rehabilitation in paraplegia
advertisement

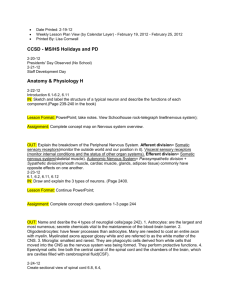
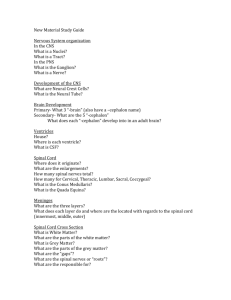
A PROJECT Entitled “REHABILITATION IN PARAPLEGIA” Submitted To The Department Of Physiotherapy I.T.S PARAMEDICAL COLLEGE Affiliated To CHAUDHARY CHARAN SINGH UNIVERSITY, MERRUT In The Partial Fulfillment of Degree Of BACHELOR OF PHYSIOTHERAPY Guide Dr Shubhra Narang Submitted By Vishakha puri March 2010 CERTIFICATE This is to certify that the project work entitled “REHABILITATION IN PARAPLEGIA” by VISHAKHA PURI BPT 2006-2010 Batch , Enroll No._____________has been completed in the partial fulfillment for the degree of Bachelor of Physiotherapy from C.C.S. University, Meerut, U.P., India. I recommend him/her for the award of BPT Degree. DR.C.S.RAM DIRECTOR DEPT. OF PHYSIOTHERAPY I.T.S PARAMEDICAL COLLEGE CERTIFICATE This is to certify that the project work entitled “REHABILITATION IN PARAPLEGIA” is conducted by VISHAKHA PURI in the partial fulfillment for the degree of Bachelor of Physiotherapy under my guidance and supervision . GUIDE Dr SHUBHRA NARANG MPT NEUROLOGY (i) CERTIFICATE OF ORIGINALITY I hereby declare that the project work entitled “REHABILITATION IN PARAPLEGIA ” embodies the original work by me . This work in part or full has not been submitted to any other university for award of degree. I shall not publish the contents of this project in part or full without the written consent of my guide and college. VISHAKHA PURI B.P.T 2006-2010 Batch Enroll. No. ________ (ii) ACKNOWLEDGEMENT I would like to express my sincerest gratitude to the following individuals without whom this study would have been unattainable. I offer my sincerest gratitude to Dr. Shubhra Narang (M.P.T) whose guidance constructive concel , unmatchable suggestions and unstinted encouragement enlightened me throughout the project. I express my heartiest gratitude to Dr. C.S. Ram , H.O.D , Department Of Physiotherapy , I.T.S Paramedical college for kindly permitting us to pursue research work. I am thankful to Dr. M Thangaraj , Dr. Stuti Sehgal , Dr. Tanu Shrivastava , Dr. Kanika Govil , Dr. Ekta for their constant inspiration and support in pursuing the study . I would like to thank my colleagues Ashish gautam , Pooja sinha , Priyenka tyagi and Yukti sharma for their co-operation in my project . Remarkable co-operation and dedication by the subjects laid milestone for the success of project completion. And finally thanks to all those who have contributed directly and indirectly towards this study. VISHAKHA PURI (iii) DEDICATED TO MY PARENTS AND ALL MY FACULTY (iv) TABLE OF CONTENTS Certificate ( Guide) i Certificate Of Originality ii Acknowledgement iii Dedication iv List of figures v-vi List of Tables vii 1) INTRODUCTION Anatomy – The basis of injury classification Epidemiology Mechanism of injury Designation of lesion level 2) TYPES OF LESIONS IN SPINAL CORD Complete injury Incomplete injury a) Central cord syndrome b) Anterior cord syndrome c) Brown sequard syndrome d) Posterior cord syndrome e) Cauda equine syndrome f ) Sacral sparing Stages after spinal cord injury a) Stage of spinal shock b) Stage of reflex activity c) Stage of reflex failure 3) CLINICAL MANIFESTATIONS Direct Impairments a) Autonomic dysreflexia b) Impaired temperature regulation c) Orthostatic hypotension d) Bladder dysfunction e) Bowel dysfunction Indirect impairments a) Pressure sores b) Deep venous thrombosis c) Contractures d) Heterotopic ossification e) Pain 4) HOSPITAL MANAGEMENT Prehospital management Immediate management of patient with spinal cord injury a) transfer from the site of emergency b) assessment of ABCDE c) neurological status examination d) skin inspection e) temperature examination f) bladder function Investigations Fracture stabilization Pharmacological management 5) REHABILITATIVE MANAGEMENT Acute phase rehabiltation Active phase rehabilitation Transition phase of rehabilitation ( 6 ) BIBLIOGRAPHY (7 ) APPENDICES Appendix A Appendix B Appendix C Appendix D LIST OF FIGURES Figure 1) Figure 2) : : Etiology of spinal cord injury Types of thoracolumbar fractures Figure 3) : Central cord syndrome Figure 4) : Anterior cord syndrome Figure 5) : Brown sequard syndrome Figure 6) : Cauda equine syndrome Figure 7) : Stage of spinal shock Figure 8) : Autonomic dysreflexia Figure 9) : Pressure sore Figure10) : Deep venous thrombosis Figure11) : Heterotopic ossification (a) Hip (b) Knee Figure12) : Harrington rod Figure13) : Jewett brace Figure14) : Phenol peripheral nerve block Figure15) : Negative pressure vacuum technique Figure 16) : Elastic support stockings Figure 17) : Tilt table Figure 18) : Rolling Figure 19) : Supine to long sitting position Figure 20) : Prone on elbow position Figure21) : Prone on hand position Figure22) : Quadruped position Figure23) : Kneeling position (v) Figure24) : Push up weight shift Figure25) : Bed to wheelchair transfer Figure26) : Wheelchair to bed transfer Figure27) : Wheelchair to car transfer Figure28) : Car to wheelchair transfer Figure29) : Wheelchair to toilet transfer Figure30) : Toilet to wheelchair transfer Figure 31) : Wheelchair to bath seat transfer Figure 32) : Bathseat to wheelchair transfer Figure 33 ) : Oswestry standing frame Figure34) : Orthosis prescribed in case of paraplegics a) Knee ankle foot orthosis b) Scott craig orthosis Figure35) : Standing from wheelchair with crutches a) Forward technique b) Sideway technique c) Backward technique Figure 36) : Crutch balancing Figure 37) : Ambulation activities with crutches a) Swing to gait b) Swing through gait c) Four point gait Figure38) : Partial body weight support treadmill Figure39) : Functional electrical stimulation (vi) LIST OF TABLES Table 1 : Etiology Table 2 : Mechanism of injury Table 3 : Pharmacological management of spasticity Table 4 : Pharmacological management of pain Table 5 : Correlation of complete injury levels and orthosis prescription ABBREVIATIONS USED LMN - Lower motor neuron UMN - Upper motor neuron SCI - Spinal cord injury DVT - Deep vein thrombosis PaO2 - Partial pressure of oxygen BP - Blood pressure CT Scan-Computed tomographic scan MRI - Magnetic resonance imaging IM - Intramuscularly IV - Intravenously TENS - Transcutaneous electrical nerve stimulation KAFO - Knee ankle foot orthosis RGO - Reciprocal gait orthosis AFO - Ankle foot orthosis FES - Functional electrical stimulation Ft - Feet # - Fracture N - Normal I - Intact PT - Performance time Rep - Repetitions Sec - Seconds H - Hold Res - Resistance (vii) CHAPTER 1 INTRODUCTION ( SIMILARLY FOR OTHER CHAPTERS) Spinal cord injury is a central neurological disorder1 . It occurs due to damage to neurological components in spinal cord occurring as a result of primary or secondary effects of disease or trauma 2. Spinal cord injury is a low incidence , high cost disability requiring tremendous changes in an individuals life style3 . Normal events of life driving a car, diving into lake or walking down stairs can suddenly results in life changing injury with physical and lifestyle constraints that totally refigure the realities of daily life . SPINAL CORD INJURY ANATOMY – THE BASIS OF INJURY CLASSIFICATION The term spinal column refers to the vertebral column bones and disc that collectively encases and protects the soft tissue of the spinal cord .The spinal cord is made up of nerve tracts carrying signal back and forth between the brain and rest of the body4 . Etiology of SCI 60 Percentage of SCI 50 40 On /before 1980 30 Since 2000 20 10 0 Rta Falls Violence Cause Sports Others Figure 1: Incidence of spinal cord injury (2) ETIOLOGY10 Trauma Road traffic accident , Gun shot wounds. Non traumatic factors Meningioma , astrocytoma , metastatic Tumours Ischaemia Developmental disorders Neurodegenerative disease Transverse myelities tumour in spinal cord Arteriosclerosis , dissecting aortic aneurysms