Psychopharmacology - Where can my students do assignments that
advertisement

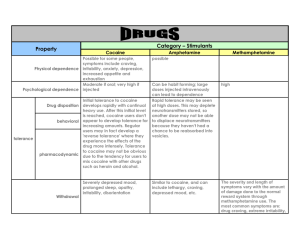
• Psychomotor stimulants – Cocaine – Amphetamines – but also – nicotine and caffeine • Cocaine is a compound found in the leaves of the shrub Erythroxylon coca. – Native to South America • Local inhabitants consume cocaine by chewing leaves. – going back 2000-5000 years • Coca chewers often combine the leaves with lime or ash – This promotes absorption • Late 1850s German chemists had isolated pure cocaine • Became immensely popular over the next 30 years • Probably the most famous advocate was Sigmund Freud • By 1885 Parke Davis & Co. pharmaceuticals was manufacturing 14 different forms of cocaine • 1886 John Pemberton introduced Coca-Cola • Cocaine containing tooth drops were even given to infants when teething – Cocaine is a local anesthetic • 1914 Harrison Narcotic Act was the beginning of restrictions on cocaine – Over time more and more restriction were put into place • From the 1920s-1960s cocaine was limited among a small group of artists, musicians, and other performers • 1970s was the first wave of cocaine use increase – snorting cocaine • 1980s (second wave) – crack cocaine • About 2 million people reported being current users (within the previous month) • About 6 million within previous year • 34 million (14% of population) used at least once during lifetime • Coca leaves contain about 0.6-1.8% cocaine • Initial extraction of the leaves results in a paste that is about 80% cocaine • Then converted to cocaine HCL a crystallized version – Readily water soluble • Can be taken orally • Intranasally • IV • Cocaine HCL is vulnerable to heat so that ruled out smoking – Can be converted back to cocaine freebase • Old way – – – – – Dissolve cocaine HCL in water Add alkaline solution (ammonia) Extract cocaine with an organic solvent (ether) Freebasing refers to smoking cocaine obtained this way Ether is highly flammable • Preparation and smoking is dangerous • New way – Mix dissolved cocaine HCL with baking soda – Heat and then dry – Chunks of cocaine known as crack • Popping noise when smoked. 11.5 Crystals of crack cocaine • The different routes of administration yield somewhat different levels of plasma cocaine • Smoked probably an understimate – 1-3 puffs of vapor heated in a flask • A few hours of coca leaf chewing produces plasma concentrations equivalent to a modest dose taking intranasally or orally • Cocaine is fat soluble – Passes readily through the blood-brain barrier • When smoked the brain is exposed to a very large surge in the brain that is not reflected in the peripheral venous system • Once absorbed into circulation cocaine is rapidly broken down by enzymes in the bloodstream and liver – Half life 0.5-1.5 hours – Thus, subjective high is brief • Smoking may produce only a 30 minute high – The breakdown products can persist longer • Benzoylecgonine and be detected in urine for a number of days following the last dose in a heavy user • Cocaine is often taken with depressant drugs to take the edge off the extreme arousal produced by cocaine alone • Cocaine and alcohol when taken together produce a unique metabolite called cocaethylene – Has biological activity similar to cocaine – Has a longer half life • The combination of cocaine and alcohol may increase the toxic effects of cocaine on the heart and other organs • Cocaine interacts with several neurotransmitter systems • Blocks the reuptake of three monoamine neurotransmitters – Dopamine – Norepinephrine – Serotonin • Binds to and blocks the transporter • Cocaine does not affect all monoamine transporters equally • Has highest affinity for 5-HT transporter, followed by DA transporter, and NE transporter • Nevertheless, it is blockade of the DA transporter that plays the biggest role in the stimulating, reinforcing, and addictive properties of cocaine • Many drugs used to treat depression block the 5-HT and NE transporter – Do not have strong arousing effects – Do not have abuse potential • At high concentrations cocaine inhibits voltage-gated NA+ channels in nerve cell axons – Blocks conduction – Produces local anesthesia • Novocaine (procaine) • Xylocaine (lidocaine) – Developed from cocaine Acute behavioral effects of cocaine • Cocaine high (mild to moderate effects) – – – – – – Feelings of exhilaration and euphoria Sense of well being Enhanced alertness Heightened energy Great self confidence Smoking produces a “rush” • Intense sense of great pleasure and power – Increases sociability and talkativeness – Heightened sexual interest – Can increase aggression Note – how the effects become more negative as dose and duration of use go up. • Cocaine can cause psychosis at high enough doses (we’ll talk more about this later). • Cocaine affects the behaviors of other animals as well • Lab mice and rats are activated by low doses of cocaine – Locomotion – Rearing – Sniffing • Higher doses are replaced by focused stereotypies – Stereotypy to stimulants in rats and mice • • • • Intense