Duration of CPR and Illness Category
Impact Survival and Neurologic
Outcomes for In-hospital Paediatric
Cardiac Arrests
Journal Club
Kavi Aucharaz
25.09.2014
Case presentation
• A 9 yr old boy admitted in the ward with fever
and possible Macrophage Activation
Syndrome.
• Sudden deterioration and cardiac arrest.
• CPR was performed >20 mins-unsuccessful
• Was this futile? How long should we perform
CPR In-hospital cardiac arrest?
• What is the relationship between duration
CPR duration and its effect on neurological
outcome?
Background
Paediatric CPR >20mins have been considered
futile after paediatric in-hospital cardiac arrests.
Concept recently been questioned, although the
effect of CPR duration on outcomes has not
recently been described.
Objective - to determine the relationship
between CPR duration and outcomes after
paediatric in-hospital cardiac arrests.
GWTG-R
The American Heart Association’s Get With The
Guidelines–Resuscitation (GWTG-R) the only national
registry of in-hospital resuscitation events.
The objectives of study were to use the GWTG-R data
to evaluate.
◦ The relationship between CPR duration and intact survival to
hospital.
◦ Discharge after paediatric IHCA according to patient illness
category.
Methods
• AHA GWTG-R is a prospective, multi-centre registry of
IHCA and resuscitation events using Utstein-style data
reporting.
• Analysis included data from 328 US and Canadian
hospitals.
• Between 1 Jan. 2000- 31Dec. 2009.
• Study was approved by the Institutional Review BoardUniversity of Pittsburgh.
Data Collection
• Index events defined as the patient’s first
cardiopulmonary arrest event during the hospitalization.
• Predefined patient illness categories based on patient
characteristics at the time of cardiopulmonary arrest.
• General medical patients had a primary diagnosis of
medical illness that was not cardiovascular.
Data collection
• Medical cardiac patients had a primary
diagnosis of medical illness that was
cardiovascular.
• General surgical patients were preoperative with
a general surgical illness or postoperative after
non cardiac surgery.
• Surgical cardiac patients were postoperative
after cardiac surgery.
• Trauma patients had single or multiple injuries.
Inclusion and Exclusion Criteria
• Included all index pulseless IHCA events
occurring in patients<18 years of age for which
at least 1 min. of chest compressions was
provided.
• Excluded patients in whom the event began out
of the hospital or in the NICU, delivery room, or
nursery.
• Also excluded patients with illness categories of
new-born, obstetric, or other illnesses.
Exclusion
• For patients who were documented as receiving >180
minutes of chest compressions, the CPR duration
variable was winsorized at a predefined maximum of 180
minutes to reduce the effects of possibly spurious
outliers.
Outcome Measures
• Primary outcome measure was survival to
hospital discharge.
• Secondary survival measures included return of
spontaneous circulation >20 minutes.
– 24-hour survival,
– Survival to discharge with favourable neurological
outcome.
• Neurological outcome was determined with the
use of Paediatric Cerebral Performance
Category (PCPC) scales, which were assigned
after a review of medical records.
Outcome measures
• Favourable neurological outcome was
prospectively defined in 2 ways:
– a PCPC score of 1, 2, or 3 on hospital discharge.
– or discharge PCPC no worse than on admission.
• Analysis was repeated excluding a PCPC score
of 3 as a favourable neurological outcome.
Statistics
• Conducted analyses using SAS 9.0 (SAS Inc,
Cary, NC) and Stata 12.1 (Stata Corp, College
Station, TX).
• Chest compression duration was analyzed as
both a continuous variable and a categorical
variable.
• Categories of CPR duration were determined
with cut points used in previous studies.
Statistics
• Studied CPR duration categories of 1-15, 16-35, and
>35 minutes.
• χ2 or Fisher exact test for categorical variables was
used.
• Wilcoxon Rank-sum test, Kruskal-Wallis test, or ANOVA
for continuous variables.
Results
3419 paediatric IHCAs in 328 hospitals that fulfilled
inclusion and exclusion criteria.
56% occurred in hospitals with ≥80 paediatric beds
86% occurred in hospitals with at least 20 pediatric
beds.
