Understanding How to Code
Colonoscopies
Presented by Barbara Parker, CPC
Prepared by Lori Dafoe, CPC
Facts
• More than two million colonoscopies are performed each
•
•
•
•
year in the United states.
Most of them are performed on an outpatient basis.
Can be performed for screening, diagnostic, or therapeutic
purposes.
Coding can be challenging, especially those procedures that
include biopsy and polyp removal.
Accurate assignment of colonoscopy procedure codes
depends on the documentation of the procedure performed
and the technique used to perform the procedure.
Facts
• A colonoscopy includes an exam of the entire colon, from
the rectum to the cecum, and may also include examination
of the terminal ileum. In order to bill for a completed
colonoscopy, the scope must be advanced past the splenic
flexure.
Factors to Consider
Was another procedure(s) performed during the diagnostic
colonoscopy?
If so, what was the procedure(s)?
What was the technique used?
What instruments were used?
Once the above factors are determined, use the following
information as guidance to determine when each of the
following codes is reported:
CPT 45378, Colonoscopy, flexible, proximal to the splenic flexure;
diagnostic, with or without collection of specimen(s) by brushing or
washing, with or without colon decompression is used to report
diagnostic colonoscopies.
All surgical colonoscopy codes include a diagnostic
colonoscopy. Therefore, if any other procedure but a
brushing or washing is performed during the diagnostic
colonoscopy, the surgical colonoscopy should be billed using
codes 45380-45385. It would not be appropriate to report
code 45378 in addition to the therapeutic procedure.
HCPC G0105 & G0121
Effective January, 1, 1998, Medicare created HCPCS Level II codes
which are equivalent to and are used in place of CPT code 45378 when
reporting outpatient colonoscopies for screening of colorectal cancer on
Medicare patients.
Code G0105 to report a screening colonoscopy for patients who are at
high risk for colorectal cancer. High risk is an individual with one or
more of the following: close relative (sibling, parent or child) who has
had colorectal cancer or an adenomatous polyp, family history of familial
adenomatous polyposis, a family history of hereditary nonpolyposis
colorectal cancer, a personal history of adenomatous polyps, a personal
history of colorectal cancer, or inflammatory bowel disease, including
Crohn’s Disease and ulcerative colitis.
Code G0121 is used to report colonoscopies for colorectal screening on
patients not meeting criteria for high risk.
If an abnormality is found during a screening colonoscopy that results in
a therapeutic procedure (e.g., biopsy, polypectomy, excision of lesion),
then the appropriate CPT code is used instead of HCPCS Level II codes
G0105 or G0121.
Code Selection
Surgical Colonoscopy Codes are determined by the
physician’s documentation of the procedure performed.
The record must state the method used to remove the tissue,
lesion or polyp.
CPT 45384, Colonoscopy, flexible, proximal to the splenic flexure; with
removal of tumor(s), polyp(s), or other lesion(s) by hot biopsy forceps or
bipolar cautery.
This code is used when bipolar cautery and monopolary
cautery forceps are used to remove tissue.
Hot biopsy forceps, also called monopolar cautery
forceps, create heat in the metal portion of the forceps
cup by causing current to flow from the device to a
grounding pad on the patient’s body to cauterize the
lesion or polyp. Bipolar cautery uses current that runs
from one portion of the tip of the cautery device to
another to cauterize and remove a lesion or polyp.
CPT 45385, Colonoscopy, flexible, proximal to the splenic flexure; with
removal of tumor(s), polyp(s), or other lesion(s) by snare technique.
This is the most often used technique for performing a
polypectomy during a colonoscopy. When the snare cautery
technique is used, a wire loop is heated and then placed
around the desired piece of tissue or polyp to shave off the
polyp or lesion. It’s important to note that the snare device
may be used with or without heat or cautery. The key term
in using this code is “snare” removal. Hot snare, cold snare,
monopolar snare and bipolar snare should all be reported
with code 45385.
CPT 45383, Colonoscopy, flexible, proximal to splenic flexure; with
ablation of tumor(s), polyp(s), or other lesion(s) not amenable to
removal by hot biopsy forceps, bipolar cautery or snare technique.
The description of this code is not as clear cut. It can be
misleading because it only indicates what techniques the code
should not be reported for. Hot biopsy and bipolar cautery
techniques are reported with CPT 43584. Snare technique is
reported with CPT 43585.
CPT 45383 can be reported for the ablation of a tumor,
polyp or other lesion (including arteriovenous
malformations) using a number of different devices including
heater probe, bipolar cautery prober, or argon laser, argon
plasma coagulators (APC).
Examples of CPT 45383, 45384, &
45385
45380, Colonoscopy with biopsy, single or multiple
Describes the use of forceps to grasp and remove a small
piece of tissue without the application of cautery.
The procedure note may describe the biopsy using cold
biopsy forceps, or may not mention the device at all.
The biopsy may be from an obvious lesion that is too large to
remove, from a suspicious area of abnormal mucosa, or from
a lesion or polyp so small that it can be completely removed
during the performance of the biopsy.
Colonoscopy with removal by snare technique (45385)
should not be used for the removal of a small polyp by
“biopsy” or “cold forceps” technique. All lesions or polyps
removed by cold biopsy foceps are reported using code
45380.
CPT 45380
CPT 45381, Colonoscopy, flexible, proximal to the splenic flexure; with
directed submucosal injection(s), any substance.
Reported when any substance is injected into the
submucosal. Substances include saline, India ink, methylene
blue, Botox and steroids.
For example, code 45381 would be reported for an injection
to “tattoo” an area with India ink for later identification
during a subsequent procedure.
