preoperative amiodarone as prophylaxis against atrial
advertisement

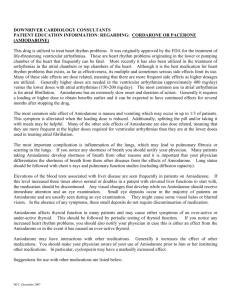
PREOPERATIVE AMIODARONE AS PROPHYLAXIS AGAINST ATRIAL FIBRILLATION AFTER CARDIAC VALVE SURGERY AMONG RHEUMATIC HEART DISEASE PATIENTS: A Meta-analysis Ian Lusoc, MD Flordeliz Lontok, MD The Heart Institute, St. Luke’s Medical Center Quezon City Introduction • Atrial fibrillation (AF) is common among patients with valvular heart disease and is a frequent rhythm disorder after cardiac surgery1 • It occurs in up to 60% of patients who undergo any cardiac surgery and those who undergo valve procedure2,3,4 1. Maesen B, Nijs J, Maessen J, Allesie M, Schotten U. Post-operative atrial fibrillation: a maze of mechanisms. Europace 2012;14:159-74. 2. Maisel WH, Rawn JD, Stevenson WG. Atrial fibrillation after cardiac surgery. Ann Intern Med 2001;135:1061-73. 3. Mitchell LB, et al. Prophylactic oral amiodarone for the prevention of arrhythmias that begin early after revascularization, valve replacement, or repair. PAPABEAR: A randomized controlled trial. JAMA 2005; 294:3093-3100. 4. Daoud EG, Strickberger SA, Man KC, Goyal R, Deeb M, Bolling S, Pagani F, Bitar C, Meissner M, Morady F. Preoperative amiodarone as prophylaxis against atrial fibrillation after heart surgery. N Engl J Med 1997; 337: 1786-91. Introduction In developing countries like the Philippines, valvular heart disease of rheumatic origin is the most frequent etiology of this disorder1 Once present, it poses risks such as hemodynamic instability, thromboembolism, necessity for anticoagulation, and prolonged hospital stay. 1. ABC of Atrial Fibrillation: History, Epidemiology, and Importance of Atrial Fibrillation. Gregory Y H Lip, et al. BMJ 1995;1311:1361. STUDY Wyse, 2002 (AFFIRM) TITLE A Comparison of Rate Control and Rhythm Control in Patients with AF POPULATION / INTERVENTION Patients with nonrheumatic AF were given either antiarrhythmic drug or drug for rate control OUTCOME Rhythm-control strategy offers no survival advantage over the ratecontrol strategy in AF STUDY TITLE POPULATION / INTERVENTION OUTCOME Wyse, 2002 (AFFIRM) A Comparison of Rate Control and Rhythm Control in Patients with AF Patients with nonrheumatic AF were given either antiarrhythmic drug or drug for rate control Rhythm-control strategy offers no survival advantage over the ratecontrol strategy in AF Raine, 2004 Effect of Mitral Valve Repair/Replacement Surgery on Atrial Arrhythmia Behavior Mitral valve surgery Mitral valve surgery in patients with alone restored chronic AF sinus rhythm in only 8.5% STUDY TITLE POPULATION / INTERVENTION OUTCOME Wyse, 2002 (AFFIRM) A Comparison of Rate Control and Rhythm Control in Patients with AF Patients with nonrheumatic AF were given either antiarrhythmic drug or drug for rate control Rhythm-control strategy offers no survival advantage over the ratecontrol strategy in AF Raine, 2004 Effect of Mitral Valve Repair/Replacement Surgery on Atrial Arrhythmia Behavior Mitral valve surgery Mitral valve surgery in patients with alone restored chronic AF sinus rhythm in only 8.5% Vora, 2004 Control of Rate vs Rhythm in Rheumatic AF Oral amiodarone ( DC cardioversion) given to RHD patients undergoing mitral valve surgery Maintenance of sinus rhythm superior to ventricular rate control in patients with rheumatic atrial fibrillation Introduction Role of IV amiodarone in restoring sinus rhythm