Physiologic Classification of Anemia Hemolytic Anemias
advertisement

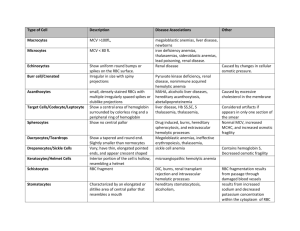
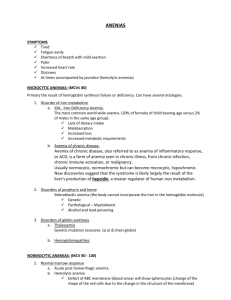
Anemia • Reduction in red cell mass or blood hemoglobin concentration, hematocrit or erythrocyte count WHO Usia 6 bulan-59 bulan 5 - <12 tahun 12 - <15 tahun Lelaki (>15 tahun) Wanita (>15 tahun) Wanita hamil Hemoglobin (g/dL) < 11 < 11,5 <12 < 13 < 12 < 11 Hematokrit (%) < 33 < 35 < 36 < 39 < 36 < 33 WHO, 2007 Classification of Anemias • Disorders of effective red cell production – disorders of erythrocyte maturation: erythroblasts die in situ before reaching the reticulocyte stage – absolute failure of erythropoiesis: absolute erythroblastopenia. • Rapid erythrocyte destruction or red cell loss Physiologic Classification of Anemia 1. Disorders of Red Cell Production a. Marrow failure i. Aplastic anemia ii. Pure red cell aplasia: Diamond-Blackfan syndrome, Transient erythroblastopenia iii. Marrow replacement: malignancy iv. Pancreatic insufficiency–marrow hypoplasia syndrome b. Impaired erythropoietin production i. Chronic renal disease ii. Hypothyroidism, hypopituitarism iii. Chronic inflammation iv. Protein malnutrition v. Hemoglobin mutants with decreased affinity for oxygen Physiologic Classification of Anemia 2. Disorders of Erythroid Maturation & Ineffective Erythropoiesis a. Abnormalities in cytoplasmic maturation i. Iron deficiency ii. Thalassemia syndromes iii. Sideroblastic anemias iv. Lead poisoning b. Abnormalities in nuclear maturation i. Vitamin B12 deficiency ii. Folic acid deficiency iii. Thiamine-responsive megaloblastic anemia iv. Hereditary abnormalities in folate metabolism v. Orotic aciduria c. Primary dyserythropoietic anemias (types I, II, III, IV) d. Erythropoietic protoporphyria e. Refractory sideroblastic anemia with vacuolization of marrow precursors and pancreatic dysfunction/deficiency Physiologic Classification of Anemia 3. Hemolytic Anemias a. Defects in hemoglobin a. Structural mutants b. Synthetic mutants (thalassemia syndromes) b. Defects in the red cell membrane c. Defects in red cell metabolism d. Antibody mediated e. Mechanical injury to the erythrocyte f. Thermal injury to the erythrocyte g. Oxidant-induced red cell injury h. Infectious agent–induced red cell injury i. Paroxysmal nocturnal hemoglobinuria j. Plasma lipid–induced abnormalities in the red cell membrane Classification of Anemias Based on Red Cell Size Microcytic Anemias • Iron deficiency • Chronic lead poisoning • Thalassemia syndromes • Sideroblastic anemias • Chronic inflammation • Some congenital hemolytic anemias with unstable hemoglobin Classification of Anemias Based on Red Cell Size Normocytic Anemias • Congenital hemolytic anemias – Hemoglobin mutants, Red cell enzyme defects, Disorders of the red cell membrane • Acquired hemolytic anemias – Antibody mediated, Microangiopathic hemolytic anemias, Secondary to acute infections • Acute blood loss • Splenic pooling • Chronic renal disease (usually) Classification of Anemias Based on Red Cell Size Macrocytic Anemias • With megaloblastic bone marrow – Vitamin B12 deficiency, Folic acid deficiency, Hereditary orotic aciduria, Thiamine-responsive anemia • Without megaloblastic bone marrow – Aplastic anemia, Diamond-Blackfan syndrome, Hypothyroidism, Liver disease, Bone marrow infiltration, Dyserythropoietic anemias Investigating anemia • Is the patient bleeding (now or in the past)? • Is there evidence for increased RBC destruction (haemolysis)? • Is the bone marrow suppressed? • Is the patient iron deficient? If so, why? • Is the patient deficient in folic acid or vitamin B12? If so, why? Investigating anemia • Detailed history and physical examination • Complete blood count: – a one-cell line (red cell line) – or part of a three-cell line abnormality (abnormality of red cell count, white blood cell count and platelet count) • Determination of the morphologic characteristics of the anemia: – blood smear – consideration of MCV and RDW – morphologic consideration of white blood cell and platelet • Reticulocyte count as a reflection of erythropoiesis • Determination if there is evidence of a hemolytic process Classification of Nature of the Anemia Based on MCV and RDW Iron-Deficiency Anemia • Clinical Manifestations – – – – – pallor glossistis Cheilitis=inflammation/fissures