Total = (30% In hospitals 20-80 beds, 14% less than
20 beds, 56% over 80 beds) )
The mean ±SD age of the study sample was
4.9±6.0 years.
Almost all events were witnessed (92.0%) and
monitored (90.5%; Table 1). Witnessed or monitored
3286 (96.1)
Results
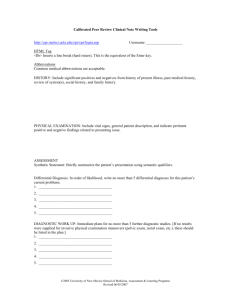
• ROSC for >20 minutes occurred in 2178 patients
(64%).
• 1373(40%) were still alive at 24 hours after the
event.
• 954 (27.9%)survived to hospital discharge.
• 651 (19.0%) had a favourable neurological
outcome
• Favourable outcome (651/954)68.2% of hospital
survivors).
Utstein diagram.
Matos R I et al. Circulation. 2013;127:442-451
Copyright © American Heart Association, Inc. All rights reserved.
Results
• Respiratory insufficiency (59.1%) and hypotension
(39.9%) were the most common comorbidities.
• Among medical and surgical cardiac patients,
arrhythmias were present in 29.6%
Results
•
•
•
•
•
2/3 of arrests occurred in the ICU.
14.4% in the ED.
10.0% on the inpatient ward,
6.2% in an operative or recovery area
Hypotension, arrhythmias, and acute respiratory
insufficiency were the most common immediate
precipitating causes of the arrests.
ECMO & CPR in cardiac surgical
patients
• Compared with other patients, trauma patients
were more likely to be older and their arrests were
more likely to occur in ED.
• Surgical cardiac patients were placed on ECMO
more than any other group-- no change in survival
with ECMO and CPR duration.
• There was a statistical significant survival benefit
for surgical cardiac patients who received>35
mins CPR and ECMO(38.5% with ECMO and
16.7% without ECMO; P<0.0001)
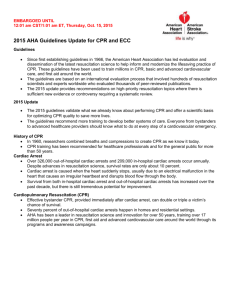
Adjusted probability of outcomes at hospital discharge by cardiopulmonary
resuscitation (CPR) duration stratified by patient illness category (adjusted for
initial pulseless rhythm, age category, weekend, night, extracorporeal
membrane oxygenation, calcium administration, sepsis, renal insufficiency,
vasoactive infusion during arrest, event location, sodium bicarbonate
administration, prior history of a cardiopulmonary arrest, prearrest apnea
monitor, prearrest pulse oximeter, and patient hypotension before arrest).
•
In the general medical patients the OR was 1 for survival to
discharge and neurological outcome
• P- IHCA Patients <18 of age for
which at least 1 min of chest
compressions were provided
• Risk factors- 5 patient illness
categories: surgical cardiac,
medical cardiac, general medical,
general surgical and trauma.
• O- primary outcome: Survival to
hospital discharge
• Secondary outcome:
ROSC>20min, 24hr survival,
survival to discharge with
favourable neurological outcome
•
Multicentre registry of IHCA and
resuscitation events using Utstein-style
data reporting.
•
GWTG-R centres accounts 10% of all
hospitals in US These volunteer centres
pay a fee(More resources) as well as
greater interest in CPR –may vary from
other US hospitals. However may not
affect the relative proportions.
•
Pre defined patient illness categories based on patients characteristics at the
time of cardiopulmonary arrest.
•
There was well defined inclusion and
exclusion criteria.
•
Objective measures of the
duration of CPR was studied in
the different categories.
•
Chest compressions duration
was analysed as both continuous
variable and categorical variable
•
Statistical test were used to
minimise bias and cofounding
variables were looked at.
•
The cohort used had all been
subject to the defined categories
of exposure i.e intervention
•
Objective primary and secondary
outcome measures were looked at.(
ROSC>20min, 24 hr survival and
survival to discharge with favourable
neurological outcome)
•
Neurological outcome-paediactric
cerebral performance category
scales(PCPC)—validated tool used
•
Well defined inclusion and exclusion
criteria.