after valve surgery in RHD patients with or without chronic AF. Research Question • Among rheumatic heart disease patients undergoing cardiac valve surgery, how effective is IV amiodarone in reducing the incidence of post-operative atrial fibrillation? Objectives 1. To determine the efficacy of IV amiodarone in comparison with placebo in reducing the incidence of post-operative AF 2. To determine the safety of amiodarone in terms of occurrence of adverse events. Inclusion Criteria • Randomized controlled trials comparing IV amiodarone vs. placebo among patients with RHD in preventing the occurrence of AF, and/or converting AF to NSR after a cardiac valve surgery. Trial Selection Potentially eligible reports identified and retrieved (n = 339) Reports included (n = 2) Trials of amiodarone vs placebo in RHD patients undergoing cardiac valve surgery Reports excluded (n = 337) Observational studies Case reports Animal studies Reviews Not amiodarone as intervention Not amiodarone vs placebo Not cardiac surgery Not cardiac valve surgery Not RHD patients Not AF Study Design Characteristics Selvaraj,1 2009 Kar,2 2011 RCT RCT 82 56 Amiodarone 42 28 Control (placebo) 40 28 Trial design Sample size, total Type of Surgery MVR or AVR, or both MVR or AVR, or both Timing of amiodarone Perioperative (after administration anesthesia induction, before CPB) Perioperative (after anesthesia induction, before CPB) Total dose of amiodarone 3 mg/kg IV infusion over 20 min 3 mg/kg IV infusion over 30 min 1. Selvaraj T, Kiran U, Das S, Chauhan S, Sahu B, Gharde P. Effect of single intraoperative dose of amiodarone in patients with rheumatic valvular heart disease and atrial fibrillation undergoing valve replacement surgery. Ann Card Anaesthesia 2009;12:10-6. 2. Kar SK, Dasgupta CS, Goswami A. Effect of prophylactic amiodarone in patients with rheumatic valve disease undergoing valve replacement surgery. Ann Card Anaesthesia 2011;14:176-82 Study Design Characteristics Selvaraj, 2009 Kar, 2011 Arrhythmia AF AF Period when AF was observed to occur At aortic cross-clamp release, at end of surgery, within 24 hours post-operatively, and before hospital discharge At aortic cross-clamp release, at end of surgery, and within 24 hours post-operatively RESULTS Baseline Characteristics Age, years SD Male:female Body weight (kg) Height (cm) Number of patients in AF (preinduction) NYHA class Class II Class III Severity of mitral stenosis Mild Moderate Severe Severity of mitral regurgitation Mild Moderate Severe Selvaraj et al, 2009 Amiodarone Placebo (n = 42) (n = 40) 33.48 ± 14.11 35.55 ± 11.65 23:19 17:23 52.24 ± 13.78 55.45 ± 13.76 160.76 ± 8.85 163.13 ± 7.73 42 40 Kar et al, 2011 Amiodarone Placebo (n = 28) (n = 28) 36 ± 89 35.25 ± 8.4 16:12 14:14 51 ± 11.35 50.53 ± 6.77 12 12 21 21 19 21 28 0 28 0 6 11 22 4 9 27 4 3 0 3 1 0 7 18 14 8 15 17 5 22 0 0 27 0 Baseline Characteristics Selvaraj et al, 2009 Kar et al, 2011 Amiodarone (n = 42) Placebo (n = 40) Amiodarone (n = 28) Placebo (n = 28) Normal 33 29 13 12 Mild dysfunction 9 11 15 16 Severe dysfunction 0 0 0 0 Digoxin 42 40 Betablocker 14 15 Calcium channel blocker 5 5 MVR 35 35 26 24 AVR 3 0 0 0 DVR 4 5 2 4 49.14 ± 11.29 47.98 ± 8.7 < 45 14 12 0 13 45 – 59 21 25 28 15 ≥ 60 7 3 0 0 LV function Type of heart surgery Pre-op LA size (mm) LA size (mm) Incidence of AF After Aortic Cross-clamping Experimental Study or Subgroup Events Control