the showerhead due to the fact that hot water was mainly used in other buildings and not nearly as much in the North Block, leading to a long payback period. In the past, the POSGH NB had a central boiler room for distributing hot water, but over time as the system went into disrepair, it was replaced with independent decentralized electric water heaters. Most of these hot water systems are located in other buildings of the hospital. Grid-connected photovoltaics is not yet an economic option, as the payback period is approximately 24 years without any feed-in tariff and there are no clear guidelines with time estimates for the process of connecting to the grid in Trinidad and Tobago. Some areas with outdoor pathways require additional lighting, but are located far from the electricity supply; however, full solar street lights would have high upfront cost. Solar powered LED bollard lighting would be a more cost-effective option at US$ 1,250 per unit including installation. Figure 11. Solar powered LED lighting Page | 15 3.4 Energy Conservation Opportunities The following energy conservation measures were identified for POSGH NB. No incentives were found for energy efficiency upgrades. ECM-1 Replace all T12 fixtures with new T8 fixtures Required Annual Energy Annual Cost Investment Savings Savings (US$) (kWh) (US$) 22,710 148,298 6,484 Available Incentives (US$) NA Payback with Incentives (Years) 3.5 Payback with no Incentives (Years) 3.5 Existing Condition: Inefficient Lighting The old T12 lighting fixtures on the NB appear to be at the end of their lives. The lighting fixtures are also in bad condition, with many broken fixtures, several burnouts, and the fixtures are old and dirty, therefore not achieving optimal lighting distribution. The 4-foot lamps were typically 40W, while the 8foot lamps were 75W. Equivalent 4-foot T8 lamps would be 32W and 8-foot T8 lamps would be 59W. There were also different colored lamps in some areas. Recommendation: Replace the old lighting fixtures with entirely new lighting fixtures, preferably with fixtures that have reflectors. The addition of a reflector will allow the client to improve lighting distribution in their spaces, while reducing the number of required lamps in half. In this case, an electronic ballast with a high ballast factor would need to be installed. Electronic ballasts come in low medium, and high ballast factors. A ballast with a high ballast factor consumes more energy while providing greater light output. The advantage in terms of efficiency is that you are able to use a reflector instead of additional lamps, thereby saving energy, In addition, 800 series high performance lamps should be used in interior spaces, where lighting color quality is important and 4,100k (natural white) is the typical color used in commercial applications. 800 series lamps provide for better quality light which is important in hospitals. 700 series T8 lamps provide lower quality light. For the 2-foot wall mounted fixtures, a lamp and ballast retrofit using standard equipment would suffice. Implementation: The estimate includes the cost of replacing (321) 4-foot T12 lighting fixtures at a cost of US$60 each and retrofitting 111 2-foot fixtures at US$30-$35 each, including material and labor. ECM-2 Delamp 4-lamp T8 fixtures and install (2) T8 lamps with high ballast factor and reflectors Required Annual Energy Annual Cost Available Payback with Payback with Investment Savings Savings Incentives Incentives no Incentives (US$) (kWh) (US$) (US$) (Years) (Years) 1,645 10,818 474 NA 3.5 3.5 Existing Condition: Inefficient Lighting Page | 16 Recommendation: 4-lamp T8 fixtures are inefficient lighting fixtures. The typical retrofit is a 2-lamp T8 fixture with an electronic T8 ballast that has a high ballast factor, high performance lamps, and a reflector. Since the T8 fixtures are relatively new, only a retrofit would need to be completed in this case. An electronic T8 ballast with a high ballast factor puts out more light and is more efficient when used with a reflector than the current configuration. Implementation: Estimated costs include a 2-lamp ballast with high ballast factor, 2 high performance T8 lamps, a reflector kit, and labor. We counted (47) fixtures that could be replaced at US$35 each. ECM-3 Replace outdoor lighting fixtures with a 70W