•
Same tool was used to look at in the
different categories-using PCPC
•
This was a prospective multi-centred
registry of IHPCAs—can’t be blinded
•
•
•
Who led the resuscitation in the
different hospitals?
The disease severity pre-arrest would
have been helpful in analysis.
1551/3419(45%) of the patients were
combined(Gen. Surgery, Surg.cardiac,
medical cardiac)not true presentation
of general paediatrics
•
•
•
•
•
•
•
Event time of the day
Event day of the week
ECMO
Calcium bolus during
arrest
underlying sepsis
Vasoactive infusion
(Multivariable logistic
regression models were
fit)
•
Favourable neurological outcome was
prospectively defined based on the PCPC score
or no worse than on admission
• PCPC was used as a global
measure of neurological
function.
• There was lack of long term
neurological follow up.
•
However there are studies which
have looked into the neurological
outcome at 6 months and 12 mo
which have shown not substantially
different status from discharge.
•
In first 15 mins CPR the survival rate fell linearly,
decreasing by 2.1% per min of chest
compressions(R2 =0.9992)
•
Survival rate continues to decrease with
increasing CPR
•
The probability of favourable neurological
outcome fell linearly in the 1st 15 mins of
CPR(R2 =0.9972).
•
Trauma patients had the poorest outcome after
any amount of CPR
•
Outcome are best with shorter duration of CPR
and that many children survive after prolonged
CPR(>35 mins).
• Compared to general medical patients, surgical cardiac patients had
best survival (OR, 2.5; 95% CI 1.8-3.4), followed by general surgical
and medical cardiac patients(P<0.0001).
• Compared with general medical patients, surgical cardiac patients
had the highest odds of achieving a favourable neurological
outcome(OR, 2.7; 95% CI 2.0-3.9; P<0.01)
• Trauma patients have decreased odds of favourable neurological
outcome compared with gen. medical group(OR, 0.2; 95% CI, 0.10.4;P<0.001)
•
•
•
•
•
•
The cohort had 45% patients with
Med/surgical cardiac and general
surgical patients.
•
Although a prospective
observational study it was well
designed.
There were good inclusion
and exclusion criteria.
Confounding factors were
taken into account.
The results were not
generalizable-newborns were
excluded who were in
NICU,(Gen. surgical and
surgical cardiac).
The practice in the different
hospitals may have been
different and this can affect
the results
Few inconsistent data in the
paper and the supplemental
tables
•
•
•
•
Prolonged resuscitation cannot be
generalised, the pre-arrest condition and
diagnosis is an important factor to be
considered
•
The study highlights in certain
illness categories such as
surgical cardiac patients have
favourable probabilities of
good neurological survival
after longer durations of CPR.
In our setting we will have less
surgical cardiac patients.
We may consider longer
duration of CPR in cardiac
medical patients .
In multiple trauma cases it
would be futile to continue
prolonged CPR due to poor
outcome.
•
Reis AG, Nadkarni V, Perondi MB, Grisi S, Berg RA. A prospective
inves-tigation into the epidemiology of in-hospital pediatric
cardiopulmonary resuscitation using the international Utstein
reporting style. Pediatrics. 2002;109:200–209.
• Samson RA, Nadkarni VM, Meaney PA, Carey SM, Berg MD, Berg
RA; American Heart Association National Registry of CPR
Investigators. Out-comes of in-hospital ventricular fibrillation in
children. N Engl J Med. 2006;354:2328–2339.
• Survey of outcome of CPR in pediatric in-hospital cardiac arrest in a
medical center in Taiwan.Citation:Resuscitation, 04 2009, vol./is.
80/4(443-8), 0300-9572;0300-9572 (2009 Apr)
• Author(s):Wu ET,Li MJ,Huang SC,Wang CC,Liu YP,Lu FL,Ko
WJ,Wang MJ,Wang JK,Wu MH
• The survival outcomes are similar to recent paediatric IHCA. Other
studies have also reported favourable neurological survival 14-22%.
•
•
•
Proportion of children who
would presumable die
without CPR survive with a
favourable neurological
outcome even after
prolonged CPR
Raise awareness that
some categories of children
eg Cardiac surgical and
general surgical patients do
better after prolonged CPR
Trauma patients have the
poorest outcome with any
period of CPR.