Neurology System
advertisement

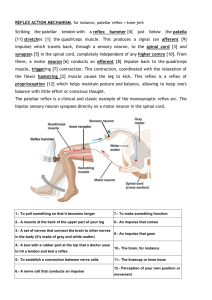
Neurology System Reflexes Reflex Arch • Spinal nerves have sensory (Afferent) & motor (Efferent) portions • Control DTRs & superficial reflexes • Simple reflex arch needs a sensory & motor neuron • Ex. Of normal reflex arch = kneejerk/patellar reflex Reflex Arch • Reflexes= basic defense mechanisms of the nervous system – Involuntary – Unconscious – Allow quick reaction to painful/damaging situations – Maintain balance – Appropriate muscle tone Four Types of Reflexes 1. Deep tendon • Patellar or knee jerk • • Corneal abdominal • Pupillary reflex to light and accommodation • • Babinski Extensor plantar reflex 2. Superficial 3. Visceral 4. Pathologic Deep Tendon Response • Briskly tap the tendon of a partially stretched • muscle For the reflex to fire, all components of the reflex arch must be intact – – – – – Sensory nerve fibers Spinal cord synapse Motor nerve fibers Neuromuscular junction Muscle fibers Deep Tendon Response • Tapping the tendon activates special sensory fibers in the partially stretched muscle, triggering a sensory impulse that travels to the spinal cord via peripheral nerve • the stimulated sensory fiber synapses directly with the anterior horn cell innervating the same muscle. Deep Tendon Response • When the impulse crosses the neuromuscular junction, the muscle suddenly contracts, completing the reflex arch. Deep Tendon Response • Each deep tendon reflex involves specific spinal segments • Abnormal reflex help locate an a pathologic lesion The Plantar Response • Normally flexion of toes • Dorsiflexion of the big toe & fanning of the other toes = Babinski Response – Indicative of CNS lesion in corticospinal tract – Babinski may also be seen in unconscious states due to drug or alcohol intoxication or postictal period Grading Reflex Response • Compare Right and Left Sides • Graded on a 4 point scale – 4+ very brisk,hyperactive with clonus – 3+ brisker than average – 2+ average, normal – 1+ diminished, low normal – 0 No response 4 point scale • Subjective • No standard exists • Wide range of normal • Advise to assess DTRs only as part of the complete neurologic exam Abnormal Findings • Clonus – Short jerking contractions of the same muscle • Hyperreflexia – Exaggerated reflex – Monosynaptic reflex arch from higher cortical levels – Brain attack • Hyporeflexia – Absence of reflex – Lower motor neuron problem – Spinal cord injury Reinforcement • Reflex response fails – Vary position – Increase the strength • Reinforcement Technique – Relaxes muscles – Enhances response – Isometric exercise in muscle group away from the one being tested sample multiple choice • During a neurologic examination, the tendon reflex fails to appear. Before striking the tendon again, the examiner might use the technique of: A. Two-point discrimination B. Reinforcement C. vibration D. graphesthesia Complete Neurologic Exam • Mental Status • Cranial Nerves II - XII • Motor System – muscle size, strength, tone, • • gait, and balance, RAMs Sensory System – superficial pain, light touch and vibration, position sense, stereognosis, graphesthesia, 2 point discrimination Reflexes – DTRs, biceps, triceps, brachioradialis, patellar, Achilles – Superficial – abdomonal , Plantar Neurologic Screening Exam • Mental Status • Cranial Nerves – II Optic – III, IV, VI Extraocular muscles – V Trigeminal – VII Facial Mobility • Motor Function- gait & balance, Knee flexion (hop or shallow knee bend) Screening • Sensory function – superficial pain & light touch (arms & legs) – Vibration – arms & legs • Reflexes – Biceps – Triceps – Patellar – Achilles Neurologic Recheck • In house patients with head trauma or neurologic deficit due to systemic disease process must be monitored closely for change in status or signs of ICP. Use this shortened form of the neurologic exam: LOC Motor function Pupillary Response Vital Signs LOC • A change in the level of consciousness is the • single most imp. Factor in this exam. It is the earliest sign. Check arousal, awareness, orientation – person, place & time. A person is fully alert when his eyes open at your approach or spontaneously, orientated x3, follows verbal commands appropriately. If not fully alert increase the amt. Of stimulus used as follows: name called, light touch on arm, vigorous shake of shoulder, pain (Nail bed, sternal rub) Motor Function • Check voluntary movement with commands (raise right arm, squeeze fingers) • If spontaneous movement occurs in reaction to noxious stimuli = Localizing, documented as a purposeful movement Pupillary Response • Size, shape, and symmetry of both pupils • In a brain injured person – a sudden, unilateral, dilated and nonreactive pupil is ominous. When ICP pushes the brain stem down (uncal herniation) it put pressure on Cranial nerve III (runs parallel to brain stem) causing pupil dilatation Vital Signs • TPR & B/P prn • Note pulse & B/P are notoriously unreliable parameters of CNS deficit. Changes are late consequences of ICP – Cushing Reflex = sudden B/P with widening pulse pressure ; pulse slow & bounding Glascow Coma Scale • Objective tool that defines LOC by assigning it a numeric value. Scale divided into 3 areas; – Eye opening – Verbal response – Motor response • Alert, normal person scores 15 • Score of 7 or < reflects coma