Scalp Window
advertisement

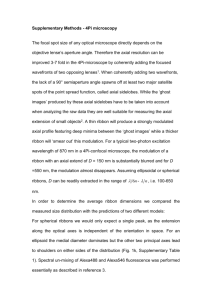
eEdE-84-9486 J Starkey1, M Fujii1, J Kim2, T Moritani3, Y Numaguchi1 1 St. Luke's International Hospital, Tokyo, Japan, 2Brigham & Women’s Hospital, Boston, MA, 3University of Iowa Hospitals and Clinics, Iowa City, IA Disclosures|None The authors have no conflicts to disclose. | Aims Scalp anatomy & trauma Scalp injuries are common Imaging features of infant scalp injuries related to birth trauma have been well described but adult traumatic scalp lesions have not. We aim to teach scalp gross and imaging anatomy and CT and MRI imaging appearance of various traumatic scalp injuries. + 24 yo M following motor vehicle accident Axial CT | Outline Scalp anatomy & trauma 1 4 Scalp Window Blood Supply 2 5 Layers Cases 3 6 Terms Extent | Terms How to describe soft tissue injury Contusion + Hematoma + Laceration + Poorly defined Well-defined Soft-tissue defect Blood products dispersed within a soft tissue without aggregation, likely due to crushed arterioles and venules. May have a similar appearance to other soft tissue fluids (e.g. edema) or other processes (e.g. scarring, infiltrating infection or malignancy, etc.). A “body of blood”, in other words a blood collection with clear borders. May have a similar appearance to other fluid collections (e.g. infection, injection sites, cysts, seromas, etc.) A soft tissue defect of the skin and deeper scalp tissues. | Outline Scalp anatomy & trauma 1 4 Scalp Window Blood Supply 2 5 Layers Cases 3 6 Terms Extent | CT scalp window Easily evaluate the scalp Makes tissues of the scalp discernable for easy visualization of site of impact, especially when contusions/ hematomas are mild/small. W: 220 L: -20 Axial Bone Window Axial Brain Window + Axial Scalp Window + + | Case 54 yo M with fall, rule out bleed Axial Scalp Window Axial Brain Window + Axial Bone Window + + This skull fracture was missed initially. The scalp window makes the scalp contusion easy to find compared to a standard brain window, allowing for careful search for an underlying fracture. Even though a subtle fracture such as this does not generally require treatment, the patient may complain of continuing headache and come back for repeat imaging (e.g. to look for new bleeding), at which time the fracture would be even less obvious. | Outline Scalp anatomy & trauma 1 4 Scalp Window Blood Supply 2 5 Layers Cases 3 6 Terms Extent | Anatomy Scalp layers schematic 1. Epidermis/dermis 2. Subcutaneous layer 3. Galeal aponeurosis 4. Loose connective tissues 5. Periosteum 1 2 The loose connective tissue layer (4, subgaleal/ subaponeurotic space) is where most bleeding occurs because the layers above it can move freely on it and this layer is where the arteries run, just under the galea. 3 4 5 The thickness of the loose connective tissues layer depends on the area of the skull. It is often very thin. The periosteum is uniformly thin and highly adherent, especially at sutures. | Anatomy Scalp gross 1. Epidermis/dermis 2. Subcutaneous layer 3. Galeal aponeurosis 4. Loose connective tissues 1 5. Periosteum 2 3 4 0 cm 1 cm 5 5 This is an intraoperative image of the temporoparietal region. The subgaleal (subaponeurotic) plane is relatively easy to dissect, while the periosteum requires a special tool to remove. | Anatomy Scalp layers on CT 1. Epidermis/dermis 1 2. Subcutaneous layer 2 3. Galeal aponeurosis 3 4. Loose connective tissues 4 5. Periosteum 5 The galeal aponeurosis and loose connective tissues are thin in many areas. The periosteum is non-visualized except under rare circumstances (e.g. calcification). | Anatomy Scalp layers on MRI 1. Epidermis/dermis 2. Subcutaneous layer 3. Galeal aponeurosis 1 4. Loose connective tissues 2 5. Periosteum 3 4 5 Axial MRA. The resolution and intensities of tissues vary with the sequence, but the fibrous galea and periosteum are hypointense. The periosteum is not normally visible unless lifted off the bone (e.g. by blood). | Cases Bumps Case 1: 55 yo M, rule out injury Axial T1 Axial T1 Fat sat + + Axial T2 Axial T2 Fat sat Case 2: 38 yo M, fall + + Axial CT + Axial CT Zoomed These subgaleal lipomas nicely demonstrate the hypointense aponeurosis on T1/T2 and hyperdense aponeurosis on CT. Unlike subcutaneous lipomas which move freely because of the underlying loose connective tissues, lipomas in the loose connective tissues layer are immobile on physical exam. Though trauma brought attention to them, these lesions are incidental findings. + | Cases Classic pediatric Case 1: 10 month old, fall Axial CT Axial T2 + + Axial T1 Sagittal T2 Case 2: 17 month old, fall + + Axial T2 Coronal T2 + + Axial T2 Coronal T2 Case 1: “Classic” subgaleal hematoma. In an infant, the subgaleal space can hold enough blood to cause shock and death. Most cases are caused by birth