medsurg reviewii
advertisement

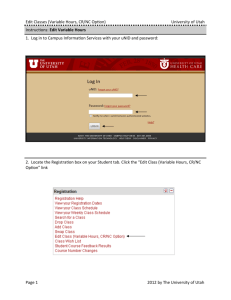
What are somethings to consider during preoperative preparation? Assessment Preadmission testing Preoperative teaching Informed Consent Patient preparation Emergency Surgery Edit 2 A patient that has been admitted into your unit has a scheduled surgery for the following day. The patients states he is allergic to latex. What, as the caregiver, must you do next? Inform the Physician and the surgical unit to prepare for preventative actions. Edit 3 Prior to surgery what should the TPCN assess for regarding history? General health & Physical status Allergies Current Meds Nutrition Understanding of scheduled procedure Psychosocial/spiritual needs Educational Needs Edit 4 If a patient drinks a six pack of beer a day are they an alcoholic? Yes, poss risk for Delirium Trimmers if restricted from continuous us for surgical procedures. Edit 5 Why does obesity affect clients in surgery? Adipose tissue does not heal as well or fast Edit 6 Why is it important to assessment the patient for ETOH and Tobacco use? Liver problems doesn't cause coagulation, malnutrition, or metabolism. (Delays wound Healing) Edit 7 Chemo therapy aids and/or leukemia is important to know about a patient prior to surgery because this indicates what? Immunocompetence Edit 8 What are preadmission testing performed based on? Patient History Procedure General Health Status Medication Use Edit 9 Patients H/H are indicated to be low. Patients O2 level is still low after putting them on 4 liters of oxygen. Why? With Decreased Heme comes decreased O2 Edit 10 Why is it good to assess the thyroid level of a patient? Hormone that Regulates Metabolism Edit 11 TCDB stands for what and should be done when and in what increments? Turn, Cough, Deep Breath should be done after surgery once every hour? Edit 12 What is the deveice that assists in the expansion of the alveoli and diffuses the anesthesia outside of the body and decreases the chances of pneumonia? Incentive Spirometer (IS) Edit 13 What are some actions taken postoperatively to decrease secondary problems? TCDB/IS Early Mobilization Pain Management Edit 14 THis is the patients voluntary agreement to participate in a particular cure or treetment. It must be provided in words that are understood by the patient by the surgeon. Informed Consent Edit 15 What is required on a written consent? Name and details of procedure Name of Patient, Surgeon, and Anesthesiologist Time and Date of signature Will/Will not receive blood Risks and Hazards Name and Qualifications of the surgeon performing this procedure. Edit 16 Patient is admitted into the unit and is informed they will need to have surgery to remove their gallbladder. The patient is 17 years old and you are in need to get a consent signed. Who do you get to sign? You would get the parents/guardian. (Confused, sedated, mentally incompetent, and minors can not sign.) Edit 17 Your patient is to be preped for surgery. You notice the site of surgery, on the chest, has hair. Why would you not shave? Because it is evidence based practice that shaving prior to surgery increases risk for infection. Instead, clip with scissors. Edit 18 Your patient is admitted on your unit to have surgery that same day. Your patient is 69 year old female with a perm, make up, manicure with nails, dentures and jewelry. What do you do to prepare them for surgery. Ask the patient to allow you to place valuables with security, Remove atleast (if not all) one fake nail for O2 monitoring, wash face free of make-up to reduce risks for complications of the eyes, remove dentures and last but not least use the rest room before departure. Edit 19 These are three stages of Anesthesia. Conduction Maintainance Emergence Edit 20 This is used on minor short term surgical procedures. Topical Anesthesia Edit 21 Versed, valium is given while patient retains respiratory function while awake during these procedures. Conscious Sedation Edit 22 Surgery begins with administration until patient is taken to PACU. Intraoperative Care Edit 23 Perioperative Nurse can be an LVN. T/F False: can only be RN and up. Edit 24 What is the average stay in PACU? 2hours with an assessment every 10-15 min. Edit 25 This is the score used for assessing the 5 areas of activity, respiration, consciousness, and O2 sat for patients safety prior to returning to unit. Must be scored between 8-10. Alderete Score PARS (Postanesthesia Recovery Score) Edit 26 EBL means? and what's important about this? Estimated Blood Loss. Possible need for blood transfusion. Edit 27 What is linked to increased risk for surgical site infection? Hypothermia Edit 28 What is the purpose for the surgical site drains? To prevent from blood coagulation to increase chances of infection and dehesence. Edit 29 Jackson Prat JP Drain Edit 30 Serous