N 491 2010 Class 4 PHC_Nursing_Presentation_Jan 2010
advertisement

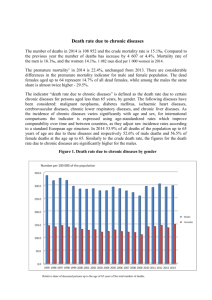
Primary Health Care Challenges and Opportunities… Jennifer Leuschner RN, BScN Manager, Primary Health Care GASHA Lost in Translation… Primary Care Primary, Secondary Tertiary Prevention Primary Health Care Population Health Chronic Disease Prevention and Management Health Promotion Health… …is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity. World Health Organization 1948 ….is a resource for everyday life, not the object of living. It is a positive concept emphasizing social & personal resources as well as physical capability evolution? We Can’t focus on Risk Factors Alone Poverty and Inequity Challenges - What ‘s wrong with the system? Too many patients are in acute care beds who should be receiving care elsewhere Too many patients with chronic illnesses develop preventable complications Too many people develop illnesses which are totally preventable We are using our human resources poorly The only determinant of health we seem to address is the health care services one Every system is perfectly designed… To achieve the results it gets. W. Edwards Deming Early Days of Primary Health Care Primary Health Care Definition Primary Health Care (PHC) is concerned with all the factors that promote health as they apply to a given population, not just personal health services. It addresses the factors that determine health such as income, social status, social support networks, education, employment, working conditions, social and physical environment, biology and genetic endowment, personal health practices and coping skills, healthy child development, gender, culture and health services These factors are addressed within a system that has appropriate linkages. PHC is developed with the full participation of the people it serves. It empowers people to take care of their own health and to take an active part in planning, policy making and delivering health care services in their community Principles of Primary Health Care Population Health Accessibility Appropriateness Intersectoral/Interprofessional Continuity of Care Community Participation Efficiency Affordable & Sustainable Primary Care Definition Primary Care is an important part of Primary Health Care and is a term used for the activity of a health care provider who acts as a first point of consultation for all patients. The aims of primary care are to provide the patient with a broad spectrum of care, both preventative and curative, over a period of time and to coordinate all of the care the patient receives. Primary Care focus on individual Selective Primary Health Care Comprehensive Primary Health Care Population Health through individuals tackles social determinants of health -Individualized clinical services -Secondary & Tertiary disease prevention -Health Education -Screening and surveillance -Immunization -Primary prevention -Health education Examples: General Practice Diabetic Clinic Heart Health Clinic Screening Programs Examples: Healthy Heart Programs Well child clinics Flu Clinics -Provision of housing, shelter, social support, food and nutrition, safe environments -Capacity building and health promotion -Health impact awareness -Harm minimization approaches -Advocacy for sustainable social and system change Examples: Youth Health Centres Healthy Public Policies Food Security work The WHO recognizes that only a comprehensive primary health care approach will actually improve the quality of life and health outcomes of people in any society and that Primary Health Care must be modified to suit the differing needs of population groups. Nova Scotia Priorities Improving access to PHC services Increase the emphasis on health promotion and wellness Providers working in teams Electronic Patient Record (EPR) Opportunities • Primary prevention to avert illness entirely • Screening initiatives • Chronic disease management to decrease acute episodes • Chronic Disease Self Management • New Providers • Success Opportunities cont’d PHCTF – paid to get change started Recommendations of a $1.0 M report in NS ….PHSOR report …..(many more) PHC in GASHA: the history Sheila Sears hired in 2003 (PHC Transition Fund) GASHA is innovative in finding money for projects – (AHTF, Drug Company $, Literacy $) Roll out of NPs GASHA hired first NP in 2005 – both clinical and community components Approx 40 initiatives in our DHA in the first few years LHCW, EMR, Cardiac Clinic, YHC Arichat Our GASHA PHC team 4 NPs 1 RN Dietitian Behaviour Motivator Coordinator AHTF coordinator Clerical support Physiotherapist …team is growing Role of the nurse in PHC Population Health Accessibility Appropriateness Intersectoral/Interprofessional Continuity of Care Community Participation Efficiency Affordable & Sustainable PHC: What’s Cookin’ in GASHA? • Focus on Chronic Disease Prevention and Management We are in the midst of crisis…..chronic disease is the cause. Our health system is not sustainable. We need a whole of community response to health, chronic disease and inequity Chronic Disease in Nova Scotia 5800 people