Spina bifida , meningomyelocele Friedreich's ataxia , spinocerebellar ataxia, Resulting from stroke or inflammation. Vascular Malformation Arteriovenous arteriovenous malformation fistula , , dural spinal hemangioma , cavernous angioma and aneurysm. Tabl e1: Etiol Demyelinating disease Multiple sclerosis ogy of spinal cord injury (3) (5) Figure 2 : Thoracolumbar fractures END OF CHAPTERS BIBLIOGRAPHY Books Referred 1. Susan B O’ Sullivan , Thomas J Schmitz : Physical Rehabilitation and Assessment and Treatment (Fifthedition) : chapter 23 : Traumatic spinal cord injury : page 932-9 2. Cameron Monroe : Physical rehabilitation : chapter 20 : Non progressive spinal cord disorders : page 539-573 3. Ida Bromley : Tetraplegia and Paraplegia (fourth edition) : chapter 10-12 : Mat work , wheelchair and wheelchair management , transfers : page 95 – 115. 4. Tidy`s Physiotherapy, Twelfth edition , Ann Thompson , Alison Skinner , JoanPrierly : chapter 7 : 229243 5. Darcy. A. Umphred : Neurological Rehabilitation : Fourth Edition :Chapter 16 : Page 477530. 6. Louis Solemom , Davi J. Warwick Silva Durai Nayagam : Apley`s System of orthopaedics and fractures : The spine : page 1130-1135 7. Lorriane William Pedretti : Occupation Therapy Practice skills for physical Dysfunction 4 th edition : Chapter 6 : 224-245 8. Kloth, Le and Feeder : Rehabilitaton in Occupational Physical Therapy : Page 334-356 9. Ebnezer : Essentials of Orthopaedics and applied Physiotherapy: Chapter 23 : page 143-147 10. Carolyn Kisner , LynnAllencolby : Theraputic exercises Foundation and techniques : section 2 : page 140 -174 11. McKinnis, LN: Fundamentals of orthopedic radiology : Chapter 12 : Spinal cord Fractures : Page (1231-1268). 12. Daniel`s L ,Worthingham C , Muscle Testing : Techniques of Manual Examination, 5th edition : Chapter 3 : Page 35-60 13. Norkin`s CC, White DJ: Measurement of Joint Motion : A Guide to Goniometry : Chapter 4 : page 164-176 14. Morison, M.J. (Ed) . The Prevention and Treatment of Pressure Ulcers. St. Louis : Mosby, 2001 Chapter 31:The Prevention and Management of Pressure Ulcer : Page : page 636-647. 15. Arthur C. Guyton, John E. Hall : Textbook of Medical Physiology: Chapter 54 : Motor Functions Of The Spinal Cord :The Cord Reflexes: Page 622-632. 16. Kenneth W. Lindsay, Ian Bone : Neurology and Neurosurgery Illustrated : 3rd edition : Chapter 22 : Spinal cord and Root compression. Page : 377-390. 17. Kissner Carolyn, Lynn Allen Colby : Theraputic Exercises Foundation and Techniques : Chapter 14, Chapter 15 :The Spine : Subacute , Chronic and Postural Problems : Page 531-576. Journals Referred: 1. Houte SV, Vanlandewijck Y (2006) Respiratory muscle training in persons in persons with spinal cord injury : A systematic review: Respiratory medicine : 100 , (1886-1895). 2. Waters RL , Adkins Rh (1991) Definition of Weurmser LA (2007) Spinal cord injury medicine : Epidemiology and classifications : Arch Phys Medical Rehabilitation : 88, (S49-S54). 3. Nobunga AI, Go BK : Recent Demographics and injury trend sin people served by model spinal cord injury care system : Arch Physical Medicine Rehabilitation : 80,1372-1382. 4. Andrew Swain, David Grundy : ABC of spinal cord injury : Chapter 1 : At the site of accident : Page (112-143). 5. Waters RL, Adkins RH : Definition of complete spinal cord injury: Paraplegia 29 , 573-581. 6. Comarr , AE : Autonomic Dysreflexia (Hyper reflexia) , Journal Spinal cord , 1997 : page 345-354 7. Erickson, RP : Autonomic Hyperreflexia : Pathophysiology and medical management. Journal : Archives of physical medicime and rehabilitation, 1980 : 61:431 8. Lamount LS: A Comparison of two arm exercises in patients with paraplegia: Journal : paraplegia : 1996, 61: Page 441-567 9. Hussey RW and Stauffer ES : Spinal Cord injury: Requirements for ambulation: Journal : Archieves of Physical medicine and rehabilitation 1973 : 54:544. 