photocell controlled LED wall packs Required Annual Energy Annual Cost Available Payback with Investment Savings Savings Incentives Incentives (US$) (kWh) (US$) (US$) (Years) 2,800 16,031 690 NA 4.1 Payback with no Incentives (Years) 4.1 Existing Condition: Inefficient Lighting Recommendation: There is a combination of metal halide and halogen fixtures being used for outdoor lighting. The halogen fixtures consumed 500 W each, while the metal halides appeared to be 175 W, but we were not able to confirm the wattage. Some fixtures were on during the day and it is believed the others were burned out due to the condition of the fixtures. Some fixtures were damaged as well. A photocell will ensure that the fixtures are only operating at night or when daylight falls below recommended levels. Implementation: The estimated cost of a 70 W LED fixture with installation included is US$400 and a one-for-one replacement is recommended with a total of 7 fixtures. ECM-4 Replace incandescent lamps with compact fluorescent lamps Required Annual Energy Annual Cost Available Investment Savings Savings Incentives (US$) (kWh) (US$) (US$) $32 2,593 88 NA Payback with Incentives (Years) 0.4 Payback with no Incentives (Years) 0.4 Existing Condition: Inefficient Lighting 60 W incandescent lamps were found in the Physiotherapy Room which was just remodeled and the lights were on. We were told that they would be replacing these with CFLs. Recommendation: We recommend 23 W CFL bulbs versus the standard 13 W CFL replacement for the 60 W incandescent bulbs, since these rooms appeared to be under lit. Implementation: Estimated cost of (1) 23W CFL is US$4. Page | 17 ECM-5 Install timers in high traffic areas and external corridors Required Annual Energy Annual Cost Available Investment Savings Savings Incentives (US$) (kWh) (US$) (US$) $2,200 109,727 3,539 NA Payback with Incentives (Years) 0.6 Payback with no Incentives (Years) 0.6 Existing Condition: Lights are left on in unoccupied spaces Lights were left on in some spaces after closing and were on along external corridors during daylight hours. This results in a great deal of energy being wasted. Recommendation: Install astronomical time clocks on lighting circuits in areas with high traffic and fixed schedules as well as external corridors. For external corridors, time clocks should be set to turn lights on at night only. For interior high traffic areas, maintenance should have discussion with staff to determine hours that lighting needs to be run for weekdays and weekends. Implementation: Estimated cost per astronomical time clock installation with programming is $220 USD. ECM-6 Install occupancy sensors in low traffic areas with little natural lighting Required Annual Energy Annual Cost Available Payback with Investment Savings Savings Incentives Incentives (US$) (kWh) (US$) (US$) (Years) $500 6,588 $223 NA 2.2 Payback with no Incentives (Years) 2.2 Existing Condition: Lights left on in low traffic unoccupied spaces Recommendation: Install occupancy in areas with low traffic such as storage spaces or rooms that are seldom occupied. Implementation: Estimated cost per occupancy sensor installation is $100 USD. ECM-7 Install indoor photo sensors in areas with sufficient daylight Required Annual Energy Annual Cost Available Investment Savings Savings Incentives (US$) (kWh) (US$) (US$) $1,500 25,093 $849 NA Payback with Incentives (Years) 1.8 Payback with no Incentives (Years) 1.8 Existing Condition: Lights are left on in spaces with sufficient daylight The lighting was operating in areas that appeared to receive sufficient day lighting such as the Eye Clinic and the X-Ray Lobby (north). Page | 18 Recommendation: Install an indoor photo sensor that will turn off lights when natural lighting is sufficient to illuminate the room. For some areas, new wiring may be needed if perimeter lighting is on the same circuit as interior lighting. Implementation: Estimated material and labor cost of each photo sensor installation is US$150. If an area does need new wiring, the costs will depend on the number of fixtures that must be rewired. An electrical contractor should be consulted to get an accurate estimate. ECM-8 Program programmable thermostats for packaged AC units for nighttime and weekend setback Required Annual Energy Annual Cost Available Payback with