Airgas template
advertisement

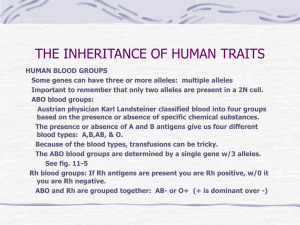
Essentials of Pathophysiology CHAPTER 13 THE RED BLOOD CELL AND ALTERATIONS IN OXYGEN TRANSPORT PRE LECTURE QUIZ (TRUE/FALSE) T F F F F There are two major types of hemoglobin—adult hemoglobin (HbA) and fetal hemoglobin (HbF). Sickle cell disease is a chronic disorder that results from changes in the size of red blood cells, not their shape. Iron-deficiency anemia affects only infants and toddlers. Hyperbilirubinemia is an increased level of serum bilirubin and very often causes cyanosis in the neonate. Thalassemias are inherited disorders of platelet synthesis that cause severe bruising and bleeding. PRE LECTURE QUIZ Aplastic Erythrocytes Mature red blood cells are also known as ____________________. The function of red blood cells is to transport ____________________ from the lungs to the tissues. If red blood cell destruction is excessive, bilirubin production is increased, causing a yellow discoloration of the skin called ______________________. Rh disease of the newborn is an example of ____________________ anemia. ____________________ anemia describes a primary condition of bone marrow stem cells that results in a reduction of all three hematopoietic cell lines—red blood cells, white blood cells, and platelets. Hemolytic Jaundice oxygen ADULT HEMOGLOBIN Two alpha chains Two beta chains Each protein chain holds one iron-containing heme group Oxygen binds to the heme groups QUESTION How many molecules of oxygen can be carried by one molecule of hemoglobin? a. 1 b. 2 c. 3 d. 4 ANSWER 4 Rationale: Each hemoglobin molecule has 2 alpha and 2 beta protein chains. Each chain contains 1 heme group. Each heme group (4 chains = 4 heme groups) is capable of carrying 1 molecule of oxygen. ERYTHROPOIESIS • Why would a man receiving chemotherapy for cancer develop anemia? decreased blood oxygen • Why would a man with renal failure develop anemia? kidneys secrete erythropoietin bone marrow stimulated creates new red blood cells RED BLOOD CELLS bone marrow creates new red blood cells: may release immature RBCs (nucleated) reticulocytes (RBCs that still have their endoplasmic reticulum) mature RBCs RBCS LAST ABOUT 120 DAYS Their membranes become weakened Because they have no nuclei, RBCs cannot make new membrane components, Why? Eventually, RBCs break as they squeeze through the capillaries mature RBCs circulate for 120 days become damaged MOST RBCS BREAK IN THE SPLEEN White blood cells living in the spleen are ready to process RBCs Creating unconjugated bilirubin Question: Why would a man with defective red blood cells develop hepatosplenomegaly? Answer: Spleen & Liver have sluggish circulation subject to clotting causing ischemia with lack of circulation to carry away toxins break in capillaries of the spleen eaten by white blood cells in the spleen, liver, bone marrow, or lymph nodes hemoglobin processed into bilirubin THE FATE OF BILIRUBIN Unconjugated bilirubin is toxic Question: Why would a man with liver failure develop jaundice? unconjugated bilirubin in blood X bilirubinemia liver links it to gluconuride jaundice conjugated bilirubin bile MALARIA PARASITES WHEN RBCS ARE DESTROYED OUTSIDE THE SPLEEN… Hemoglobinemia makes the plasma turn red Hemoglobinuria makes the urine cola-colored Question: Why was malaria called “blackwater fever?” break in capillaries outside the spleen hemoglobin released into the blood hemoglobinemia hemoglobinuria QUESTION Red blood cells (erythrocytes) are made in the ________ and destroyed in the _________. a. b. c. d. kidneys, liver kidneys, spleen bone marrow, spleen bone marrow, liver ANSWER c. bone marrow, spleen Rationale: Erythropoietin, made in the kidneys, stimulates the bone marrow to produce RBCs. Eventually, RBCs break up in the capillaries of the spleen and their hemoglobin is processed as bilirubin in the liver. CAUSES OF ANEMIA Blood loss Hemolysis Impaired RBC production SCENARIO A man had severe anemia and developed: Weakness Angina Fainting Tachycardia Sweating and pallor Pain in his bones and sternum Question: Which symptoms are caused by decreased RBCs, O2? By compensation using the GAS? By attempts to replace the RBCs? ANEMIAS OF DEFICIENT RBC PRODUCTION Iron deficiency anemia (often caused by blood loss) Megaloblastic anemias Cobalamin (Vitamin B12) deficiency (Needed for DNA replication) º Pernicious anemia Folic acid deficiency (Needed for DNA replication) Aplastic anemia (bone marrow depression) Chronic disease anemias Chronic inflammation Lymphocyte production Chronic cytokines suppress erythropoietin renal failure Erythropoietin not produced IRON-DEFICIENCY ANEMIA Hypochromic and microcytic erythrocytes Poikilocytosis (irregular shape) (poi'kə-lō-sī-tō'sĭs) Anisocytosis (irregular size) (ān-ī'sō-sī-tō'sĭs) (Rubin E., Farber J.L. [1999]. Pathology [3rd ed., p. 1077]. Philadelphia: Lippincott-Raven.) VITAMIN B12 DEFICIENCY (PERNICIOUS ANEMIA) Megaloblastic anemia Erythrocytes are large, often with oval shape Poikilocytosis and teardrop shapes Anisocytosis (Irreg. size) Neutrophils are hypersegmented (Rubin E., Farber J.L. [1999]. Pathology [3rd ed., p. 