10. Mikel berg R, Reid S : Spinal cord lesion and lower extremity bracing: An overview and Follow up study : Paraplegia , 1999 : 379, 19. 11. Bernardi M, Et al : The Efficiency of walking of paraplegic patients using reciprocal gait orthosis : Paraplegia : 2000 : 78 : 552-559 12. Sipski ML, Delisa JA : Functional electrical stimulation spinal cord injury rehabilitation A review of literature. Journal : Physical therapy : 56 : 778-789. Web site referred 1) 2) 3) 4) 5) 6) http://www.google.com http : // www.yahoo.com http:// www.searchi.com http:// www.meditech.com http://www.emedicine.com http://www.medscape.com 7) http:// www.pubmed .com 8) http:// bartleyby.com APPENDICES APPENDIX- (a) APPENDIX-(b) FORMAT FOR CASE REPORT-1 (please note it is of a different project) Name: Mrs. Kamlesh Age: 51 years Gender: Female Occupation: House wife Any other recreational activity: No Address: Railway Road, New Defence Colony, Muradnagar, Ghaziabad Chief Complaint: Patient complaints of Low back pain since 3-4 months with the pain on the left side of buttocks. History of Past Illness A) History of Previous similar Problem: Same type of illness occurs 2 year back, but the intensity of episode was less problematic then present. Any Previous traumatic History: History of fall from the stairs 2 years back. History of Present Illness: A) Episode of illness: The illness started 8-9 years back. The episode is of recurrent low back pain with aggravation of symptom since 3-4 months. This is second episode of illness. B) Onset : (i) PathologicalYes a) Sudden - N b) Gradual -Y No (ii) Traumatic- Mechanism of injuryC) Site of pain: Pain is in lower lumbar region and the left side of buttocks D) Is there is any radiation of pain: Yes/No- Y If yes: where it goes- It radiated form the lower back to the left side of buttocks thigh. E) Is any paraesthesia / numbness / tingling sensation: No F) Most preferred position of the patient: Lying in the supine position. G) Sleeping position of the patient: Patient preferred to lie in the right side lying position. H) Mattress used: Hard Surface I) Any other history: No Medical History Diabetes √ Y/N Hypertension √ Y/N till mid of Cardiac disease √ Y/N Cancer √ Y/N Tuberculosis √ Y/N Infection √ Y/N Repetitive Coughing √ Y/N √ Y/N Any other medical problem Drug History Past drugs History: No Present drug History: On Phase Medications - Analgesic Allergic to any Drug: No Surgical History Any surgery: Hysterectomy has been done 5 years back. Date of Surgery: Not known Any complication after Surgery: No. Bed stay after Surgery: 15 -20 days. Occupational History: - Home maker. Personal History: Smoking: No Alcohol: No Dietary Habits: Regular History of Constipation: No Other Details: Fever: N Malaise: N Any other joint problem: N Any bladder/ bowel symptoms like incontinence or retention N Any respiratory problem N Symptoms suggestive of major neurological disturbances Frequency of episodes of pain: N 1 attack before 8 years 2 attack before 2 years 3 attack before 3 months Intensity (VAS) (On first visit) - 9 out of max. of 10 Type of Pain: Superficial- X Deep- √ Nature of Pain: Sharp- X √ Dull- Aggravating Factors: Pain is aggravated by prolonged sitting, standing, and bending forward. Relieving Factors: Patient got relief after lying in right side lying position. Does pain aggravates with coughing, sneezing: N (But previously it was present) On Observation: Body type: X Ectomorphic o √ Mesomorphic Endomorphic X Gait: Patient walks with the lordotic posture and takes precautionary measures during walking to avoid the jerk. Assistive device: No Attitude of patient: Normal Lethargic √ X Tense Over anxious X X X Bored X Spinal posture: Standing: Patient was having protruded neck with excessive lumbar Lordosis. Lying: Patient lies in supine lying position and avoids bending forward while getting up from bed. Spinal curvature: Lumbar spine: Normal lordosis X Excessive lordosis √ X √ X √ X Flat back Scoliosis Sway back X