sniffing Continuous head and limb movements Licking Biting – Humans sometimes show stereotypy as well • Repetitive picking and scratching • All animals tested so far readily learn to self-administer cocaine I.V. • Monkeys have been trained to smoke cocaine freebase • If cocaine is made freely available the animals health deteriorates – High mortality rates – Points to the powerful reinforcing properties of the drug • Animals trained to discriminate cocaine from vehicle readily learn – Learning generalizes to amphetamine • Indicates the two drugs are similar – Much less generalization to caffeine • Indicates the two drugs are not as similar. • Cocaine is considered a sympathomimetic drug – Produces symptoms of sympathetic nervous system activation • • • • Increased heart rate Vasoconstriction Hypertension Hyperthermia • At low doses these effects are usually not harmful. • At high doses these effects can be fatal – Seizures – Heart failure – Stroke • Intracranial hemorrhage 11.8 Computerized tomographic (CT) scan of a thalamic hemorrhage in a crack cocaine smoker DA plays a key role in the subjective and behavioral effects of Cocaine • Dopamine plays a central role in the behavioral response of animals to cocaine and amphetamine • Table 11.2 • Note in Table 11.2 (previous slide) that amphetamine but not cocaine microinjected in the nucleus accumbens is reinforcing (Goeders & Smith, 1983) – Surprising finding – Not known why • Differences in how cocaine and amphetamine work at the synapse? • Anesthetic effects of cocaine? • Subsequent work points to different regions of nucleus accumbens • There is evidence that rats will Self administer in to the NA shell rather than NA core (Rod-Henricks et al, 2002). Knock out mice • More recently the neurochemical mechanisms of cocaine action have been studied in genetic knock out mice • Led to some confusing results • May say more about the knock out model than about the mechanism of cocaine • Notice in the next slide that knockout mice for the dopamine transporter, still self-administer cocaine. – FR 2 schedule • This finding implies that the DAT is not the only mechanism of reward. – Could be true • Also could be that knockout mice adapt to the lack of dopamine transporter • There is some evidence that serotonin blockade may play a greater role in the reinforcing effects of cocaine in knockout mice – Fluoxetine (Prozac; 5-HT reuptake inhibitor) doesn’t support selfadministration in wild-type mice • Does in knock out mice – Fluoxetine also was found to stimulate DA release in the mesolimbic pathway • in knock out mice; but not in wild type mice • Adds to already high levels (because no DAT) • Perhaps this mediates reward Neural mechanisms of psychostimulants in humans • Brain imaging studies show that once a certain minimum level of DAT occupancy is achieved (40-60%) the subject may experience a “high” – Studied with PET scan • [11C]d-threo-methylphenidate – a radiotracer which binds rapidly to the DAT in vivo • See how much cocaine (or methylphenidate) reduced [11C]d-threo-methylphenidate binding – Use methylphenidate, which also binds to DAT because it can be used in participants that have not previously used cocaine • The intensity of the high depends on two other things besides drug occupancy of DAT – 1) The rate at which the transporter occupancy occurs • IV and smoking = quick occupancy – More intense high – 2) The baseline of DA activity • If DA release is low – blockade of DAT may not have that much of an effect • If DA release is high – blockade of DAT seems to have a much greater effect – See next slide. • May explain individual differences in the high that people feel – Some subjects with 60% DAT occupancy failed to report a high » Perhaps they have low baseline DA levels The role of DA receptor subtypes in the effects of psychostimulants • There are 5 different subtypes of DA receptors – D1 and D5 (D1-like family) – D2, D3, and D4 (D2-like family) • Studies have shown that antagonism of D1-like or D2-like families can reduce behavioral activation and reinforcing properties of psychostimulants – Nonselective antagonists • So we don’t know which member or members of the families are actually controlling the effects Genetic knockouts and cocaine • Knockout mice lacking D1 receptors – Are not activated by cocaine – Won’t self-administer cocaine • Though they will work for food and for opiates – Caine et al. (2007) » Also blocked self-administration of D2 agonists • Knockout mice lacking D2 receptors – Are activated by cocaine – Do self administer cocaine • What do the results on the previous slide mean? – D1 receptors may play a bigger role in the activational and rewarding effects of cocaine than do D2 receptors – Perhaps D1 receptors play a permissive role for Dopamine agonists (Caine et al.) • This would explain why D2 agonists were not effective in D1 knockout mice D3 receptors? • D3 receptor antagonist (SB277011-A) blocks the enhancement of brain reward (ICSS) that normally occurs • Implicates the D3 receptor in rewarding