Payback with Investment Savings Savings Incentives Incentives no Incentives (US$) (kWh) (US$) (US$) (Years) (Years) $0 5,000 $170 NA NA NA Existing Condition: Unprogrammed thermostats The programmable thermostats were found not to be programmed for nightly and weekend setback. One example was the Physiotherapy Room that was unoccupied, but had air conditioning running 24/7 with a set point temperature of 21ºC. The measured room temperature for Physiotherapy was 24ºC with 62% humidity while unoccupied, due to envelope issues and possible issues with the ductwork. Recommendation: The set point temperature should be increased while the room remains unoccupied due to construction. For occupied rooms, the thermostats should be programmed for night time and weekend setback. Humidity levels should be measured to ensure that indoor relative humidity remains below 60% at 24ºC dry bulb to prevent any mold growth. Due to the humid climate and condition of the building envelope, it is not recommended that air conditioning units are completely turned off for any extended period of time. Implementation: Work may be completed by onsite staff familiar with digital controls. ECM-9 Increase setpoint temperatures on split and packaged AC Units Required Annual Energy Annual Cost Available Investment Savings Savings Incentives (US$) (kWh) (US$) (US$) $0 5,000 $170 NA Payback with Incentives (Years) NA Payback with no Incentives (Years) NA Existing Condition: Temperatures set too low We found the set point temperature to be too low in most rooms. Recommendation: Temperatures should be set between 24 and 26 degrees Celsius for Recovery and Patient rooms and between 17 and 27 ºC for Operation Theatres. Humidity levels should be monitored to ensure that indoor relative humidity remains below 60% at 24ºC dry bulb to prevent any mold growth. Ideal relative humidity levels for hospitals is 45% - 55%. Due to the humid climate and Page | 19 condition of the building envelope, it is not recommended that air conditioning units are completely turned off for any extended period of time. Implementation: Work may be completed by onsite staff familiar with digital controls. ECM-10 Install door thresholds for all external doors of air conditioned rooms. Required Annual Energy Annual Cost Available Payback with Investment Savings Savings Incentives Incentives (US$) (kWh) (US$) (US$) (Years) $1,000 20,000 $680 NA 1.5 Payback with no Incentives (Years) 1.5 Existing Condition: Inefficient doors New external doors do not have floor thresholds and as a result have substantial gaps between it and the floor which cause heat gain into the air conditioned spaces. Recommendation: Door thresholds should be installed for all external doors of air conditioned rooms. Implementation: Estimated cost per door threshold is $20. Maintenance staff would install thresholds. ECM-11 Replace hollow core doors with solid core doors for all external doors of air conditioned rooms. Required Annual Energy Annual Cost Available Payback with Payback with Investment Savings Savings Incentives Incentives no Incentives (US$) (kWh) (US$) (US$) (Years) (Years) $3,000 20,000 $680 NA 4.4 4.4 Existing Condition: Inefficient doors External doors of air conditioned rooms are aluminum hollow core Recommendation: Solid core doors generally have higher insulation capacity and should be used for external doors to air conditioned rooms. Implementation: Estimated cost per solid core door is $200. Maintenance staff would install doors. ECM-12 Readjust sensor for sliding door over X-Ray reception Required Annual Energy Annual Cost Available Investment Savings Savings Incentives (US$) (kWh) (US$) (US$) $0 1,500 $51 NA Payback with Incentives (Years) NA Payback with no Incentives (Years) NA Existing Condition: Inefficient doors Page | 20 The external sliding doors for the main X-Ray reception which is air-conditioned are ineffective for reducing loss of cooling to the space for the following reasons. Door opens and close for approximately 15s Door sensor opens the doors when people pass by along the external corridor. Recommendation: External sliding door sensor should be adjusted to open doors only for people standing directly in front of it. Implementation: This can be performed by hospital maintenance staff. ECM-13 Air sealing of building envelope where leaks