of lips Koilonychia Weakness and fatigue • Diagnostic Studies – CBC. Blood smear – Iron studies, reticulocyte – Endoscopy/Colonoscopy Iron-Deficiency Anemia • Treatment – Treatment of underlying disease/problem – Replacing iron • Diet • Drug Therapy – Oral iron » Absorbed best in acidic environment » GI effects » 4-6 mg/kgBW/day – Parenteral iron » IM or IV » Less desirable than PO Iron-Deficiency Anemia Management • Assess cardiovascular & respiratory status • Recognizing s/s bleeding – Monitor stool, urine and emesis for occult blood • • • • Diet teaching—foods rich in iron Supplemental iron Emphasize compliance Iron therapy for 2-3 months after the hemoglobin levels return to normal β-thalassemia DIAGNOSIS THALASSEMIA MAYOR Presentasi klinis: Pemeriksaan laboratorium: Anamnesis: Esensial: 1. 2. 3. 4. Darah tepi lengkapa o Hemoglobin o Sediaan apus darah tepi: mikrositer, hipokrom, anisositosis, poikilositosis, sel eritrosit muda (normoblast), fragmentosit, sel target. o Indeks eritrosit (MCV, MCH, MCHC, RDW) bila tidak ada cell counter, lakukan uji resistensi osmotik 1 tabung (fragilitas) Analisa hemoglobin: 1. Elektroforesis Hemoglobin o Hb varian kuantitatif (elektroforesis cellulose acetat membrane) o HbA2 kuantitatif (metoda mikrokolom) o HbF (alkali denaturasi modifikasi Betke 2 menit) o HbH inclusion bodies (pewarnaan supravital / retikulosit) Atau 2. Metoda HPLC: Analisis kualitatif dan kuantitatif Pada keadaan tertentu : • Analisis DNA (molekuler)b 5. 6. 7. 8. Pucat yang lama (kronis) Mata tampak kuning Mudah infeksi Perut membesar akibat hepatosplenomegali Pertumbuhan terhambat/pubertas terhambat. Riw. fraktur patologis Riw. keluarga menderita thalassemia Riwayat transfusi berulang) Pemeriksaan fisik 1. 2. 3. 4. 5. 6. 7. 8. Anemia/pucat Ikterus Facies Cooley Hepatosplenomegali Gizi kurang/buruk Perawakan pendek Hiperpigmentasi kulit Pubertas terlambat Diagnosis Thalassemia (-) Tetap curiga analisis DNA TIDAK curiga cari sebab lain D/: Thalassemia / (+) - Mayor - Intermediac Pengobatan Utama Usaha Pencegahan Hukum Mendel Aplastic Anemia • Pancytopenia – Decrease of all blood cell types • RBCs • White blood cells (WBCs) • Platelets – Hypocellular bone marrow • Etiology – Congenital: chromosomal alterations – Acquired • Exposure to ionizing radiation, chemical agents, viral and bacterial infections Aplastic Anemia • Clinical Manifestations – Gradual development – Symptoms caused by suppression of any or all bone marrow elements – General manifestations of anemia • Fatigue • Dyspnea • Pale skin • Frequent or prolonged infections • Unexplained or easy bruising • Nosebleed and bleeding gums • Prolonged bleeding from cuts • Dizziness • headache Aplastic Anemia • Diagnosis – Blood tests • CBC – Bone marrow biopsy Aplastic Anemia • Treatment – Identifying cause – Blood transfusions – Antibiotics – Immunosuppressants – Bone marrow transplantation Morphology 1. Spherocytes • Hereditary spherocytosis • ABO incompatibility in neonates • Immunohemolytic anemias with IgG- or C3-coated red cells • Acute oxidant injury (hexose monophosphate shunt defects during hemolytic crisis, oxidant drugs, and chemicals) • Hemolytic transfusion reactions • Clostridium welchii septicemia • Severe burns, other red cell thermal injury • Spider, bee, and snake venom • Severe hypophosphatemia • Hypersplenism 2. Target Cells • Hemoglobins S, C, D, and E • Hereditary xerocytosis • Thalassemias • (Other hypochromic-microcytic anemias) • (Obstructive liver disease) • (After splenectomy) • (Lecithin–cholesterol acyltransferase deficiency) 3. Spiculated or Crenated Red Cells • Acute hepatic necrosis (spur cell anemia) • Uremia • Red cell fragmentation syndromes • Infantile pyknocytosis • Embden-Meyerhof pathway defects • Vitamin E deficiency • Abetalipoproteinemia • Heat stroke‡ • McLeod blood group • (After splenectomy) • (Transiently after massive transfusion of stored blood) • (Anorexia nervosa) 4. Elliptocytes • Hereditary elliptocytosis • Thalassemias • (Other hypochromic-microcytic anemias) • (Megaloblastic anemias) 5. Stomatocytes • Hereditary stomatocytosis • Rhnull blood group • Stomatocytosis with cold hemolysis • (Liver disease, especially acute alcoholism) • (Mediterranean stomatocytosis) • Diagrammatic representation of different types of poikilocyte Normocyte