Fluid is.... Cell Break down. Clear Fluid Edit 31 Where do the most of the nerves reside? On the surface of skin. Edit 32 What are some common nursing diagnoses for postoperative care? Acute Pain Decrease Cardiac Output: AEB Incr HR & Decr BP Impaired Skin Integrity: AEB surgical incision Risk For (many) Anxiety Knowledge Deficit Edit 33 Post-operatively, what is the limit for patient who is due to void? 8HRs post-op Edit 34 Atelectasis is caused by what post operatively? Not performing some essentials such as TCDB & IS. Edit 35 When should a patient be able to eat or drink? When the Gag Reflex occurs Edit 36 The occurrence of a broken clot that is moving, ex DTV is called ___. Thombosis Phlebitis Edit 37 When is staph seen in a surgery incision? 45 day after surgery Edit 38 What medications go with a PCA pump? Morphine, Demerol, Phentonyl, Diluadid Edit 39 Along with PCA what alternatives are give to relieve pain? Muscle Relaxant and PO meds Edit 40 How long do PCA's usually stay with a patient after surgery? 24 hrs, after that PO meds are administered. Edit 41 What are some nursing interventions for Pain relieve for postoperative care? Encourage early mobilization Pomote cardiac output, wound healing, bowel/bladder function Provide emotional support Education Edit 42 What is the lowest the diastolic pressure needs to be to insure proper blood flow to the brain? Diastolic pressure needs to be atleast 50and above Edit 43 How does a patient adapt to an illness or loss? Denial or disbelief; Anger; Bargaining; Resolution; Acceptance. Edit 44 What is the difference between active and passive participation? Active is reading the material given to them for the better of their health. Passive is disposing of all info given to them and not participating. Edit 45 What are the different types of Sutures? A) Individual/Interrupted B) Continuous Sutures C) Blanket Sutures D) Retention Sutures Edit 46 This is the act of a wound that opens along the joined edges. Dehiscence Edit 47 This is the removal of internal organs from an opened wound. Evisceration Edit 48 These sutures are used in surgical incision that prevent dehiscence and ultimately prevent evisceration. Retention Sutures Edit 49 What is the largest organ in the body? skin Edit 50 What is a break in the skin with disruption of the normal continuit of structures from a physical means? Wound Edit 51 This type of cleanliness consists of GI, uninfected operative outside of resp, genital, and urinary tract. Clean-Closed Edit 52 This type of cleanliness consists of operation wounds in respiartion, GI, genital or uninfective urinary tract. Clean-Contaminated Edit 53 This type of cleanliness is an Open, fresh, accidental, oper. c brk in sterile technique or GI spillage, nonpurulent inflammation. Contaminated Edit 54 This type of Cleanliness is in old wounds with dead tissue, infection, or perforated viscera. Dirty/Infected Edit 55 This is the tearing of tissue. Laceration Edit 56 This is the scraping of skin off surface. Abrasion Edit 57 This is a closed wound: bruise. Contusion Edit 58 This is a small, deep wound. Puncture Edit 59 This is an intentional cut into tissue. Incision Edit 60 This is a clean surgical incision with well defined edges and has minimal tissue loss during healing process (occuring by epithelialization) Primarily Healing Process Edit 61 This healing process a wound without proximate edges such as a pressure ulcer. (Great tissue loss, open wound) Secondary Healing Process Edit 62 This type of wound is the result of debridement of a large necrotic wound. Requires management of infection. Delayed suturing and grafts. Tertiary Healing process Edit 63 The bodies reaction towards wounds and begins within minutes of the injury and can last up to three days. Inflammatory Phase Edit 64 Injury occurs---3min-->swelling, redness, heat & Pain---> Bleeding controlled by hemostasis---> WBC's ingest bacteria & prepare for tissue repair Inflammatory Phase Edit 65 Damaged tissues & Mast cells creates histamine resulting in _____. Basal dilation Edit 66 New granulation tissue is generated producing a red, beefy, shiny tissue with a granular appearance is known as what phase of healing? Proliferative Phase Edit 67 What stimulates production of collagen; epithelialization with scar formation? Fibroblasts Edit 68 Collagen fibers reorganize, mature and gain tensile strength of a healing wound. This phase is known as? Maturation Phase Edit 69 Scar tissue is regains the skin's original strength and more. T/F False: Scar tissue regains 70-80% of skins original strength. Edit 70 This is new, healing tissue, very fragile at first and is red. What is this wound classified as? Granulation Edit 71 "Moist scab" necrotic tissue with yellow color. This wound is classified as? Slough Edit 72 "Dry Scab" Necrotic tissue known as what wound