Thoracic spine: Normal Kyphosis √ Excessive kyphosis X Scoliosis Any Step off sign: No. Any presence of tuft of hairs: No Others: On Palpation No Muscle tone (Lumbar muscle): Tone Increased Tenderness: Present Site: Left PSIS and L3-L4 spinous process. Odema: Absent Swelling: Absent On Examination: MOVEMENTS: JOINT MOVEMENTS ACTIVE PASSIVE LUMBAR FLEXION P, TR P,TR EXTENSION NP NP SIDE FLEXION ROTATION P- PAINFUL NP- NON PAINFUL IR-INITIAL RANGE MR- MID RANGE TR- TERMINAL RANGE LEFT RIGHT LEFT RIGHT NP P NP P LEFT RIGHT LEFT RIGHT NP NP NP NP RANGE OF MOTION: JOINT MOVEMENTS ACTIVE PASSIVE LUMBAR SPINE Flexion 0-74* 0-75* Extension 0-18* 0-20* Side Flexion RIGHT LEFT RIGHT LEFT 62-47 62-49 62-48 62-50 *- signifies taken from the inclinometer END FEELS:Lumbar Flexion: Tissue Stretch Lumbar Extension: Tissue Stretch Lumbar Side Flexion: Lumbar Rotation: JOINT HIP JOINT Right Tissue Stretch Left Tissue Stretch Right Tissue Stretch Left Tissue Stretch MOVEMENTS Flexion ACTIVE PASSIVE Right Left Right Left 0-100 0-100 0-110 0-110 Extension 0-15 0-15 0-15 0-15 Abduction 0-35 0-35 0-40 0-40 Adduction 0-20 0-20 0-25 0-25 Internal Rotation 0-35 0-35 0-35 0-35 External Rotation 0-45 0-45 0-45 0-45 END FEELS:Hip Flexion: Right- Tissue Stretch Left- Tissue Stretch Hip Extension: Right- Tissue Stretch Left- Hip Abduction: Right- Tissue Stretch Tissue Stretch LeftHip Adduction: Right- Tissue Stretch Tissue Stretch Left- Tissue Stretch MANUAL MUSCLE TESTING OF LUMBAR SPINE 1) Abdominals : 4 2) Lumbar Extensors : 4 MANUAL MUSCLE TESTINGOF HIP 1) Hip Flexors: 2) Hip extensors: 3) Hip Adductors: 4) Hip abductors: 5) Hip Internal rotators: 6) Hip External Rotators: Left- 4+ Right- 4+ Left- 4+ Right- 4+ Left- 4+ Right- 4+ Left- 4+ Right- 4+ Left – 4+ Right- 4+ Left- 4+ Right- 4+ MUSCLE LENGTH TEST: Hamstring test: Normal Rectus femoris test/ Ely’s test: Normal MYOTOMES: Affected myotomes are: L3, L5 DERMATOMAL EXAMINATION: Affected Dermatomes are: L3, L4, L5 SPECIAL TEST: SLR: Negative for neural tissue Slump test- Positive Prone Knee Bending – Negative Bowstring test – Positive Valsalva maneuver- Negative ANY OTHER FINDINGS: PROVISIONAL DIAGNOSIS: Lumbar PIVD (L3, L4, L5) WITH RADICULOPATHY INVESTIGATIONS: MRI FINDING: MRI reveals: Disc Degeneration at L4-L5 levels Diffuse Posterior disc herniations with extrusion at L5-S1 Diffuse Posterior herniations with annular tear at L4-L5 level Disc bulge at L3-L4 DIAGNOSIS: LUMBAR PIVD (L3- L4-L5) without radiculopathy to left buttocks. PHYSIOTHERAPY TREATMENT: Treatment A: (10 DAYS) 1) Hot pack for 15 minutes 2) Interferential Therapy- 10 minutes, Four pole vector 45 degree scan, square waveform 3) Traction: 20 Kg, intermittent traction with hold time 5seconds and relax time 20 second for the duration of 10 minutes is given in straight leg position. Treatment B: (Next 10 DAYS) 1) Hot pack for 15 minutes 2) Transcutaneous Electrical Nerve Stimulation- HI TENS, 2 channels, 1st at the nerve roots of L3, L4, and L5. 2nd channel at the nerve course at left buttocks for 15 minutes Treatment C: (Next 5 days) 1) Ultrasound at the L4-L5 level- pulsed 1.2W/cm2 for 5minute and at the left sacroiliac joint pulsed 0.8 W/cm2 for 5 minutes 2) Transcutaneous Electrical Nerve Stimulation- HI TENS, two channels, one at the nerve roots of L3, L4, and L5. two channel at the nerve course at left buttocks for 15 minutes HOME PROGRAM AND ERGONOMICS: 1) Patient is advised to use the lumbosacral orthosis to support the back during travelling. 