are present in windows, doors, and walls Required Annual Energy Annual Cost Available Payback with Payback with Investment Savings Savings Incentives Incentives no Incentives (US$) (kWh) (US$) (US$) (Years) (Years) $3,080 120,000 $4,080 NA 0.75 0.75 Existing Condition: Poor envelope condition There are a number of damaged windows and doors with gaps or holes resulting in great air loss and increased energy consumption for air conditioning units. In turn, this leads to greater temperatures and higher humidity indoors, which can in turn, lead to mold issues. Recommendation: Broken windows should be repaired and holes in envelope or doors for air conditioned spaces should be sealed in order to tighten the building envelope and prevent infiltration of hot and humid outdoor air. Implementation: Cost of air sealing is estimated at US$0.14 per square foot of conditioned space. An insulation professional should be hired to perform air sealing work. ECM-14 Central duct HVAC system with humidity control to replace all split units Required Available Payback with Annual Energy Annual Cost Investment Incentives Incentives Savings (kWh) Savings (USD) (USD) (USD) (USD) $700K – 900K Level 3 Req. Level 3 Req. Level 3 Req. Level 3 Req. Payback with no Incentives (USD) Level 3 Req. Existing Condition: Inefficient HVAC system The current HVAC configuration is inefficient. There are several different types of split systems serving different areas leading to higher operating and maintenance costs due to the decentralized systems and number of units operating. In addition, the use of these systems is insufficient to address indoor air quality concerns due to lack of ventilation and they are not able to properly control humidity, leading to dehumidifiers being used in some rooms and other rooms experiencing high humidity for hospital rooms. Page | 21 Recommendation: Plan a phased conversion to a centralized system for the entire block. Removal of split AC units and installation of centralized ducted AC system with humidity control such as desiccant wheels or electric reheat. Return air ducts also necessary to mix conditioned air with fresh air in order to conserve energy. Consider a centralized chilled water system for the whole block which in the long term would yield greater energy as well as cost savings but will have a greater first cost and more down time to the hospital to accommodate installation. Due to the time it takes to install a new chiller plant versus replacing split units one by one, rooms would have to be closed to accommodate the new duct system. Building envelope improvements must first be realized before undertaking this measure. Figure 12. Schematic of desiccant wheel courtesy of everything-ice.com Implementation: An ASHRAE Level 3 Energy Audit is necessary before undertaking this measure. If the decision is to maintain single split systems where they are currently used, there should be an aim to standardize the brand. 4.0 Operational and Behavioral Guidelines HVAC Operation and Maintenance A great deal of energy is wasted from having the packaged AC units run 24/7 at full capacity while rooms like Physiotherapy are unoccupied. In addition, all the holes and leaks in the envelope require all AC systems to run constantly. Training maintenance staff to locate and close leaks that appear over time is vital to keep infiltration to a minimum thereby reducing the required cooling load. Great care should be taken though to ensure good IAQ . Any damage or leaks to HVAC ducts should be immediately repaired. Outdoor ducts should be insulated and weatherproofed to prevent damage caused by the elements. Damaged condensing coils should be replaced or repaired. Condensing units should be positioned further from the wall to allow for sufficient Page | 22 air flow across the coils. Damaged insulation on refrigerant should be repaired as soon as it is discovered. Air filters should be checked on schedule and replaced when necessary. The issues listed above are maintenance and repair issues. While they may save energy, they are more important in the sense that if they are not addressed, the system will not function properly. Lighting Operation and Maintenance A great deal of energy is wasted by leaving interior lights on when rooms are unoccupied and leaving exterior lights on during daylight