properties of cocaine Cocaine abuse and the effects of chronic cocaine exposure • People usually begin taking cocaine intranasally • Most who try cocaine do not continue to a pattern of drug abuse – – – – – Some report anxiety response Availability of drug may be limited Cost may be too much Social and legal consequences Fear of addiction • Approximately 10-15% of initial users eventually become abusers • Initial use may be reinforced by the powerful rewarding aspects of the drug • Social reinforcement may also play a role – Friends enjoy newfound energy and enthusiasm • Transition to smoking or IV is often a significant event in drug history – Much greater high – Often develop cocaine binges • Bouts of drug use lasting from hours to days • Nothing is more important than maintaining the high – 3-day freebasing binge could involve consuming as much as 150 g of cocaine Tolerance and Sensitization • Psychostimulants cause tolerance, but they often also cause sensitization. – sensitization can occur after a few exposures – can last for weeks or months • Why sometimes tolerance and sometimes sensitization? – Not fully understood – Pattern of drug use may play a role • Chronic exposure (continuous infusion) – more likely to elicit tolerance • Acute exposures (once daily) – more likely to elicit sensitization • See following graphs 11.12 Chronic cocaine administration can produce tolerance or sensitization (Part 1) 11.12 Chronic cocaine administration can produce tolerance or sensitization (Part 2) Sensitization • Sensitization can increase in strength after the last drug use (that is during withdrawal). – Presumably due to ongoing neurochemical changes. • In some cases researchers have observed acute tolerance along with long-term sensitization. – Bradberry (2000) • Monkeys self administering cocaine over 6 month test period • Measured DA levels in the striatum • If the monkeys injected themselves twice during a session, – the DA response to the second dose was reduced (acute tolerance) – However, the DA response to the first dose each session gradually escalated over the 6 month period (long-term sensitization). • These acute tolerance and long-term sensitization effects may help us understand patterns of drug use in humans – The long-term sensitization may underlie the increased craving that users experience (like the incentive sensitization model we discussed in Ch 8). – Users also report that during a cocaine or amphetamine binge, they need more drug later to obtain the high they had at the beginning • Thus, there may be a short-term tolerance that wears off prior to the next binge. • Sensitization can be divided into two phases • Induction – Establishment of sensitization – NMDA receptors (glutamate) seem to be involved • Remember tolerance to opiates? • Expression – Changes in reactivity of DA nerve terminals in the nucleus accumbens seem to be involved • A given dose of cocaine causes greater increases in synaptic DA levels Health Consequences of chronic cocaine use • As we stated before a single high dose can cause a stroke or seizure • What about chronic use? – Effects on the body • Heart problems – – – – Chest pains Cardiac arrhythmias (irregular hear rate) Cardiac myopathy (damaged heart muscles) Myocardial infarction (heart attack) • There can also be adverse effects on the lungs, GI system, and kidneys. • Snorting can lead to perforation of the nasal septum Maternal Cocaine use • Effects on fetus – Not completely understood – Some children turn out okay – Others have attentional deficits – Some show Cognitive deficits – May increase prenatal mortality • The old correlation causation issue Chronic cocaine and the brain • Check out Box 11.1 in your book for an in depth discussion. • In general there is evidence that chronic cocaine use can alter DA functioning in the brain – Of course we already expected this from the animal work that showed tolerance and sensitization effects • There is also some evidence for decreased grey matter in brain areas associated with cognitive functioning – Prefrontal and temporal areas • There is some evidence that there may be behavioral consequences – Impaired verbal memory – Impaired attention – Impaired motor function • But….keep in mind…we have the old correlation vs. causation issue again. Pharmacotherapy for cocaine? • Are there drugs we can use to treat cocaine abuse? • Desipramine (tricyclic antidepressant) – – – – Mainly inhibits NE uptake Most widely used drug to treat cocaine addiction Used in adjunct with traditional therapies Used most often with those that have been diagnosed as also having depression (comorbid). – Used for those diagnosed with cocaine abuse more than the more severe cocaine dependence. • Researchers are working on developing drugs that might reduce cocaine’s euphoric effects • Partial agonists of the DA receptor especially D1 and D3 are gaining a lot of interest – Would compete with DA for access to the receptor – Would have lower efficacy – Possibly blunt the effects of cocaine • BP 897 a D3 