classification? Eschar Edit 73 You examine a patients wound. You notice the wound appears smooth, velvety texture with a dark red color with bumpy texture. What type of wound tissue is this? Granulation Tissue Edit 74 Angiogensis & collagen deposition is found in ____ Granulation tissue Edit 75 You find a patients wound appear creamy white, stringy, loosely adhering to wound. What type of wound is this? Slough Tissue Edit 76 Black fibrinous network of platelets, cells (scab), which becomes food for bacteria, delaying the healing process. Needs to be removed. Dead Tissue/Eschar Edit 77 (Internal) decreased Blood Pressure, increased pulse, increased respirations, diaphoresis and restlessness. These are complications of what type of wound? Hemorrhage Edit 78 Purulent Drainage can be the cause of _____ creating a complication of wound healing. Infection Edit 79 If a patients abdominal incision eviscerates what must you do as a nursing intervention? Apply moist saline and sterile gauze, notify surgeon/physician and do not attempt to reapply organs internally. Edit 80 The partial/total separation of layers usually occurring 3-11 days after injury is known as what? Dehiscence Edit 81 The total separation of wound layers; protrusion of visceral organs through a wound opening. Evisceration Edit 82 A clear drainage (water plasma liquid portion of the blood) Serous Edit 83 Thick yellow green tan or brown drainage, that contains white blood cells and bacteria Purulent Edit 84 Pale red watery mixture of clear and red fluid drainage Serosanguineous Edit 85 Bright red drainage (bleeding) Sanguineous Edit 86 If a wound is infected what must be present? Purulent drainage Edit 87 Redness, edema, heat, pain, loss of function are all cardinal signs of ____. Inflammation Edit 88 P&P:PAGE 654 Table 34-35 KNOW WBC COUNT Edit 89 You are changing a patient's wound dressing. There is an increased amount of exudate, pallor of wound bed, and a delay in healing. What is this signs of? Infection Edit 90 Contaminated or traumatic wounds usually show signs of infection when? 2-3 days Edit 91 Surgical wounds show signs of infection when? 4-5 days post-op Edit 92 When obtaining a culture of wound drainage what is the procedure? Cleanse first Collect form wound base, not drainage Differentiate aerobic v anaerobic Use Sterile technique (swab tip touches ONLY area to be cultured and inside of culturette) Edit 93 Why is nutrition essential for wound healing? Protein: essential in wound healing and cellular growth Tight Glucose control: **Diabetes** Edit 94 Body build is essential because... For the slightly fluffy type, excess skin/adipose tissue may be of a complication to heal quickly and efficiently. Edit 95 Why is oxygenation essential for wound healing? Anygiogensis and epithelialization Edit 96 When assessing a wound, what should one take note of? Location, size Amount of drainage, color, consistency Wound base- type tissue Any tunnel or undermining Wound margins Surrounding tissues Signs of infection Progress toward healing Edit 97 For wound cleansing, Hydrogen Peroxide is the best solution to use in homes and clinical settings. T/F False: Hydrgen Peroxide is a cytotoxic solution. Complicates wound healing. Edit 98 What are the four methods of debridement? Autolytic Enzymatic Mechanical Sharp Edit 99 When an enzyme is placed on top of a necrotic tissue. Enzymatic Edit 100 Nurse using a wet to try dressing to remove the necrotic tissue Mechanica Edit 101 When a physician uses the assistance of a scapule to physically remove necrotic tissue from a wound. Sharp Edit 102 What is the purpose of a dressing over a wound? Protect; aid in hemostasis; promote healing (absorb drainage, debridement); Support/splint; protect pt from visualization; promote thermal insulation; Provide moisture between wound & dressing; and remove excess moisture. Edit 103 What is a good dressing? It will remove excess exudate from a wound, won't allow wound to dry by keeping moist enviroment. Allows proper gas exchange, and thermoregulation. Minimize contamination, be non-traumatic and not adhere to the wound. Edit 104 DIABETES Mellitus Edit 105 This is a group of conditions characterized by relative or complete lack of insulin. It can also be characterized by defects in insulin cell receptors as a result in disturbances in metabolism of carbs, proteins, & lipids. Diabetes Mellitus Edit 106 What type of Diabetes is most abundant in adults and children? Type 2 Diabetes (90%) Edit 107 This is a chronic condition that often results in damage to organs and other pathological/disease states. (Silent Killer) Diabetes Mellitus Edit 108 What are the diagnosis criteria for type 1 Diabetes Mellitus? 