2) Patient is advised for hot fomentation at home. 3) Patient is advised to lying in prone lying position for at least 15 minutes duration twice in a day. 4) Patient is explained about the proper sitting, standing, lying, and lying to standing, doing the household activities in a proper way. 5) Patient is advised to take rest and to avoid the forward bending as much as the patient can avoid. Exercises: Protocol A: Pelvic tilting Hamstring Stretching Spinal Rotation Calf Stretching Neck Raising Knee Rolling These exercises are advised to be done twice daily for the 10 seconds hold time and 10 repetitions. Protocol B: Lying in extension Extension exercises Back and Gluteal exercise PROGRESS NOTE: Pain Reduction Progress: Visual Analog Scale (VAS): Dated: 0 5 No pain Mild Pain 10 Severe Pain 4/3/10- 5 out of max 10 9/3/10- 3 out of max 10 17/3/10- 1out of max 10 The patient had the treatment A for 10 days continuous then the patient pain subsided to the lower lumbar back and slightly to the left buttocks area. All the lumbar muscle spasm has been also reduced. After 10 days the Treatment plan B started and continued for the 7 days. Now the pain was reduced to a limit and patient was able to do her ADL’s. Along with the treatment plan B, the patient was advised to start the exercise protocol A. But the patient had the slight tenderness at the lower lumbar spinous process. After that the treatment plan C was started for 5 days. Pictures Of assessment: Posture assessment: Tenderness checking: Fig 1 & 2 Fig 1 Fig 2 Two tender points: Fig 3 Fig 3 Lumbar movement assessment: Lumbar flexion and extension Fig 4 & 5 Fig 4 Fig 5 Measurement of lumbar range by inches tape (schobber’s test) Measuring Lumbar Flexion: Fig 6 Fig 6 fig 7 Measuring Lumbar Movement by Inclinometer: Fig 8 Fig 9 Special test: PKB Fig 10 SLR Test Slump Test Fig 12 APPENDIX ASSESSMENT SCALES Scale For Assessment Of Spinal Cord injury ASIA Scale Impairment Scale Fig 11 Scale For Assessment Of Spasticity Spasm Frequency Scale Modified Ashworth Scale Scale for Assessment Of Pressure Sore Risk Bradens scale Scales For Assessment Of Activities of Daily Living Barthel Index Scale Functional Independence Measure Scale Scale For Assessment Of Ambulation Walking Index Scale For Spinal Cord Injury ASIA Scale ( Standard neurological classification of spinal cord injury ) Impairment Scale A - Complete : No motor or sensory function is preserved in the sacral segment S4 -S5 level B - Incomplete : Sensory but not motor function is preserved below the neurological level and includes the sacral segments S4- S5 C - Incomplete : Motor function is preserved below the neurological level and more than half of the key muscles below the neurological level have a muscle grade less than 3 . D- Incomplete : Motor function is preserved below the neurological level and at least half of the key muscles below the neurological level have a grade of 3 or more E- Normal : Motor and sensory function is normal SCALES FOR ASSESSING SPASTICITY Spasticity Rating Scale Spasm Frequency Scale 0 - No spasms 1 - One spasm or fewer per day 2 - Between one and five spasms per day 3 - Between five and nine spasms per day Ten or more spasms per day 4 - Modified Ashworth Scale 0 - No increase in muscle tone 1 - Slight increase in muscle tone, manifested by a catch and release or by minimal resistance at the end range of motion when the part is moved in flexion /extension abduction or adduction 1+ - Slight increase in muscle tone, manifested by a catch, followed by minimal resistance throughout the remainder (less than half) of the ROM 2 - More marked increase in muscle tone through most of the ROM, but the affected part is easily moved 3 - Considerable increase in muscle tone, passive movement is difficult SCALE FOR ASSESSING PRESSURE SORE RISK Braden Scale Patients Name _____________________________________ Evaluators Name Name________________________________ Date of Assessment Sensory perception Ability to respond meaningfully to pressure-related discomfort Completely Limited Unresponsive (does not moan, flinch, or grasp) to painful stimuli, due to diminished .level of consciousness or sedation / limited ability to feel pain over most of body Very Limited Responds only to painful stimuli . Cannot communicate discomfort except by moaning or restlessness / has a sensory impairment which limits the ability to feel