Learning the Pathophysiology, Neuroanatomy, and
advertisement

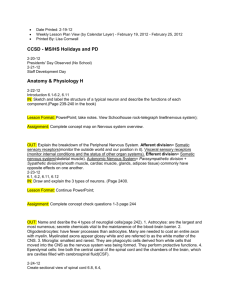
Learning the Pathophysiology, Neuroanatomy, and Neurovascular Anatomy of the Cervical Spinal Cord through Cases of Spinal Cord Infarction (eEdE-232) Jason Ginos, MD; Scott McNally, MD PhD; Melissa Cortez, DO, Edward Quigley, MD PhD; Lubdha Shah, MD University of Utah Departments of Neuroradiology and Neurology Disclosures • The authors declare that they have no conflict of interest. Objective • This educational exhibit illustrates the neuroanatomy and neurovascular anatomy of the cervical spinal cord by exploring the pathophysiology of cervical cord infarction through case examples. Introduction • The spinal cord is made up of several important tracts including: Dorsal Column Medial Lemniscus System Introduction • The spinal cord is made up of several important tracts including: • Dorsal column medial lemniscus system Introduction • The spinal cord is made up of several important tracts including: • Dorsal column medial lemniscus system • Corticospinal tracts Introduction • The spinal cord is made up of several important tracts including: • Dorsal column medial lemniscus system • Corticospinal tracts • Anterolateral system Introduction • The spinal cord is made up of several important tracts including: • Dorsal column medial lemniscus system • Corticospinal tracts • Anterolateral system • Injury to one or more of these pathways can result in localizing neurological symptoms. Introduction • Also contributing to the complexity of spinal vascular pathophysiology is considerable variation to the cervical cord vascular anatomy. Introduction • Selective catheterization of the right vertebral artery (green arrow) with radicular branches supplying the spinal cord (yellow arrow) Approach • We retrospectively reviewed radiology reports over the past 5 years at our institution looking for cases of spinal cord infarction. Images and clinical notes were reviewed in detail. Findings • We identified ten cases with imaging and clinical features supporting cervical cord infarction. • The clinical presentation and imaging findings of these cases help illustrate the functional anatomy of the cervical cord and the vascular supply. Case 1 • A 33 year-old female with a left vertebral artery dissection following neck manipulation presented with an ipsilateral cord infarction with resulting Horner and Brown-Séquard syndromes. Findings • Sagittal and axial T2 images demonstrate normal cervical cord signal. Note that the vertebral artery flow voids are normal. Findings • Sagittal and axial CTA images demonstrate a normal left vertebral artery without evidence of dissection. Findings • The symptoms persisted so follow up imaging was obtained two weeks later • Sagittal and axial T2 images demonstrate T2 hyperintensity within the left hemicord at the level of C5 (red circle). • Note that the left vertebral artery flow void is irregular and narrowed (yellow arrow). • Axial T1 weighted (MPRAGE) fat saturation image demonstrates that the left vertebral artery is dissected with luminal narrowing and intramural hematoma (yellow arrow). • Axial diffusion weighted image (DTI trace) at the same level demonstrates diffusion restriction (blue circle). Case discussion • We postulate that the vertebral artery dissection occluded a radicular branch resulting in cord infarction. • Coexistent injury to the sympathetic pathway resulted in Horner syndrome (ptosis, miosis, and anhydrosis). Brown-Séquard Syndrome • This pattern of deficits occurred as a result of direct injury to the dorsal column-medial lemniscus tracts (sensory) and the lateral corticospinal tract (motor) • The contralateral loss of pain and temperature sensation occurred via damage to the spinothalamic tract of the anterolateral system Oculosympathetic Pathway • 3 Neuron Arc • Central • Preganglionic • Postganglionic Courtesy: Anne Heyman, MD Horner’s Syndrome Anatomic Considerations • Central (First-order) • Hypothalamus, brainstem, cervical spinal cord (sympathetic pathway) • Preganglionic (Second-order) • Cervicothoracic cord, brachial plexus, pleural apex • Postganglionic (Third-order) • Cervical ganglion, CS, ICA, Cavernous sinus Case 1 Right Hemicord Infarction--Companion Case • 53 year old female