1) Present with symptoms of 3 P's 2) Causal plasma glucose >200mg/dL 3) Flasting plasma glucose >/= 126mg/dL & confirmed by repeat on another day+1 P's is preferred method 4) 2 hr plasma glucose >/= 200 mg/dL during OGTT Edit 109 What are the 3 P's? Polydipsia Polyuria Polyphagia (Sudden weight loss) Edit 110 In this type of diabetes, there are damage caused to the beta cells of pancreas that's thought to be result of autoimmune response caused by Genetic predisposition, viral infections, environmental stimuli, and islet cell autoantibodies are present. Type 1 Diabetes Edit 111 a naturally occurring polypeptide hormone secreted by the beta cells of the islets of Langerhans in the pancreas in response to increased levels of glucose in the blood as well as the parasympathetic nervous system and other stimuli. Insulin Edit 112 characteristic signs of diabetes mellitus, including increased desire to eat, excessive thirst, increased urination, and eventually lethargy and weight loss Insulin Edit 113 How does one manage type 1 diabetes? Intensive therapy; admin of insulin>3xday; dietary intake; anticipate exercise. Conventional therapy: Admin of insulin 1-2xday, self monitoring of urine or blood glucose 1x day, client education on diet & exercise. Edit 114 This is an abnormal accumulation of ketones in the body caused by excessive breakdown of fatty acids. Ketosis (develops in the absence of adequate metabolism of carbs...as in diabetes Type 1) Edit 115 The diagnosis criteria for type 2 diabetes in adults is? 2hr plasma glucose >/=200mg/dL OGTT (or any other tests as for Type 1) Edit 116 What is the diagnosis criteria in Type 2 diabetes in children? Overweight & any of the following: 1) Family history of type 2 in 1 or 2 relatives 2) Native American, African American, Hispanic American, Asian-American/Pacific Islander 3) Signs of insulin resistance or conditions associated w/insulin resistance; acanthosis nigricans, HTN, dyslipidemia, or PCOS. Edit 117 A patient states he is at the clinic at least 3-4times a week due to UTI they are always thirsty and urinate frequently. What are these clinical symptoms of? Type 2 diabetes Edit 118 Hyperpigmentation, thickening of the skin and PCOS Edit 119 What is the number 1 factor for type 2 diabetes in children? Obesety Edit 120 Who is more susceptible to diabetes? Girls (ratio is 1.7-1) (Maturity Onset Diabetes of the Young; Type 2) Edit 121 Cells do not accept insulin; increased resistance r/t altered cellular metabolism & intracellular postreceptor defect Insulin resistance Edit 122 Insulin secretion may be normal or decreased Insulin secretory defect in Type 2 Edit 123 Are islet cell antibodies present in Type 2 diabetes? No Edit 124 What is the conventional therapy for managing type 1 diabetes? Admin of insulin 1-2xday; self monitoring of urine or blood glucose 1xday; client education on diet & exercise. Edit 125 If blood sugar is greater than 300 or if there is presents of ketose in the urine output should a diabetic exercise? No, <300mg/dL. (body is not taking sugars in to provide for the strength to exercise) Edit 126 This is a risk factor for type 2 diabetes that produces insulin resistant states causing beta cells to produce excessive amounts of insulin. OBESITY Edit 127 How can Type 2 diabetes be managed? Oral agents, exercise, insulin, and diet. Edit 128 What are the criteria for the use of insulin? Severity f diabetes: degree of hyperglycemia & presence of physical symptoms Comorbidities: severity of other diseases may make noninsulin options less successful Client: preference/compliance Edit 129 Risk for distrubed thought process, for impaired skin intregrity, for infection and for injury are all nursing diagnosis for? diabetes Edit 130 You notice your diabetic patient's change in behavior as more erratic, confused and trembling, shaking with cool clammy skin and a pale skin tone. You find the patient's food tray on the floor. What are these signs of? Hypoglycemia Edit 131 What are the signs and symptoms of Hyperglycemia? Polyuria, polydipsia, and headache. Edit 132 Life threatening insulin deficiency Diabetic Ketone Acidosis Edit 133 In management of a chronic condition of diabetes, what lab test is done to evaluate progress? Hemoglobin A1C Edit 134 This term is used broadly to include the stomach, duodenum and jejunum. "within the small intestine" Enteral. Edit 135 Decompression of the stomach through removal of contents using intermittent suction is known as what action? Apsiration Edit 136 What would cause you to aspirate enteral tubes? Remove stomach contents due to obstruction in intestine, or after abdominal surgery to allow bowel to function and anesthesia to wear off. (Rational for both is to prevent aspiration into lungs) Edit 137 Why is it essential after surgery to allow bowel to start passing gases and even movement? Anesthesia has caused bowels to stop and should wear off to prevent patient aspiration into lungs and decrease pressure on a surgical