pain or discomfort over 2 of body. Slightly Limited Responds to verbal commands, but cannot always communicate discomfort or the need to be turned / has some sensory impairment which limits ability to feel pain or discomfort in 1 or 2 extremities. No Impairment Responds to verbal commands pain or discomfort . . Has no sensory deficit which would limit ability to feel or voice Moisture Degree to which skin is exposed to moisture Constantly Moist Skin is kept moist almost constantly by perspiration, urine, etc. Dampness is detected every time patient is moved or turned. Very Moist Skin is often, but not always moist .Linen must be changed at least once a shift. Occasionally Moist Skin is occasionally moist, requiring an extra linen change approximately once a day. Rarely Moist Skin is usually dry, linen only requires changing at routine intervals. Activity Degree of physical activity Bed fast Confined to bed. Chair fast Ability to walk severely limited or non-existent . Cannot bear own weight and/or must be assisted into chair or wheelchair. Walks Occasionally Walks occasionally during day, but for very short distances, with or without assistance . Spends majority of each shift in bed or chair Walks Frequently Walks outside room at least twice a day and inside room at least once every two hours during waking hours . Mobility Ability to change and control body position Completely Immobile Does not make even slight changes in body or extremity position without assistance Very Limited Makes occasional slight changes in body or extremity position but unable to make frequent or significant changes independently. Slightly Limited Makes frequent though slight changes in body or extremity position independently . No Limitation Makes major and frequent changes in position without assistance. Nutrition Usual food intake pattern Very Poor Never eats a complete meal . Rarely eats more than a of any food offered . Eats 2 servings or less of protein (meat or dairy products) per day . Takes fluids poorly . Does not take a liquid dietary supplement /or maintained on clear liquids or IV for more than 5 days. Probably Inadequate Rarely eats a complete meal and generally eats only about 2 of any food offered. Protein intake includes only 3 servings of meat or dairy products per day. Occasionally will take a dietary supplement / receives less than optimum amount of liquid diet or tube feeding Adequate Eats over half of most meals . Eats a total of 4 servings of protein (meat, dairy products per day . Occasionally will refuse a meal, but will usually take a supplement when offered / is on a tube feeding or TPN regimen which probably meets most of nutritional needs Excellent Eats most of every meal . Never refuses a meal . Usually eats a total of 4 or more servings of meat and dairy products . Occasionally eats between meals . Does not require supplementation. Friction and shear Problem Requires moderate to maximum assistance in moving. Complete lifting without sliding against sheets is impossible. Frequently slides down in bed or chair, requiring frequent repositioning with maximum assistance . Spasticity , contractures or agitation leads to almost constant friction. Potential Problem Moves feebly or requires minimum assistance. During a move skin probably slides to some extent against sheets, chair, restraints or other devices. Maintains relatively good position in chair or bed most of the time but occasionally slides down. No Apparent Problem Moves in bed and in chair independently and has sufficient muscle strength to lift up completely during move . Maintains good position in bed or chair. SCALES FOR ASSESSING ACTIVITIES OF DAILY LIVING Functional Independence Measure ( FIM SCALE ) The Functional Independence Measure (FIM) scale assesses physical and cognitive disability. Fim scale Self-care 1. Eating 2. Grooming 3. Bathing/showering 4. Dressing upper body 5. Dressing lower body 6. Toileting 7. Swallowing