die per year from 4 chronic diseases Cardiovascular Disease (Heart disease, stroke etc.) Cancer COPD (Chronic Obstructive Pulmonary Disorder) Diabetes Nova Scotia Context cont’d 68% of Nova Scotians 12 years of age and over have at least one chronic condition (CCHS, 2002) 70% of Health Care Costs related to Chronic Diseases (GPI Atlantic, 2002) Impact of Chronic Disease In Canada: NS highest death rate attributable to cancer Second highest rate of diabetes Chronic Disease account for 75% of all deaths in NS Medical costs alone for chronic diseases in NS account for $1.2 billion/year When combined with productivity losses they account for over $3 billion/year U.S.A. Projected toll resulting from Quality Gap Condition Shortfall in Care Avoidable Toll Diabetes 24% Blood sugar not measured 29,000 kidney failures Colorectal cancer 62% not screened 9,600 deaths Pneumonia 36% elderly did not receive vaccine 10,000 deaths Heart attack 39-55% did not receive needed medications 37,000 deaths Hypertension <65% received indicated care 68,000 deaths Healthcare Papers, Vol. 7, No. 4, 2007 Chronic Disease Prevention & Management Continuum (across the lifespan) Well Population Primary Prevention At Risk Population Secondary Prevention Established Chronic Disease Controlled Chronic Disease Tertiary Prevention Surveillance of diseases & risk factors Building healthy public policy Creating supportive environments Strengthening community actions Developing personal skills Universal & targeted approaches Population-based screening Case finding Periodic health examinations Early intervention Medication to control Universal & targeted approaches Self-management Surveillance and monitoring Creating supportive environments Health Promotion Health Promotion Prevent movement to at-risk group Draft – April 11, 2008 Treatment and acute care (exacerbation of chronic condition) Complications management Self-management Creating supportive environments Monitoring Ongoing care Maintenance Rehabilitation Self-Management Creating supportive environments Monitoring Health Promotion Health Promotion Prevent progression To established disease Prevent progression to complications and/or hospitalizations T.E.A.M. (Teaching Eating and Activity Management for Families) Chronic Disease Prevention, Screening and Management Pilot Project in Culturally Diverse and Geographically Isolated Communities Average Lipid Level 5 4.42 4.5 4.27 4.05 4 3.5 mmol/L 3 Initial 2.5 2.23 3 months 2.16 2.03 2 1.5 1.5 1.45 1.51 1.4 1.41 1.39 1 0.5 0 Triglycerides Total Cholesterol HDL LDL 6 months Initial 3 Months 6 Months Blood Pressure 131/69.5 119/66.4 118/68.8 Weight 196.1 lbs 190.1 lbs 180.7 lbs BMI 31.21 30.68 Waist Circumference 102.7 cm 99 cm 29.85 95.2 cm Body Fat 36.66 % 34.98 % 34.51 % Diabetes HbA1c 6.171 6.5 6.183 Your Way to Wellness (Chronic Disease Self-Management Program) Chronic Disease Self Management • Self-management is what people do every day: decide what to eat, whether to exercise, if and when they will take their medications. • Everyone self-manages; the question is whether or not people make decisions that improve their health-related behaviors and clinical outcomes. Patient Contact with Health Professionals GP visits per annum = 1 hour Visits to specialists = 1 hour PT, OT, Dietitian = 10 hours Total = 12 hours with professionals 364.5 days managing on their own or 8748 hours Barlow, J. Interdisciplinary Research Centre in Health, School of Health & Social Sciences, Coventry University, May 2003. Aboriginal Health Transition Fund Lindsay’s Health Centre for Women Men’s Health Centre Health Connections Collaborative Practice Teams Electronic Medical Record Well Women’s strategy Do I Need to See a Dr. Books Patient Teaching Guides (Angina, COPD, Heart Failure, Heart Attack, Diverticular disease) Health Literacy Midwifery Program Staff development (Cultural Safety, Motivational Interviewing Tips For Better Health (adapted from Donaldson, 1999) 1. Don't smoke. 2. Eat a balanced diet that includes plenty of fruit and vegetables. 3. Keep physically active. 4. Manage stress by making time to relax. 5. If you drink alcohol, do so in moderation. 6. Cover up in the sun and avoid sunburns. 7. Practise safer sex. 8. Take up cancer screening opportunities. 9. Be safe on the roads: follow the Highway Code. Tips for Staying Healthy (adapted from Dave Gordon Townsend Centre for International Poverty Research , University of Bristol) 1. Get yourself a good education. If you are illiterate, get some help. 2. Avoid being poor. If you are, try not to be poor for long. 3. Don't work in a stressful, low paid manual job. 4. Don't become unemployed. If you are, try not to stay unemployed for long. 5. Don't live in damp, low quality and crowded housing. 6. Don't live in a polluted environment. What can you do now and in the future? To improve health outcomes: Don’t just moan about things (more $$) Think outside the “health” services box (food security, literacy) Be “p”olitical (lobby, join a board) Ask “Why?” “If you always do what you have always done, you’ll always get what you always got” - PB Thank you