site. Edit 138 What is the process of lavage of the stomach to stop gastric/esophageal bleeding? Iced normal saline is placed into the tube using a 50-60cc catheter tipped syringe, and then removed. Repeat his process until bleeding stops Edit 139 The process of lavage of the stomach to remove poisonous medications from the body? Normal saline is placed into the tube using a 50-60cc catheter tipped syringe, and then removed. Repeat. Edit 140 This is the use of a special ballooned enteral tube to stop hemorrhage from gastric ulcers or esophageal varices. Compression of Stomach or Esophagus Edit 141 This is the use of an enteral tube to provide adequate nutrition & insure medication delivery directly into the stomach or small intestine when individuals are unable to eat in the usual manner. Feeding & Medication Administration Edit 142 What are the reason for the use of an Enteral Tube? 1) Decompression of the stomach through removal (aspiration) of contents using intermittent suction 2) Lavage of the stomach 3) Compression of Stomach/esophagus 4) Feeding and Medication Administration Edit 143 Salem Sump, and Levine tubes are what type of enteral tubes? Nasogastric Tubes Edit 144 When sterile objects touch another clean object it still remains sterile. T/F False: ONLY sterile to sterile Edit 145 When you lose range of vision of sterile objects/field what have you done? You have "contaminated that object/field. Edit 146 What happens to sterile object/field the longer it is exposed to air? It becomes contaminated Edit 147 When removing staples from a patient, you notice the TPCN cleans the site then remove the staples away from the skin from top to bottom, one after the other. What do you take note of? The TPCN should have removed everyother staple for proper precautions toward possible dehiscence. Edit 148 After removal of staples what should be documented? Sutures removed Objective description of incision line Instructions Patient response Edit 149 When removing Interrupted sutures you should cut beneath the knot and pull with forceps at the opposite end of the knot. T/F False: Grasp the knotted end with forceps. Snip the suture close to the skin surface opposite the knot and in one smooth pull, remove the suture. Edit 150 The function of this organ plays a role in immune function, internal organ protection, temperature control of the body, provides sensory perception, assists in maintenance of fluid and electrolytes and communication of feelings (body image). Skin Edit 151 What are the classic signs of inflammation? Redness Edema Heat Pain Loss of Fxn Edit 152 What must be present for an infection to have occurred? Purulent drainage must be present Edit 153 Your patient is running a temperature of 102.5. You've administered ASA as ordered and start with a dressing change on an abscess on the left hip. You notice tenderness as you remove dressing and also a foul odor. What do you expect to see after the removal of dressing? Purulent drainage due to an infection. Signs: Tenderness Fever Foul odor Edit 154 This is a complication of wound healing that is an abnormal passage between 2 organs or between an organ & the outside of the body. Fistula Edit 155 This is a complication of wound healing that is an abnormal passage away from wound base that is not connecting to another wound, organ or outside. Tunnel Edit 156 What are some factors impairing wound healing? Nutrition, Age, Body Build, Impaired O2, smoking, diabetes, drugs, radiation, wound stress, psychosocial impact Edit 157 Nutrient availability, moisture level, cleanliness, skin integrity, comorbidities, txmts, cause and severity of injury are all an influence for _______. Wound Healing. Edit 158 When assessing a wound what should you note? Location, size Amount of drainage, color, consistency Wound base – type tissue Granulation, slough, eschar % Red, yellow, black Moisture content – moist, wet, dry Any tunnels or undermining Wound margins Surrounding tissue Signs of infection? Progress toward healing Edit 159 This assessment tool helps you assess the size, depth, undermining, necrotic tissue type & amount, exudate type & amount, peri-wound color, edema, induration, granulation and epithelialization. Bates Jensen Wound Assessment Tool Edit 160 This is the removal of necrotic material/tissue. Debridement Edit 161 ? Gauze, nonstick dressing Edit 162 ? Film dressing Edit 163 ? Hydrocolloids dressing Edit 164 ? Foam dressing Edit 165 What must you do prior to changing a dressing? ALWAYS Check doctor’s order Explain procedure to patient Establish what equipment is needed Provide privacy and Provide comfort Use sterile technique (in hospital or for all acute wounds) Wash hands before & after Assess wound as previously discussed Document Edit 166 Hourly urine output of 30cc/hr is considered ___. Abnormal (poor kidney fxn may