Risk Ratio Risk Ratio Total Events Total Weight M-H, Fixed, 95% CI Kar, 2011 2 28 8 28 34.2% 0.25 [0.06, 1.07] Selvaraj, 2009 6 42 15 40 65.8% 0.38 [0.16, 0.88] 68 100.0% 0.34 [0.16, 0.70] Total (95% CI) Total events 70 8 23 Heterogeneity: Chi² = 0.24, df = 1 (P = 0.62); I² = 0% Test for overall effect: Z = 2.93 (P = 0.003) M-H, Fixed, 95% CI 0.01 0.1 1 10 100 Favours Amiodarone Favours Placebo Incidence of AF At the End of Surgery Experimental Study or Subgroup Events Control Risk Ratio Risk Ratio Total Events Total Weight M-H, Fixed, 95% CI Kar, 2011 0 28 4 28 25.3% 0.11 [0.01, 1.97] Selvaraj, 2009 4 42 13 40 74.7% 0.29 [0.10, 0.82] 68 100.0% 0.25 [0.09, 0.65] Total (95% CI) Total events 70 4 17 Heterogeneity: Chi² = 0.40, df = 1 (P = 0.53); I² = 0% Test for overall effect: Z = 2.82 (P = 0.005) M-H, Fixed, 95% CI 0.01 0.1 1 10 100 Favours Amiodarone Favours Placebo Incidence of AF Post-op in ICU within 24 hours Experimental Study or Subgroup Control Risk Ratio Risk Ratio Events Total Events Total Weight M-H, Fixed, 95% CI Kar, 2011 4 28 7 28 39.7% 0.57 [0.19, 1.74] Selvaraj, 2009 5 39 9 27 60.3% 0.38 [0.14, 1.02] 55 100.0% 0.46 [0.22, 0.95] Total (95% CI) Total events 67 9 16 Heterogeneity: Chi² = 0.28, df = 1 (P = 0.60); I² = 0% Test for overall effect: Z = 2.09 (P = 0.04) M-H, Fixed, 95% CI 0.01 0.1 1 10 100 Favours Amiodarone Favours Placebo Incidence of AF First Post-op Day Experimental Study or Subgroup Control Risk Ratio Risk Ratio Events Total Events Total Weight M-H, Fixed, 95% CI Kar, 2011 6 28 15 28 40.0% 0.40 [0.18, 0.88] Selvaraj, 2009 9 42 22 40 60.0% 0.39 [0.20, 0.74] 68 100.0% 0.39 [0.24, 0.65] Total (95% CI) Total events 70 15 37 Heterogeneity: Chi² = 0.00, df = 1 (P = 0.96); I² = 0% Test for overall effect: Z = 3.66 (P = 0.0002) M-H, Fixed, 95% CI 0.01 0.1 1 10 100 Favours Amiodarone Favours Placebo Adverse Events Hypotension Experimental Study or Subgroup Control Risk Ratio Risk Ratio Events Total Events Total Weight M-H, Fixed, 95% CI Kar, 2011 1 28 1 28 9.8% 1.00 [0.07, 15.21] Selvaraj, 2009 5 42 9 40 90.2% 0.53 [0.19, 1.44] 68 100.0% 0.58 [0.23, 1.47] Total (95% CI) Total events 70 6 10 Heterogeneity: Chi² = 0.19, df = 1 (P = 0.67); I² = 0% Test for overall effect: Z = 1.16 (P = 0.25) M-H, Fixed, 95% CI 0.01 0.1 1 10 100 Favours Amiodarone Favours Placebo Adverse Events Bradycardia Experimental Study or Subgroup Kar, 2011 Selvaraj, 2009 Risk Ratio Risk Ratio Events Total Events Total Weight M-H, Fixed, 95% CI 1 28 1 28 14.0% 1.00 [0.07, 15.21] 16 42 6 40 86.0% 2.54 [1.10, 5.84] 68 100.0% 2.32 [1.06, 5.12] Total (95% CI) Total events Control 70 17 7 Heterogeneity: Chi² = 0.41, df = 1 (P = 0.52); I² = 0% Test for overall effect: Z = 2.10 (P = 0.04) M-H, Fixed, 95% CI 0.01 0.1 1 10 100 Favours Amiodarone Favours Placebo Conclusion • Among RHD patients with or without chronic AF undergoing cardiac valve surgery, IV amiodarone appears to decrease the incidence of atrial fibrillation after surgery • The incidence of adverse event (bradycardia) appears to be higher in the amiodarone group. Limitation • Small population size • It is not clear whether an anti-arrhythmic surgery was done to the study population which can significantly influence outcome • Recurrence of AF during entire hospitalization and beyond was not investigated. Recommendation • Larger RCTs with similar protocols • Follow up cardiac rhythm of patients after hospital discharge. THANK YOU Validity CRITERIA Randomization Allocation Concealment Selvaraj 2009 Yes Yes Kar 2011 Yes Yes Baseline Characteristics Yes Yes Blinding of Patients Yes Yes Blinding of Caregivers Yes Yes Blinding of Assessors Yes Yes Intention to treat Adequacy of Follow-up Yes Yes Yes Yes References 1. Maesen B, Nijs J, Maessen J, Allesie M, Schotten U. Post-operative atrial fibrillation: a maze of mechanisms. Europace 2012;14:15974. 