hours. The installation of automated lighting controls as detailed in the energy conservation section would do a great deal to address this issue by removing the human element. Maintenance staff should be trained to ensure all lighting controls, including existing time clocks are operating as they should and according to schedule. Awareness Campaign In order for POSGH to wage a successful energy awareness campaign, the awareness of hospital staff and students must be elevated. POSGH should follow the steps outlined below to successfully reduce energy consumption through awareness. Step 1: Planning Phase 1. Commitment should be obtained from POSGH senior management in supporting the awareness campaign 2. An “Energy Efficiency Champion” should serve as the spokesman for the energy efficiency program to promote the program and endorse the program’s messages 3. A team should be assembled to oversee the energy efficiency initiatives and a person from that team should be assigned as the program leader 4. Baseline energy consumption for the entire hospital campus should be established for different end-uses to determine where the most energy is being used and can be saved. 5. Determine the energy awareness of staff through surveys and questionnaires 6. Establish POSGH’s mission and goals for the awareness campaign 7. Develop an annual budget for the program based on POSGH’s financial resources and expected energy and cost savings Step 2: Design and Implementation Phase 1. Work with employees to determine where operational improvements can be made to reduce energy consumption while maintaining existing comfort levels 2. Identify communication tools that will be used to promote awareness in the hospital including newsletters, pamphlets, posters, press releases, and more 3. Develop messages/slogans that promote energy conservation in the hospital as well as material that may be distributed such as stickers placed over switches to remind occupants to turn off the lights before leaving a room unoccupied 4. Develop and determine which activities will be carried out to conserve energy and plan a budget for those activities, goals, and anticipated results 5. Create a time frame for carrying out activities and reporting results Page | 23 Step 3: Measure, Evaluate, and Report Results 1. Determine effectiveness of overall program activities through analyzing POSGH’s energy bills versus past energy bills 2. Determine effectiveness of individual program activities by obtaining employee feedback and surveying hospital employees 3. Aggregate and compile estimated energy savings due to program activities and create promotional material documenting POSGH’s activities and resulting energy and cost savings 4. Conduct quarterly or bi-annual evaluation of activities to monitor activities and make adjustments where needed Step 4: Follow Through 1. Coordinate regular meetings with senior management to show results and effectiveness of approaches and plan for the following year. 2. Get feedback from involved parties to determine strengths and weaknesses of various approaches to determine best practices and develop new approaches for the following year 3. Publically recognize and award employees that make the greatest contributions to conserving energy Page | 24 Appendix A – Site Plan Page | 25 Appendix B – Floor Plans Ground Floor First Floor Page | 26 Appendix C – Lighting Survey Fixture Type 1L 2F T12 (20W) 2L 2F T12 (20W) 2L 4F T12 (40W) 2L 8F T12 (75W) 4L 4F T12 (40W) 2L 4F T8 (32W) 2L 8F T8 (59W) 4L 4F T8 (32W) Incandescent (60W) 175W MH 500W Halogen Total kW Demand Base Total Fixture W Total kW Controls 87 26 2.262 Manual 24 51 1.224 Manual 142 86 12.212 Manual 10 158 1.58 Manual 169 172 29.068 Manual kWh Base Annual Hours 3120 3120 8760 4380 2600/8760 Total kWh 7,057 3,819 106,977 6,920 191,064 68 1 35 56 109 112 3.808 Manual 0.109 Manual 3.92 Manual 8760 8760 8760 33,358 955 34,339 8 5 2 551 60 215 500 0.48 Manual 1.075 Manual 1 Manual 56.738 8760 8760 8760 4,205 9,417 8,760 406,872 Additional data concerning lighting equipment is available upon request. Page | 27 Appendix D – Air Conditioning Survey Room Area (sqf) Controls Physiotherapy Room 2637 Digital Thermostat Eye Clinic 3304 Digital Thermostat Ultra Sound 265 Thermostat SCREENING ROOM SKIN CLINIC 340 Thermostat Doctor's Examination Clinic 