receptor partial agonist reduces cocaine-seeking in rats – Is currently in clinical trials Cocaine vaccine? • Animals can be immunized against cocaine – Create antibodies that attack the cocaine molecule – Less cocaine will get to the brain – Seems to work with animals (see following figures). • Has been tried with humans, but the antibodies gradually disappeared over time 11.14 Reduction in behavioral responses to cocaine in vaccinated (immunized) rats (Part 1) 11.14 Reduction in behavioral responses to cocaine in vaccinated (immunized) rats (Part 2) Amphetamines • Amphetamine is the parent compound of a family of synthetic psychostimulants • True amphetamine comes in 2 forms – 1-amphetamine (Benzedrine) – d-amphetamine or dextroamphetamine (dexedrine) • Other members of amphetamine-like psychostimulants – – – – Methamphetamine 3,4-methylenedioxymethamphetamine (MDMA) 3,4-methylenedioxyamphetamine (MDA) 3,4-metheylenedioxy-N-ethylamphetamine (MDE) • As can be seen in the following slide all of these compounds are structurally quite similar to dopamine 11.15 Amphetamine and related psychostimulants History of Amphetamine • Ephedrine and Cathinone are naturally occurring plant compounds that are similar to amphetamine – chemical structure presented in previous slide • Cathinone is primary active ingredient in khat (qat) – Shrub native to East Africa and Arabia History of Amphetamine • Ephedrine comes from the herb Ephedra vulgaris. – Ephedrine (Ephedra) is obtained from the dried branches of this plant • Chinese have used Ephedra for more than 5000 years as an herbal remedy – Reduces appetite – Heightened energy • Been marketed as a weight loss product in health food stores – Was very popular History of Amphetamine • Side effects of ephedra – Elevated blood pressure – Increased risk for heart attack or stroke • In 2003 Baltimore Orioles pitcher Steve Bechler collapsed and died during spring training in Florida – Had been taking high doses of ephedra containing supplement to control weight – Coroner ruled ephedra as a likely contributor to his death – FDA banned the sale of ephedra containing supplements in 2004. History of Amphetamine • Ephedra played a role in the initial development of amphetamine • Purified ephedrine was used to treat asthma in 1920s – Pseudoephedrine is a modern decongestant • Similar compound but with less side effects – There was concern that demand may be greater than supply of the plant – Amphetamine was used as a synthetic substitute. • Smith, Kline, & French pharmaceuticals created an amphetamine-containing inhaler in 1932 • Effective treatment for nasal or bronchial congestion History of Amphetamine • Some patients began to overuse the inhalers – Often available without prescription • Contained a cotton plug which contained the amphetamine – Some folks began to open the inhalers and either chew or swallow the cotton plug, or extract the amphetamine for injection. • Amphetamine tablets were marketed in 1935 as a treatment for narcolepsy. – Amphetamines are still used for this purpose today. • 1940s amphetamine was widely embraced by medical profession – American military personnel were given amphetamine to maintain alertness and forestall sleep while on duty History of Amphetamine • After WWII there was a surge in street use of amphetamine – 1950s and 60s students used amphetamines as study aids • The peak of use occurred in early 70s – Since then cocaine use has surpassed amphetamine use – An exception to this trend is the recent upsurge in methamphetamine use Amphetamine/Methamphetamine • Amphetamine and Methamphetamine are quite similar pharmacologically • Amphetamine is typically taken PO, IV, or SC – AKA: uppers, bennies, dexies, black beauties, diet pills • Methamphetamine is more potent than amphetamine – Typically taken PO, Intranasally, IV, or smoked. – AKA: meth, speed, crank, zip, go – Smoking can be done with a glass pipe, or by heating on a piece of aluminum foil (“chasing the dragon”) Crystal Meth/Ice • Methamphetamine HCL is a crystal form that is particularly suitable for smoking – AKA ice or crystal meth • Began showing up in Hawaii in the 1980s. • Now spread to many parts of the country. – Especially west, south, and midwest • Inexpensive to make and highly addictive Patterns of use • Use of amphetamine/methamphetamine often occurs in binges “speed freaks” – Can last for days • Little sleep or eating occurs during a run – Check out “Spun” • Metabolized by the liver at a slow rate – Very long half-life, so the high from amphetamine/methamphetamine lasts much longer than that of cocaine mechanism of action (a triple whammy) • Amph./methamp. are indirect agonists of the catecholaminergic system – Enter the terminal button (via DAT) and cause release of catecholamines from terminal button – 2 mechanisms involved • 1) DA molecules are released from synaptic vesicles into the cytoplasm • 2) the dopamine transporter moves the DA out into the synapse (reverse transport) – This reverse transport prevents reuptake. – Very high doses can