GIT pain premeeting Qs

[
PBL PATIENT CASE 9
]
Abdominal Pain
Pre-Meeting Questions
1.
Describe the anatomy of the gastrointestinal tract, renal tract, abdominal aorta, pancreas and hepatobiliary tree.
2.
Where are pain receptors found in the GI tract? What kind of pain do patients describe and what is the physiological basis for this experience when they have problems of the respective organ?
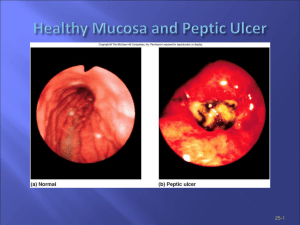
Stomach:
Located in left hypochondium and epigastric regions.
Cardia: surrounds cardial orifice.
Fundus: dilated superior part, reaches level of about 5ICS
Body: Fundus to antrum. Cheif(pepsinogen) and parietal (Hcl) cells.
Pyloric Part: wide antrum leading into narrow pyloric canal which thickens with circular muscle to form pyloric sphincter which is normally under tonic contractions but opens to allow chime into SI.
*Mucous cells in all regions of stomach
Arterial Supply: Coeliac trunk with R+L gastric arteries along lesser curvature. R+L gastroomental arteries along greater curvature.
Also tortuous splenic artery giving off short gastric arteries.
Nerves: parasymp from vagal trunks that enter through oesophageal hiatus.
*Pain receptors: visceral pain receptors on serosal surfaces and wall of mesentery, pain is poorly localised and response to chemical and mechanical stimuli, and is generally referred to midline.
Small Intestine:
Duodenum: has C-shaped course around head of pancreas at L2. Second part has bile and pancreatic ducts running into ampulla.
Jejunum and Ileum: Part of Midgut region therefore supplied by SMA which leaves Abdominal Aorta at level of L1 and supplies 15-
18 branches forming arterial arcades that give rise to vasa recta. Characteristics to distinguish each:
Jejunum: deeper red, wider, thick and heavy walls, high and long vasa recta and closely packed circular folds.
Colon:
Ileum: pink, narrower, thin walls, short vasa recta, Peyers patches and Merckels Diverticulum (rule of 2’s).
Ascending (attached to post ab wall) to right colic flexure (retroperitoneal) from ceacum. Transverse part is mobile. Splenic flexure is junction of mid and hidgut so colon distal to this point is supllied by IMA. Descending (attached to post ab wall) colon runs into sigmoid which joins rectum at S3. Distinguishing features:
Teniae coli: 3 thickened muscle layers that make up longitudinal layer.
Haustra: sacculations of colon between teniae (outpouchings of wall)
Omental appendices (epiploica): small fatty projections off the omentum.
Pain: Bowel obstruction causes colicky pain that can occur anywhere in the abdomen. Colon obstruction tends to cause less frequent colicky pain that small intestine (ie. every 15min instead of every 2-3 min). Vomiting, constipation and abdominal distension also associated.
Abdominal Aorta:
Passes through aortic hiatus (T12) to level of L4 (iliac crests) where it divides into R+L and continues as common iliacs and median sacral branch
Coeliac trunk at upper border of pancreas: left gastric, splenic and common hepatic.
[
PBL PATIENT CASE 9
]
Abdominal Pain
SMA from 2 nd part duodenum. Passes behind neck of pancreas but over 3 rd part duodenum and supplies duodenum distal to ampulla. Gives off brances to ileum and jejunum and middle and right colic brances to proximal colon .
IMA from splenic flexure at L3. Runs obliquely to peliv brim and crosses bifurication of common iliac arteries. Terminates as superior rectal artery after giving off sigmoid and left colic arteries.
Renal Tract:
Kidneys: lie retroperitoneally on post ab wall at level approx T11/12 with right lower due to liver. Renal hilum at L1 has VAT ant to post.
Ureters: muscular ducts 25-30cm long have retroperitonel course from kidney to bladder in front of lumbar spinous processes. Crosses psoas major and bifurication of common iliac artery. # points narrowest calibre: pelviutereric junction, crossing pelvic brim and passing through bladder wall.
Pain: pain of kidney refers to back. Ureters goes to lumbar or hypogastric or genital region depending on level of injury. Renal calculus causes colicky pain as ureters consistently contract to try push stone out, with radiation towards the groin.
Pancreas:
Functions as exocrine (acinar cells of alveoli secrete pancreatic juice) and endocrine (glucagon and insulin from islet cells). Lies retroperitoneal at level LI, post to stomach, duodenum on R and spleen on L.
15 cm long.
Divided into head, uncinated process (curved bit), neck, body and tail which is close to hilum of spleen. Head is near ampulla (tumor of pancreas can block bile duct as well as pancreatic duct). Also accessory duct (may be absent) which opens directly into duodenum (not associated with bile duct).
Arterial suplly from splenic artery and gastroduodenal artery.
Acute pancreatitis may occur is pancreatic duct is blocked – build up of pancreatic enzymes causes pancreas to start digesting itself.
Pain: intrinsic pain refers to epigastric region, while inflammation can hit other structures and refer to posterior abdominal wall and
BACK. Pain may be partially relieved by sitting up and leaning forward. Vomiting common.
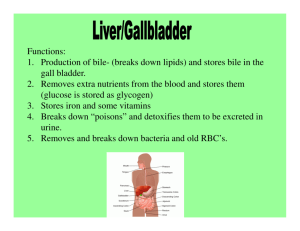
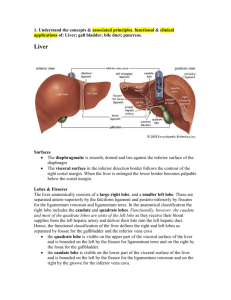
Hepato-biliary tree:
Gall bladder releases stored bile when fat reaches duodenum (CCK stimulates). In liver hepatocytes secrete bile into canaliculi which drain into interlobular bile ducts> R+L hepatic ducts> common hepatic duct> joined by cystic duct from gall bladder to form bile duct> joined by pancreatic duct to form ampulla of Vater which empties into 2 nd part duodenum. Gall bladder has Hartmann
Pouch at junction of cystic duct where gall stones commonly collect. Gall stones: Fat, Forty, Female, Fair, Fertile with distal part of ampulla narrowest point of duct system.
Pain: rarely colicky despite being called colic. Often severe constant pain in epigastria that can last for hours if cystic duct obstruction. Cholecystitis causes pain to shift to RUQ and may become more severe.
Pain Key Points:
Paired: nerves from same side so pain referred to that side. Kidneys and ureters.
Unpaired: bilateral nerve supply so refer to midline even if not midline. Stomach, pancreas, liver etc.
Midline: Formed by union of two halves so two nerve supplies.
Abdominal referred pain: Foregut > T8, Midgut > T10, Hindgut > T12
Back pain can be from abdominal viscera: pancreas, duodenum, aorta and parietal peritoneum pathology can all present with back pain with possible dorsal rami involvement.