Code 45381 should be reported as an additional service to
any other therapuetic procedure performed at the same time.
Code 45381 is not used to report injections to control
bleeding.
CPT 45381
CPT 45382, Colonoscopy, flexible, proximal to the splenic flexure; with
control of bleeding, (e.g., injection, bipolar cautery, unipolar cautery,
laser, heater probe, stapler, plasma coagulator).
Used to describe injection to control bleeding resulting from
a number of causes including diverticulosis, angiodysplasia or
prior session intervensions.
Bleeding that starts as a result of an intervention performed
during the colonoscopy, such as a polypectomy or biopsy, and
is controlled by any method is considered part of the initial
therapeutic procedure and should not be reported separately
with code 45382.
CPT 45382
Multiple Procedures
When multiple colonoscopy procedures are performed during the
same session, documentation must specifically describe the type of
lesion(s), the location of the lesion(s), and the techinique used to
perform each procedure.
One code is used to report multiple procedures using the same
technique.
Multiple codes are reported when more than one procedure was
performed using multiple techniques.
When more than one colonoscopy code is reported for the same
session, they should be listed in descending order value with
modifier -59 (Distinct procedural service) to identify that the
service was performed at a separate site.
Modifiers
Modifier 59, Separate Procedure.
Used to indicate different sites, incisions, encounters.
Example: Colonoscopy with removal of polyp at the transverse colon by
snare technique (45385) is performed at the same session as a biopsy
proximal to the splenic flexure (45380). Modifier -59 is
appropriate because the two procedures are performed on separate
lesions at separate locations. Report as 45385, 45380-59.
Modifiers
Modifier 51, Multiple Procedure.
Used to indicate multiple procedures performed at the same session
by the same provider.
Multiple procedure discount should be applied to the
reimbursement of the code, so it is very important to add this
modifier to the second and subsequent code based on RVU order.
It is not based on the order the services were performed or based
the primary procedure based on what was done to address the
patient’s illness.
Example: Colonoscopy (45378) performed at the same session as upper
endoscopy (43200). Use modifier 51 on the upper endoscopy because
RVU’s are lower than the colonoscopy. Report as 45378, 43200-51.
Modifiers
Tells the payor, “This is a service that should be processed
without a patient due balance, because it was a preventive
service with an A or B rating from the USPSTF”.
Modifier 33, Preventive Services. Used for commercial
claims.
Modifer PT, CRC screening test converted to diagnostic test
or other procedure. Used for Medicare claims.
If using these modifiers, make sure your primary diagnosis is
the v-code describing the appropriate type of screening,
followed by the diagnosis for the findings.
Modifiers
For coding purposes, the colonoscope must pass the splenic flexure.
If this is not achieved, it is an incomplete colonoscopy. The
documentation should clearly state how far the scope was inserted
and the reason for the discontinuation.
Modifier 53, Discontinued procedure. Used on physician claims.
Not to be used to report the elective cancellation of a procedure prior to
inducation of anesthesia or surgical preparation in the surgical suite.
(NOTE: Prior to January 1, 2011, providers had been instructed
to use modifier -52 to report an incomplete colonoscopy.)
Modifer 73, Discontinued procedure prior to anesthesia. Used for
facility claims.
Modifier 74, Discontinued procedure after the administration of
anesthesia. Used for facility claims.
Modifiers
Modifier 22, Increased Procedural services.
Used to denote circumstances for which a procedure was
complicated, complex, difficult, or took significantly more time
than usually required by the provider to complete the procedure.
Example: The physician performs a colonoscopy on a patient with a tortuous
colon. The gastroenterologist spends 110 minutes navigating the scope
through the twists and turns of the patient’s lower intestine.
Even when justified, it can be difficult at best to obtain higher than
normal reimbursement from payers.
The documentation should clearly describe the unusual nature of
the service to justify the additional charge!
Diagnosis Coding - Screening
Screening colonoscopy performed on a patient with no presenting signs or symptoms related to
the digestive system, but have reached the age for routine screenings should be coded using:
V76.51 Special screening for malignant neoplasm, colon.
All additional findings are reported as secondary codes.
Additional secondary codes for high risk can be used when the information is recorded in the
patient’s record:
V10.05 Personal history of malignant neoplasm, large intestine
V12.72 Personal history of colonic polyps
V16.0 Family history of malignant neoplasm, gastrointestinal tract
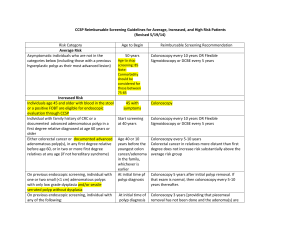
High risk is coded when any of the following conditions are noted by the provider or in the patient's
history:
Close relative (sibling, parent, or child) has had colorectal cancer or an adenomatous polyposis
Family history of hereditary nonpolyposis colorectal cancer
Personal history of adenomatous polyps
Personal history of colorectal cancer
Personal history of inflammatory bowel disease, Crohn's disease, or ulcerative colitis
Diagnostic colonoscopy performed the confirmed diagnosis should be coded. If no definitive
findings are noted, then code(s) for the symptoms prompting the service should be used.
Diagnosis Coding - Diagnostic
Diagnostic colonoscopy performed the confirmed diagnosis
should be coded.
If no definitive findings are noted, then code(s) for the
symptoms prompting the service should be used.
For example, blood in stool/hemopositive stool, bleeding from rectum,
iron deficiency anemia of unknown cause, change in bowel habits,
persistent abdominal pain.
THANK YOU!!
Presented by Barbara Parker, CPC
Prepared by Lori Dafoe, CPC
 0
0