also inhibit monoamine oxidase Amphetamines do have therapeutic uses • Used to treat narcolepsy • Some forms are also used to treat ADHD – Low doses of psychostimulants can cause a calming effect in ADHD children – Usually combined with counseling (therapy) of some sort • Methylphenidate is available in several forms to treat ADHD – Ritalin (immediate release form) • Works 3-4 hours – Ritalin SR • Lasts 6-8 hours – Ritalin LA and Concerta • Can last an entire day • How can stimulants be calming? – Human adults given low doses of methylphenidate are more likely to show arousal and hyperactivity – But young people appear to be calmed • Some have speculated that this response is specific to children with ADHD • Other researchers have shown that even children that don’t have ADHD have increased attention and lower activity levels to therapeutic doses of amphetamine – Leading to speculation that this response to amphetamine is a general developmental phenomenon • Apparently low doses can reduce activity in young rats as well. – Kuczenski and segal (2002) – graph – Oral doses of methylphenidate during active part of cyle (night) – Not shown in graph is that high doses (5 mg/kg) caused increased activity High doses and chronic use of amphetamine • Amphetamines can cause psychotic reactions • Same sorts of symptoms that we discussed for cocaine psychosis • These kinds of effects usually require chronic high doses in order to develop. – After a few “speed runs” • Perhaps may cause “flash backs” – Triggered by stressful events – Perhaps previous drug use caused heightened stress sensitivity? Amphetamine Neurotoxicity • Animals exposed to multiple doses of methamphetamine – Long-lasting reductions in • DA levels • Tyrosine hydroxylase – Remember key enzyme in DA synthesis • Dopamine transporter – Indicates damage to DA axons and terminals • Histology experiments show degenerating axons – Also causes damage to serotonergic axons Amphetamine neurotoxicity in humans? • PET scan data indicate large losses of DAT in the striatum for previous methamphetamine users. – Doesn’t necessarily mean loss of axons, but animal data would imply that it might • Notice the lack of DAT in parkinson’s patients (PD) compared to control – Then compare the slides for methamphetamine users • Given that striatal DA activity occurs during normal aging, if nothing else these findings might imply an increased susceptibility to Parkinson’s disease MDMA (Ecstasy) • Developed by Merck pharmaceutical company in 1914 • Forgotten for decades, but reemerged in the 1970s – Some psychotherapists began to give MDMA to clients during therapy • Caused clients to communicate better • Open up their emotions, experience greater closeness and empathy for others – People began to use it recreationally • AKA: Ecstasy, XTC, Adam • 1985 the DEA made MDMA a schedule 1 drug • Psychological effects of MDMA – Produces mild euphoria – Increased energy – Enhanced sensory perception – Feelings of well being and self-confidence – Desire to interact with other people • Physical effects of MDMA – – – – – – – – Increased heart rate Increased blood pressure Elevated body temperature Sweating Salivation Tremor Tightening of jaw muscles Teeth grinding • MDMA was closely associated with Rave scene – This led to concern about heatstroke and dehydration • Could be fatal Mechanism of action of MDMA • Acts at DA and serotonin neurons – Enhances release and blocks reuptake of both NTs • The primary mechanism of action appears to be activation of the serotonergic system. – Probably explains the subjective and physiological differences between MDMA and amph./methamp. MDMA toxicity? • Animal studies – Repeated high doses have been shown to damage serotonergic pathways in the brain • Decreased serotonin levels and pruning (loss of terminal button branches) of serotonin axons in the the cortex and hippocampus – There is evidence of regrowth, but the regrowth is not always normal • Some show long lasting deficits (see next figure) • Some studies have actually shown development of excessive serotonergic input • • • Monkeys stained for serotonergic neurons in neocortex Control monkey – left column Middle column – 5 mg/kg MDMA twice daily for 4 days • Sacrificed 2 weeks later • Right column – 5 mg/kg MDMA twice daily for 4 days • Sacrificed 7 years later • From what I can gather – (don’t hold me to this). – A pretty high dose for humans • About 2.5 mg/kg – Typical dose? • About 1-1.5 mg/kg • Does this sort of toxicity occur in humans? – Critics say pretty high doses in animal studies • Humans may not typically expose themselves to such levels – However, there are signs of deficits in heavy users • • • • Reduced 5-HIAA (principle metabolite) of serotonin Decreased 5-HT transporter density Some signs of cognitive deficits Decreased performance on memory tests – Again…..correlational (poly drug use; preexisting conditions) – Also typically study people that are chronic heavy users of MDMA – Hard to say what the long-term effects of a few doses of MDMA are.