result in anemia and impaired calcium absorption. Edit 167 What is the normal output of urine per day? 1500-1600cc Edit 168 This is composed of the glomerulus, Bowman's capsule, proximal convoluted tubule, loop of Henle, distal tubule and collecting duct. Nephron Edit 169 Name the Location, Size, Fxn, Secretions, and what it Regulates. One On each side of vertebral column, lower back. Approximately 2inches in length Fxn: filters water, glucose, amino acids, urea, creatinine, and major elevtrolytes in blood forms urin in the nephron. Secretes:erythropoietin which stimulates production of RBC's in the bone marrow and it regulates calcium and phosphate. Edit 170 The kidney is perfused by what artery/vein? Renal Artery Edit 171 This connects kidney to bladder and is approximately 5 inches in length and transport sterile urine to bladder. Ureters Edit 172 How do the ureters enter the bladder? Obliquely which reduces potential for urine reflux into the kidney. Edit 173 Urine moves in a continuous drip. T/F False: Urine moves in peristaltic waves Edit 174 This organ is located in the pelvic cavity behind the symphysis pubis and its function is to act as a receptacle for urine. Bladder Edit 175 What is the normal volume held by the bladder? Normal volume 600mL and decreases with age to 250mL Edit 176 What is the difference in location of the bladder between a man and a woman? In men, it rests against the anterior wall of the rectum, whereas a woman's rests against the anterior walls of the uterus and vagina above the deltrusor muscle. Edit 177 The size of the bladder is in comparison to the size of ___. you fist. Edit 178 This is located in the inferior aspect of the bladder and its function is to as a conduit connecting bladder to outside of the body. Urethra Edit 179 What's the difference in the size of a woman's urethra to a man's? Women 1.5-2.5inches in legnth. Men 8 inches in legnth. Edit 180 What assists in the removal of bacteria from the urethra? Turbulent Flow Edit 181 Explain the process of urination. (The brain may inhibit the urge to void or allow voiding) Bladder contracts--> Relaxation of the urethral sphincter--> Contraction of the deltrusor muscle. Edit 182 When assessing a patients urine what should you note? Color, Clarity, Odor, & Amount Edit 183 UA, Specific Gravity of Urine, C&S, 24hr Urine, BUN, Cr are all lab assessments related to ____. Renal System Edit 184 Classification of diseases that affect the renal system by decreasing blood flow to and through the kidney is ... Pre-renal disease Edit 185 Renal disease is a classification of diseases that affect the conditions of ____. The Kidney Edit 186 Classification of diseases that affect the renal system with obstruction that occurs below the kidney preventing urine flow through the system is ... Postrenal disease Edit 187 While Assesing this factors influence on Urination you will find that it is associated with the development of end stage renal disease (ESRD) and uremic syndrome. Diabetes Mellitus Edit 188 Multiple sclerosis is an example of what disease condition that influences urination? Post Renal Disease Edit 189 Heart Failure is an example of what disease process that influences Urination? Pre-Renal Edit 190 This is the spectrum of symptoms that accompany uremia such as blood in the urine. uremic syndrome Edit 191 Benign Prostatic Hyperplasia is an example of this disease condition that influences Urination. Post Renal Disease Edit 192 This is a nonmalignant, noninflammatory enlargement of the prostate, most common among men over 50 yrs of age. Progressive and may lead to urethral obstruction and to interference with urine flow, urinary frequency, nocturia, dysuria, and UTI. Benign Prostatic Hyperplasia Edit 193 This disease decreases cognitive awareness of a full bladder resulting in overflow incontinence. Alzheimer Disease Edit 194 What are some common renal system diagnostic tests? Renal Ultrasound Intravenous Pyelogram (IVP) Abdominal Xray (KUB0 Post Void Residual Edit 195 These are some other Nursing Assessments to Consider for Urination Elimination. Sociocultural Psychological Fluid Balance Surgical Procedures Medications Diagnostic Examinations History of Pregnancy Limitations in Mobility Edit 196 What are some good health promotional interventions you could teach the patient about regarding urinary elimination? Teach the Patient about Risk Factors r/t Disease Teach the Patient about prescribed medications Maintain Hydration to flush bladder of pathogens Reduce Caffeine in Diet (tea, coffee, colas and chocolate) that prompts diuresis Insure Hygiene to reduce pathogen access Teach Kegel exercises to strengthen muscle tone Maintain Mobility to get to the bathroom Ingestion of Cranberry or Blueberry Juice Timely Toileting Edit 197 Give me examples of Nursing Diagnoses for urinary