trauma. Case 2: Subperiosteal hematoma. The galeal aponeurosis is lifted with a small subgaleal collection. More centrally, the periosteum can be seen, with a hematoma underneath, caused by a skull facture. + + | Case 78 yo F, fall Axial Scalp Window Axial FLAIR + Axial MRA + Parietooccipital subgaleal hematoma in typical configuration adjacent to the skull. Note the hypointense aponeurosis visible on both FLAIR and MRA. On initial CT the hematoma is limited to the right but spreads to the left side on subsequent MRI obtained for other reasons. + | Outline Scalp anatomy & trauma 1 4 Scalp Window Blood Supply 2 5 Layers Cases 3 6 Terms Extent | Extent Loose connective tissues Anterior-Posterior: The galeal aponeurosis is a thin fibrous sheet that connects to the frontalis muscle anteriorly, which continues to the periorbital region to contact the superior nasal bridge and run beneath the orbitalis muscles. Therefore, hematomas that occur in the loose connective tissues can extend anteriorly and inferiorly to involve the periorbital and superior nasal regions. This is why trauma remote from the orbits can still cause a “black eye.” Posteriorly, the aponeurosis connects with the occipitalis muscle. Lateral: The aponeurosis connects with the temporalis muscle and runs along the superficial temporal fascia, part of what surgeons term the superficial muscular aponeurtic system (SMAS). Therefore, hematomas which arise in the subgaleal space and extend laterally and inferiorly will not enter into the temporal fat pads. They can extend to the auricularis muscles at the more posterolateral spaces. Images this slide courtesy of Visible Body (www.visiblebody.com) | Extent Anterolateral spaces coronal 3a The aponeurosis (3a) combines anteriorly and inferiorly to become the superficial temporal fascia (3b). 3a 1 5a 2 1 5a 4a 4b 2 4a Deep to the aponeurosis is the superficial temporal fat pad (4a) and the deep temporal fat pad (4b), covered by the superficial and deep layers of the temporalis fascia. These and the temporalis muscle (5a) fill the temporal fossa. The gateway of the superficial temporal artery scalp branches is through the anterior superficial temporal fat pad. 1. Epidermis/dermis 2. Subcutaneous layer 4b 3a/b. Galeal aponeurosis/superficial temp. fascia 4a/b. Superficial & deep temporal fat pads 5b 3b 5b 3b 5a/b. Temporalis/masseter muscles | Extent Anterolateral spaces coronal 3a When contusions or hematomas in the subaponeurotic (subgaleal space) occur, they will remain outside of the superficial temporal fascia and temporal fat pads (4a/4b). At the level of and inferior to the zygoma, the aponeurosis becomes less well defined and blood can extend deeper into the subcutaneous tissues (3b). 3a 1 5a 2 1 5a 4a 4b Potential space for subgaleal hematoma. 2 4a 1. Epidermis/dermis 2. Subcutaneous layer 4b 3a/b. Galeal aponeurosis/superficial temp. fascia 4a/b. Superficial & deep temporal fat pads 5b 3b 5b 3b 5a/b. Temporalis/masseter muscles | Extent Anterolateral spaces axial Patient 1 Axial CT Patient 2 + Axial CT Patient 3 + Axial T2 The same structures are readily apparent in 3 different patients on CT/T2. The orbicularis oculi muscle is continuous with the superficial temporal fascia, a continuation of the galeal aponeurosis. The superficial and deep temporalis fascia define the superficial and deep temporal fat pads, respectively. + | Case 48 yo F, fall Axial Scalp Window Axial Scalp Window + Axial Scalp Window + Left frontal subgaleal hematoma. The superior portion of the superficial temporal fat pad maintains normal density; note that in this location fat will be under the hematoma, not because the hematoma is in the subcutaneous fat but because fat from the temporal fossa is located deeper. Blood extending to the skin surface and small air bubbles in the hematoma indicate a small laceration. + | Case 75 yo M, motor vehicle accident Axial Scalp Window Axial Scalp Window + Axial Scalp Window + + Note that the bilateral subgaleal hematomas connect in the midline and extend beneath the frontalis and orbicularis muscles. The superior portion of the superficial temporal fat pad maintains normal density. A small laceration is present on the right. | Case 78 yo F, fall Axial Scalp Window Axial FLAIR + Coronal FLAIR + Left subgaleal hematoma extends to the left superior nasal area on initial CT. On both the CT and an MRI performed several days later, the blood products are limited to the space outside of the left superficial temporal fascia, with the underlying superficial and deep temporal fat pads uninvolved. + | Case 29 yo M, fall Axial Scalp Window Axial Scalp Window + Axial Scalp Window + Different 29 yo on axis to compare. Potential pitfall: some people, particularly young adult males, have large temporalis muscles. These can mimic