1076]. Philadelphia: LippincottRaven.) SCENARIO A boy presents with: Pallor Weakness Low red blood cell count Increased respiratory and heart rates Yellow skin Dark brown urine Enlarged spleen and liver Question: What is your diagnosis? Is he lacking RBC production or hemolytic anemia? Which symptoms are caused by decreased RBC count? By GAS? By hemolysis? QUESTION Which type of deficiency causes pernicious anemia? a. Iron b. Vitamin B6 c. Vitamin B12 d. Folic acid ANSWER c. Vitamin B12 Rationale: Intrinsic factor produced by cells of the gastric mucosa binds vitamin B12 and assists absorption of B12. When gastric mucosa cells are lacking often due to autoimmune antibodies attacking gastric mucosa production of IF is reduced and B12 is not absorbed. HEMOLYTIC ANEMIAS Membrane disorders , RBC shape and fragility Hereditary spherocytosis (shape holding inner membrane) Acquired hemolytic anemias (chemicals drugs, antibodies) hemolytic disease of the newborn-Rh incompatibility any of a group of inherited hypochromic anemias Hemoglobinopathies and especially Cooley's anemia controlled by a series of allelic genes that cause reduction in or Sickle cell disease failure of synthesis of one of the globin chains making up hemoglobin and that tend to occur Thalassemia especially in individuals of Mediterranean, African, or southeastern Asian ancestry —sometimes used with º Alpha a prefix (as alpha-, beta-, or delta-) to indicate the hemoglobin chain affected. º Beta G6PD deficiency (Glucose 6 Phosphate Dehydrogenase enzyme deficiency- limits RBC’s ATP production) G6PD G6PD Easily mistaken for malaria. Heinz bodies on the periphery SICKLE CELL DISEASE Mutation in beta chains of hemoglobin When hemoglobin is deoxygenated, beta chains link together Forming long protein rods that make the cell “sickle” SICKLE CELL DISEASE Mutation in beta chains of hemoglobin At a single location in the protein chain valine is substituted for glutamic acid Valine Glutamic acid When hemoglobin is deoxygenated, beta chains link together, forming long protein rods that make the cell “sickle” PROBLEMS CAUSED BY SICKLE CELL DISEASE Sickled cells block capillaries Acute pain Infarctions cause chronic damage to liver, spleen, heart, kidneys, eyes, bones Pulmonary infarction acute chest syndrome (Pneumonia) Cerebral infarction stroke Sickled cells more likely to be destroyed Releasing excess bilirubin Jaundice SICKLE CELL DISEASE INHERITANCE Scenario: A man has sickle trait (heterozygous for sickle cell) His wife has sickle cell disease Question: What percentage of their children will have the disease? In a population, the gene frequency of the sickle cell allele is 10% Assuming the gene is equally common in males and females and does not affect reproduction, what percentage of the next generation’s population will have sickle trait? Use the Hardy-Wienberg Equilibrum equations: p+q=1 ; p= probability of normal gene and q = prob. of Sickle q2 + 2pq + p2 =1 ; 2pq= freq of occurrence of father’s genotype, heterozygous SICKLE CELL DISEASE INHERITANCE s = Sickle Gene S= nonSickle percentage of their children s s S Ss Ss s ss ss Father has the Trait, Ss Mother has the disease, ss Possible Children’s Genotype 50% have the disease, ss 50% are Heterozygous, Ss SOLVE FOR FREQUENCY HETEROZYGOTES IN THE POPULATION Use the Hardy-Wienberg Equilibrum equations: p+q=1 ; p= probability of normal gene and q = prob. of Sickle q2 + 2pq + p2 =1 ; 2pq= freq of occurrence of father’s genotype, heterozygous Given: Frequency of Sickle gene = 10% In the Hardy-Wienberg equation q=.1 Therefore p= 1-.1=.9 or 90% of genes are normal q2 = percent with sickle disease = (.1)2 = .01 =1% Question: What is the % heterozygous From equations 2pq= 2(.1*.9) =.18 or 18% have the trait without the disease QUESTION True or False. Patients with sickle cell disease who also suffer from lung diseases are more prone to sickling. ANSWER True Rationale: Hypoxia, which is more likely to occur in lung/pulmonary disease, is an important exacerbating factor associated with increased sickling and vessel occlusion. FETAL HEMOGLOBIN HAS NO BETA CHAINS It has alpha chains and gamma chains This means it cannot sickle Persons with some fetal hemoglobin are partially protected from sickle cell disease Some treatments include inducing HbF production THALASSEMIAS Alpha Beta • Defective gene for alphachain synthesis • Defective gene for betachain synthesis • May have 1–4 defective genes • May have 1–2 defective genes • Affects both fetal and adult Hb • Affects only adult Hb • In fetus, gamma4 Hb may form; in adult, beta4 Hb may form • Alpha4 Hb may form SCENARIO A woman has β thalassemia. p219 She has pale skin and gums, fatigue, and headaches She has been treated with transfusions since childhood Her jaw is enlarged; she has had two leg fractures in the past year(Thin cortical bone w/ enlarged marrow. Bone deposition on jaw) She has Heinz bodies (precipitate aggregate of excess α chains in RBC) Her liver is enlarged; she has jaundice and liver failure Question: Which of these signs and symptoms are due to anemia, which to compensatory erythropoiesis, and which to treatment?