2. ABC of Atrial Fibrillation: History, Epidemiology, and Importance of Atrial Fibrillation. Gregory Y H Lip, et al. BMJ 1995;1311:1361. 3. Raine D, Dark J, Bourke JP. Effect of mitral valve repair/replacement surgery on atrial arrhythmia behavior. J Heart Valve Dis 2004; 13:615-21. 4. Maisel WH, Rawn JD, Stevenson WG. Atrial fibrillation after cardiac surgery. Ann Intern Med 2001;135:1061-73. 5. Mitchell LB, et al. Prophylactic oral amiodarone for the prevention of arrhythmias that begin early after revascularization, valve replacement, or repair. PAPABEAR: A randomized controlled trial. JAMA 2005; 294:3093-3100. 6. Daoud EG, Strickberger SA, Man KC, Goyal R, Deeb M, Bolling S, Pagani F, Bitar C, Meissner M, Morady F. Preoperative amiodarone as prophylaxis against atrial fibrillation after heart surgery. N Engl J Med 1997; 337: 1786-91. 7. Bealieu Y, Denault AY, Couture P, et al. Perioperative IV amiodarone does not reduce the burden of AF in patients undergoing cardiac valvular surgery. Anesthesiology 2010; 112:128-37. 8. Aasbo JD, et al. Amiodarone prophylaxis reduces major cardiovascular morbidity and length of stay after cardiac surgery: A metaanalysis. Ann Intern Med 2005; 143:327-336. 9. Wyse DG, Waldo AL, DiMarco JP, Domanski MJ, Rosenberg Y, Schron EB, et al. Atrial fibrillation follow-up investigation of rhythm management (AFFIRM) investigators: a comparison of rate control and rhythm control in patients with atrial fibrillation. N Engl J Med 2002; 1825-33. 10. Vora A, Kamad D, Goyal V, Naik A, Gupta A, Lokhandwala Y, Kulkami H, Singh B.Control of rate versus rhythm in rheumatic atrial fibrillation: a randomized study.Indian Heart J. 2004 Mar-Apr;56(2):110-6. 11. Selvaraj T, Kiran U, Das S, Chauhan S, Sahu B, Gharde P. Effect of single intraoperative dose of amiodarone in patients with rheumatic valvular heart disease and atrial fibrillation undergoing valve replacement surgery. Ann Card Anaesthesia 2009;12:10-6. 12. Kar SK, Dasgupta CS, Goswami A. Effect of prophylactic amiodarone in patients with rheumatic valve disease undergoing valve replacement surgery. Ann Card Anaesthesia 2011;14:176-82 13. Raanani E, Albage A, David TE, Yau TM, Armstrong S. The efficacy of the Cox/maze procedure combined with mitral valve surgery: A matched control study. Eur J Cardiothorac Surg 2001;19:438-443. AFFIRM Trial Wyse DG, Waldo AL, DiMarco JP, Domanski MJ, Rosenberg Y, Schron EB, et al. Atrial fibrillation follow-up investigation of rhythm management (AFFIRM) investigators: a comparison of rate control and rhythm control in patients with atrial fibrillation. N Engl J Med 2002; 1825-33. Raine D, Dark J, Bourke JP. Effect of mitral valve repair/replacement surgery on atrial arrhythmia behavior. J Heart Valve Dis 2004; 13:615-21. Vora A, Kamad D, Goyal V, Naik A, Gupta A, Lokhandwala Y, Kulkami H, Singh B.Control of rate versus rhythm in rheumatic atrial fibrillation: a randomized study.Indian Heart J. 2004 Mar-Apr;56(2):110-6.