hematoma, especially if the head positioning is off axis, making one side more prominent than the other. Note that the overlying subcutaneous tissues are normal, however. + | Outline Scalp anatomy & trauma 1 4 Scalp Window Blood Supply 2 5 Layers Cases 3 6 Terms Extent | Blood supply ECA & ICA branches Note that arteries tend to run at the lower dermis or just on top of the aponeurosis. Both the ECA and ICA supply the scalp. Blood supply is derived mostly from the external carotid artery: superficial temporal artery, main branch passes anterior to the tragus in the deep temporal fat bad. The occipital artery supplies the posterior scalp. The anterior scalp is supplied partially by branches of the facial artery and partially by two small branches of the ICA’s ophthalmic artery (supraorbital a., supratrochlear a.) that exit from the superior orbit. ICA and ECA vessels anastomose freely. | Case 74 yo M, fall Axial Scalp Window Axial MRA + Axial MRA + Left parietooccipital subaponeurotic hematoma on initial CT. MRA obtained subsequently for other reasons revealed enlargement of the hematoma. A branch of the left occipital artery can be clearly seen within the hematoma as the source of bleeding. Note the clear depiction of the aponeurosis. + | Outline Scalp anatomy & trauma 1 4 Scalp Window Blood Supply 2 5 Layers Cases 3 6 Terms Extent | Case 23 yo F, fall Axial Scalp Window Axial Subdural Window + Axial Subdural Window + Right frontal subcutaneous glass. On further questioning, the patient had fallen through glass. A small laceration with mild hemorrhage and high density foreign body is present. Safety glass (i.e. leaded glass) is hyperattenuating. Wood or plain glass are mildly hyperattenuating but can still often be identified. + | Case 79 yo M, fall Axial Scalp Window Axial Scalp Window + Axial Scalp Window + + Cutaneous/subcutaneous benign calcifications. Perhaps a foreign body such as small grains of dirt/sand could have a similar appearance, but the round shape and dermal location are consistent with benign skin calcifications. Further, the subjacent soft tissues have no signs of injury. | Case 45 yo F, presenting with domestic abuse Axial Scalp Window Axial Scalp Window + + Axial Scalp Window Axial Scalp Window + + Axial Scalp Window Axial Scalp Window + + Axial Scalp Window Axial Bone Window Cosmetic procedure changes. Images demonstrate high density along the frontal bone, an interior nasal bone implant, and density in the area below the orbicularis muscles, consistent with forehead filler injections, cheek filler injections, and rhinoplasty. The patient did not have radiological evidence of acute trauma. + + | Case 24 yo M, grazed by train Axial Scalp Window Axial Scalp Window + Coronal Scalp Window + + “Scalping” type injury. The patient has subgaleal blood and air with a large laceration on the right running anterior to posterior with complete separation of the aponeurosis from the skull superiorly and on the contralateral side. | Summary Scalp anatomy & trauma 1 4 Scalp Window Blood Supply 2 5 Layers Cases 3 6 Terms Extent Use contusion, hematoma, and laceration correctly. Hematomas can spread anteriorly all the way to the orbits and across the nasal bridge, posteriorly to the occiput, and laterally to the periauricular regions W: 220, L: -20 for easy evaluation The ECA supplies most of the scalp with some ICA contribution anteriorly Skin, subcutaneous tissues, aponeurosis, loose connective tissues, periosteum Trauma can be accompanied by foreign bodies. Some non-traumatic entities can mimic trauma. Familiarity with scalp anatomy and various scalp injuries will help you better understand and more accurately describe these common entities. | Selected references Scalp anatomy & trauma 1. af Geijerstam JL, Britton M. Mild head injury - mortality and complication rate: metaanalysis of findings in a systematic literature review. Acta Neurochir (Wien) 2003;145:843-850; discussion 850 2. Amaral L, Chiurciu M, Almeida JR, et al. MR imaging for evaluation of lesions of the cranial vault: a pictorial essay. Arq Neuropsiquiatr 2003;61:521-532 3. Bordignon KC, Arruda WO. CT scan findings in mild head trauma: a series of 2,000 patients. Arq Neuropsiquiatr 2002;60:204-210 4. Davis DJ. Neonatal subgaleal hemorrhage: diagnosis and management. CMAJ 2001;164:1452-1453 5. Ellis H, Mahadevan V. The surgical anatomy of the scalp. Surgery - Oxford International Edition 2014;32:e1-e5 6. Fabbri A, Servadei F, Marchesini G, et al. The changing face of mild head injury: temporal trends and patterns in adolescents and adults from 1997 to 2008. Injury 2010;41:913917 7. Le TH, Gean AD. Imaging of head trauma. Semin Roentgenol 2006;41:177-189 8. Sinnatamby CS, Last RJ. Last's anatomy : regional and applied. Edinburgh ; New York: Churchill Livingstone/Elsevier; 2011 Thank you!