Sphincters 1. Bladder management 2. Bowel management Mobility 1. Transfers : bed/chair/wheelchair 2. Transfers : toilet 3. Transfers : bathtub/shower 4. Transfers : car 5. Locomotion : walking/wheelchair 6. Locomotion : stairs 7. Community mobility Barthel index Activity Score Feeding 0 - unable 5 - needs help cutting, spreading butter, etc., or requires modified diet 10 - independent ______ Bathing 0 - dependent 5 - independent (or in shower) ______ Grooming 0 - needs to help with personal care 5 - independent face/hair/teeth/shaving (implements provided) Dressing 0 - dependent 5 - needs help but can do about half unaided 10 - independent (including buttons, zips, laces, etc.) ______ Bowels 0 - incontinent (or needs to be given enemas) 5 - occasional accident 10 - continent Bladder 0 - incontinent, or catheterized and unable to manage alone 5 - occasional accident 10 - continent ______ Toilet use 0 - dependent 5 - needs some help, but can do something alone 10 - independent (on and off, dressing, wiping) ______ Transfers ( bed to chair and back ) 0 - unable, no sitting balance 5 - major help (one or two people, physical), can sit 10 - minor help (verbal or physical) 15 - independent ______ Mobility (on level surfaces) 0 - immobile or < 50 yards 5 - wheelchair independent, including corners, > 50 yards 10 - walks with help of one person (verbal or physical) > 50 yards 15 - independent (but may use any aid; for example, stick) > 50 yards ______ Stairs 0 - unable 5 - needs help (verbal, physical, carrying aid) 10 - independent ______ TOTAL (0–100): ______ SCALE FOR ASSESSING AMBULATION Walking index scale for spinal cord injury (WISCI II) Physical limitation for walking secondary to impairment is defined at the person level and indicates the ability of a person to walk after spinal cord injury. The development of this assessment index required a rank ordering along a dimension of impairment, from the level of most severe impairment (0) to least severe impairment (20) based on the use of devices, braces and physical assistance of one or more persons. Level Description 0 - Client is unable to stand and/or participate in assisted walking. 1 - Ambulates in parallel bars, with braces and physical assistance of two persons, less than 10 meters. 2 - Ambulates in parallel bars, with braces and physical assistance of two persons,. 10 meters. 3 - Ambulates in parallel bars, with braces and physical assistance of one person, 10 meters. 4 - Ambulates in parallel bars, no braces and physical assistance of one person 10 meters. 5 - Ambulates in parallel bars, with braces and no physical assistance 10 meters. 6 - Ambulates with walker, with braces and physical assistance of one person, 10 meters. 7 - Ambulates with two crutches, with braces and physical assistance of one person 10 meters. 8 - Ambulates with walker, no braces and physical assistance of one person, 10 meters . 9 - Ambulates with walker, with braces and no physical assistance, 10 meters. 10 - Ambulates with one cane/crutch, with braces and physical assistance of one person , 10 meters 11 - Ambulates with two crutches, no braces and physical assistance of one person , 10 meters 12 - Ambulates with two crutches, with braces and no physical assistance 10 meters 13 - Ambulates with walker, no braces and no physical assistance, 10 meters. 14 - Ambulates with one cane/crutch, no braces and physical assistance of one person , 10 meters 15 - Ambulates with one cane/crutch, with braces and no physical assistance 10 meters 16 - Ambulates with two crutches, no braces and no physical assistance, 10 meters. 17 - Ambulates with no devices, no braces and physical assistance of one person, 10 meters 18 - Ambulates with no devices, with braces and no physical assistance, 10 meters. 19 - Ambulates with one cane/crutch, no braces and no physical assistance 10 meters 20 - Ambulates with no devices , no braces and no physical assistance, 10 meters.