elimination. impaired, related to incontinence as evidenced by dribbling urine, frequent trips to the bathroom at night and history of an enlarged prostate. Edit 198 What are some common alterations in Urinary elimination? Urinary tract infections Urinary retention Urinary incontinence Urinary diversions Edit 199 Renal System Equipment Guidelines for Procedures (REVIEW PPT) Strict handwashing before and after procedure Use gloves when in contact with body fluids Place patient in position of comfort before starting procedure Check date on outside of equipment packaging to insure it is sterile Do not use packaged items that have been opened Explain to the patient what you are going to do before starting the procedure If you contaminate your sterile field-start over. Edit 200 What is the purpose for NG intubation? Decompression through aspiration of gastric contents Lavage with normal saline for gastric bleeding or removal of poisonous substance Hypokalemia, Enteral feeding or medication administration for a short period of time, usually 1-2 weeks Who is able to perform an NG Tube placement and what is required to do so? RN or LVN is able to place one with a Dr.'s Order Edit 202 When measuring the length of an NGT for placement one should ... Use the tip (end of the catheter with vents), measure from the tip of the patients nose to the earlobe. Hold your fingers on the measurement above, then add measurement from earlobe to xiphoid process. Add six (6) inches to this measurement for stomach location. Mark the NG tube with tape or sharpee pen as indicator for individual patient placement. Edit 203 You should add 6inches of length to the NGT from the Auxillary Process. T/F False: Add 6inches from the Xiphoid process. Edit 204 You have successfully placed the NG tube without complications. You check the pH of the aspirated fluids and find a result of 7.0. What do you do next? Remove the NG tube. A pH of 7 indicates the tube is placed in the lungs. (pH of 4.0 is gastric contents Edit 205 What is the most adequate way to check placement of an NGTube? X-ray Edit 206 If patient starts coughing or gaging in the process of placing the NG tube you should? stop pull back then proceed after they stop coughing. Edit 207 Your patients meds are about time to be given but they now have an NG tube. You notice on the med the markings SR. What do you do next? You call the doctor and request for another form of that medicine to give either liquid or injection form. SR is a slow release med that can not be crushed. (TR, SR, ER, ER) Edit 208 What are some common nursing Diagnoses related to NG Tube? Nausea related to gastric distention (secondary to pancreatitis) as evidenced by refusal of food, report of gagging sensation Risk for deficient fluid volume related to vomiting (secondary to GI bleed) Imbalanced Nutrition: less than body requirements related to inadequate food intake (secondary to anorexia nervosa) as evidenced by 900 calorie intake on calorie count, albumin of 2.5. Edit 209 The clinical manifestations of this disease is gradual onset of polyuria, polydipsia, easily fatigued, and frequent infections (UTI). Often discovered w/diagnosis of comorbidity. Type 2 DM Edit 210 Why is obesity a risk factor for DM Type 2? Obese people produce insulin resistant states causing beta cells to produce excessive amounts of insulin. Edit 211 What are some medical diagnoses associated with enteral nutrition? Cerebrovascular Accident (stroke) resulting in dysphagia Esophogeal Cancer requiring surgery Head and neck cancers requiring radiation treatments Facial trauma from a motor vehicle accident Edit 212 This Enteral tube enters into the stomach. It is a hard plastic, usually used no longer than 2 weeks, and is inserted by RN or LVN. Residual should be checked before any feeding or medication administration and document amount. Check pH for placement (pH 4.0) Nasogastric Tube (salem Slum, Levine) Edit 213 This Enteral tube enters through abdomen into stomach. It's held in place by a balloon/water combo. Inserted by physician under flouroscopy. Residual checked before any feeding or medication administration and document amount. (pH 4.0) Gastrostomy Tube Edit 214 This Enteral tube enters into duodenum through nose or mouth. Soft plastic, weighted at the end, x-ray for placement. Inserted by physician. No residual check, collapses with manipulation. Considered lower risk for aspiration from this location. Moved into duodenum by peristalsis. Position for advancement of tube. Duodenal Tube (Dobhoff) Edit 215 This enteral tube enters into jejunum through abdominal approach, then sutured in place. Soft plastic. No residual check as there is only a small space in intestine for pooling of contents. Considered lowest risk for aspiration into lungs from this location. Inserted by physician under flouroscopy. Jejunostomy