200 Radiographer's Staff room 280 Manual Remote Room 6 Main X-ray 223 Manual Remote Room 7 Main X-ray 255 Manual Remote Doctor's Office X-Ray Dept. 134 Manual Remote Head of Radiology 112 Thermostat CT Scan Processing Room Equip 444 Thermostat Ward 2 Office GRD FLR 115 Thermostat Ward 1 Nurse's Office 115 Thermostat Ward 1 2050 Thermostat ENT Theatre 1230 Thermostat Eye Theatre 1230 Thermostat Ward 1 Pantry 118 Thermostat Eye Clinic Dispensary 106 Thermostat Births and Deaths 2270 Thermostat X-Ray Review Room 95 Thermostat Head Nurse 54 Thermostat Nurse's Room 1st. Floor Skin Clinic 157 Thermostat Prep Room Skin Clinic 200 Thermostat Ward 15 125 Thermostat Ward 15 125 Thermostat Make Carrier Carrier NORDYNE NORDYNE PEAKE YORK CARRIER CONCORD COLD WAVE MILLER MILLER YORK Cold Wave PEAKE CARRIER CARRIER Cold Wave Toshiba Peake Craft Carrier Miller Carrier Cold Wave Cold Wave Model 50TC-D17A5A5A0A0A0 50TC-D24A5A5ADA0A0 P3RA-060K 91820A XL0108-R PCU-036M-216 B0C25R16A 38CKC03635(0)1 RC10A36A-1B SS2-24000 MDX5-012KCR1 MDX4-024KCK3 YJDA18FS-ADA No data found PCV-036B216-PC0 38AUZA 12A0A 5A0A0A0 38AUZA12 A0A5A0A0A0 MSE-12CRN1 CWC18NC Type Rooftop Packaged Unit Rooftop Packaged Unit Packaged Unit Split System Split System Split System Split System Split System Split System Split System Split System Split System Split System Split System Condenser Condenser Split System Split System Split System Window Unit Window Unit Window Unit Window Unit Split System Split System Tons 15.0 20.0 4.6 3.0 3.0 2.0 3.0 3.0 2.0 1.0 2.0 No data No data V A kW EER IPLV 230 64.7 17.5 11.0 12.0 230 83.6 24.2 10.0 11.0 230 38.6 8.9 10.0 NA 230 19.4 4.5 No data NA 230 17.0 3.9 No data NA 230 10.8 2.5 No data NA 230 17.4 4.0 10 SEER NA 230 17.1 3.9 10 SEER NA 230 11.3 2.4 No data NA 240 6.7 1.6 No data NA 240 11.8 2.8 No data NA No data No data No data No data No data No data No data No data No data No data 3.0 230 20.9 4.81 No data NA 10.0 230 33.1 10.4 11.2 NA 10.0 230 33.1 10.4 11.2 NA 230 NA 2.0 230 11.0 2.5 NA 1.5 230 11.2 2.6 No data NA 2.0 230 11.0 2.5 NA 2.0 230 11.0 2.5 NA 1.5 230 11.0 2.5 NA 2.0 230 11.0 2.5 NA 1.0 230 5.1 1.2 13 SEER NA 1.5 230 11.0 2.5 Additional data concerning air conditioning equipment is available upon request. Page | 28 Appendix E – Measurements and Envelope Room Setpoint Temp (Deg C) Measured Temp (Deg C) Relative Humidity (%) CO2 Readings (ppm) Height (ft) Construction Physiotherapy Room 21.0 23.0 62% 477 13 Average Eye Clinic 21.0 23.7 52% 1,245 13 Poor Ultra Sound No Data 22.0 59% 562 13 Average SCREENING ROOM SKIN CLINIC No Data No Data No Data No Data 13 Average Doctor's Examination Clinic No Data No Data No Data No Data 13 Average Radiographer's Staff room No Data 26.1 65% 507 13 Average Room 6 Main X-ray No Data 23.0 67% 559 13 Average Room 7 Main X-ray No Data 24.3 68% 624 13 Average Doctor's Office X-Ray Dept. No Data No Data No Data No Data 13 Average Head of Radiology No Data 23.1 74% 472 13 Poor CT Scan Processing Room Equip 18.0 21.9 68% 444 13 Average Ward 2 Office GRD FLR No data No data No data No data 13 Average Ward 1 Nurse's Office No data No data No data No data 13 Poor Ward 1 No data No data No data No data 13 Poor ENT Theatre No data 22.0 82% 381 13 Poor Eye Theatre No data 22.6 70% 543 13 Poor Ward 1 Pantry No Data No Data No Data No Data 13 Poor Eye Clinic Dispensary No Data No Data No Data No Data 13 Poor Births and Deaths No Data No Data No Data No Data 13 Poor X-Ray Review Room No Data No Data No Data No Data 13 Poor Head Nurse No Data No Data No Data No Data 13 Poor Nurse's Room 1st. Floor Skin Clinic No Data No Data No Data No Data 13 Poor Prep Room Skin Clinic No Data No Data No Data No Data 13 Poor Ward 15 No Data No Data No Data No Data 13 Poor Ward 15 No Data No Data No Data No Data 13 Poor Additional data concerning measurements and building envelope is available upon request. Page | 29 Appendix F – Equipment Survey Data concerning surveyed hospital equipment is available upon request. Page | 30 Appendix G – Spot Measurements Location Served Equipment Served Physiology (New Const); Eye Clinic X-Ray Department & Eye Theater X-Ray Department Central AC Split AC, Lighting, Plug loads X-Ray Equipment Line Ph 1 Voltage V 225 NM Ph 2 V NM Ph 3 V NM Ph 1 A 130 Ph 2 A 99 Ph 3 A 123 225 110 110 197 174 276 101 440 NM NM NM 4.40 5.00 4.90 Page | 31