Tube Edit 216 This is the use of a pump to deliver nutrition over 12 hrs or 24hrs. Ordered by physician as cc/hr x number of hours. Continuous feeding Edit 217 This is method, a nurse administers using gravity (bolus) and 60cc syringe. Liquid feeding is poured into the syringe, plunger is removed. The higher syringe is held, the faster the flow. Intermittant Edit 218 A patient is on tube feeding and you noticed the patient is soiled so you act to clean them. What do you do? You turn off tube feeding and lower the head to proceed with cleaning. After you've completed, raise patient to fowlers position from 30-45degrees than start feeding. (prevents patient from aspiration) Edit 219 What is the pH of the gastric, intestine, and lung content in exact order? 4.0; 5.0; 7.0; Edit 220 When should you check the residual of a patient with a enteral tube? You should check residual every 4hrs and before meds are give. Edit 221 When should you hold tube feeding? When lowering patient below 30 degrees and if residual is >100mL or double hourly infusion than you should hold feeding Edit 222 If output of enteral tube decreases due to thick secretions, what should you us to dislodge obstruction? Cola or cranberry juice Edit 223 After checking the residual on your patient you notice there is 200mL more than the last time you have check. What should you do with the fluids? return residual to prevent electrolyte imbalance Edit 224 _____ Commercial formula is specific for patients on enteral feedings with respiratory conditions while _____ is for renal conditions. Pulmocare / Nepro Edit 225 This nutritional product for enteral feeding adds calories or proteins, but is not intended to provide entire caloirc intake. Supplements Edit 226 This enteral nutritional feeding usually is prepared by family when patient is living in home setting. Blenderized Edit 227 This occurs with hyperosmolar solutions-formulas high in electrolytes and carbohydrates. Fluids are drawn into the formula from the vascular system through osmosis rapid distention of location in GI tract resulting in cramping and diarrhea. Dumping Syndrome with Enteral Feedings Edit 228 How do you prevent dumping syndrome from occurring due to enteral feedings? Assess patient to rule out other reasons for diarrhea Slow down formula administration (may be issue in intermittent feedings performed by nurse) Administer feeding at room temperature Consider amount of enteral flushes used by nurse administering the feeding Report dumping syndrome and discuss continuous versus intermittent feedings with dietician/MD. Edit 229 What are some gastrointestinal strategies one could implement to minimize complications of Enteral Feeding? Room temperature formulas to prevent gastric cramping Monitor gastric residual to prevent vomiting/aspiration Appropriate fiber & water content to promote hydration and bowel function Edit 230 What are some mechanical strategies one could implement to minimize complications of Enteral Feeding? Check tube placement to reduce aspiration risk HOB elevated 30-45 degrees to reduce aspiration risk Check residual q 4 hours, and before feeding/meds Prevent kinks in tubing to insure delivery of feeding/meds Insure pump is set correctly to deliver nutrition as ordered and prevent fluid overload Edit 231 What are some metabolic strategies one could implement to minimize complications of Enteral Feeding? Monitor blood glucose levels daily to insure patient safety I&O every shift to prevent dehydration or fluid overload Assess feeding rates/formulation and document every shift Provide oral hygiene every four hours Monitor breath sounds every four hours Edit 232 When gastrointestinal tract cannot be accessed for an extended period of time, what is the alternative route for delivery of nourishment? (TPN) Total Parenteral Nutrition or (HAL) Hyperalimentation (requires Central line access) Edit 233 What should be monitored while a patient is on TPN or HAL? Based upon daily blood draws for electrolytes, liver studies, renal panel, albumin, glucose Requires accuchecks every 4-6 hours to monitor glucose (TPN/HAL utilizes 10-50% glucose solution) More expensive, more invasive, than enteral feeding High glucose content places patient at high risk for infection-monitor for signs and symptoms May not add any other fluids, medications or blood products through this “dedicated” intravenous line Edit 234 What are some common nursing diagnoses associated with enteral tubes? Imbalanced Nutrition, less than body requirements related to difficulty swallowing as evidenced by prolonged length of time food is in the mouth without swallowing, coughing while eating, loss of 10 pounds in two weeks. Nausea related to gastointestinal irritation as evidenced by report of vomiting at home, potassium (K+) of 2.5, and inability to consume food and fluids.