status post ACDF complicated with the development of cord infarction resulting in right sided weakness and sensory loss. • Axial and sagittal T2 images demonstrate T2 hyperintensity within the right hemicord at the level of C6-C7 (red arrow). • Note the ACDF (green arrow). Case 2 • A 59 year-old male with an epidural abscess and long central segment cord venous ischemia resulting in tetraplegia and sensory loss. • Axial T2 image demonstrates T2 hyperintensity within the central cord at the level of C2 (red circle). • Note the T2 hyperintense epidural collection (green arrow). Tetraplegia • In this case, the bilateral descending and ascending pathways were damaged resulting in tetraplegia and sensory loss Case 2 Tetraplegia--Companion Case • 37 year old obese male with history of emphysema/COPD, active smoker, hypertension, bipolar disorder and steroid induced hyperglycemia who presented with acute C7 complete tetraplegia. During the hospital course the patient developed bowel ischemia with colonic perforation leading to sepsis and death. • Axial STIR image demonstrates STIR hyperintensity within the central cord at the level of C7 (red circle). • Sagittal STIR image shows a T8 compression fracture thought to be secondary to ischemic necrosis (yellow arrow). • We hypothesize that in this case the bone marrow abnormalities reflect the shared supply of the radiculomedullary arteries supplying both the vertebral body and the spinal cord resulting in ischemia. MR Imaging of Spinal Cord and Vertebral Body Infarction. William T . C. Yuh, et al. AJNR 13:145-154, January/February 1992. Case 2 Tetraplegia--Companion Case • 72 year old male with multiple comorbidities including thromboembolic supratentorial infarction and tetraplegia. Sagittal and axial T2 images demonstrate T2 signal hyperintensity within the cervical cord extending from C3 through C7 (Yellow arrows) Sagittal GRE image demonstrates linear signal hypointensity within the cervical cord extending from C3 through C7 compatible with hemorrhage (Green arrow). DTI image shows diffusion restriction within the cord as well as the occipital lobe (Red arrows). Case 2 Tetraplegia--Companion Case • 34 year old female with a complex congenital occipital-cervical abnormality status post C1 laminectomy and occiput to C3 fusion. Presenting with bilateral hand numbness and leg weakness. Sagittal and axial T2 images demonstrate T2 signal hyperintensity within the cervical cord extending from C1 through C4 (Yellow arrows). Note the susceptibility artifact from the posterior fusion hardware. Case 3 • A 58 year-old male presented with left-sided pain and temperature paresthesias. • Axial T2 image demonstrates T2 hyperintensity within the right anterolateral cord at the level of C6 (red circle). Note the left vertebral artery occlusion (yellow arrow). Axial DTI demonstrates diffusion restriction within the same region (blue circle). Case discussion • Left vertebral artery occlusion and contralateral cord infarction involving the anterolateral right hemicord. • In contrast to Case 1, this resulted in more focal injury to the spinothalamic tract given the clinical presentation. Spinothalamic Tract • The lateral spinothalamic tract transmits pain and temperature. • The anterior spinothalamic tract transmits crude touch and firm pressure. • The pathways for pain and temperature cross midline. • This gives rise to pain and temperature loss on the side contralateral to the injury. Spinothalamic Tract • The lateral spinothalamic tract transmits pain and temperature. • The anterior spinothalamic tract transmits crude touch and firm pressure. • The pathways for pain and temperature cross midline. • This gives rise to pain and temperature loss on the side contralateral to the injury. Case 4 • A 58 year-old male presented with renal cell carcinoma metastatic to the left vertebral artery and adjacent C5 vertebral body. The vertebral artery was surgically occluded with a resulting left hemicord infarct involving the corticospinal tract and resulting in left-sided weakness. • Axial T2 image demonstrates T2 hyperintensity within the left hemicord at the level of C5 (red circle). Note the postoperative changes. Case discussion • The vertebral artery was surgically occluded with a resulting left hemicord infarct involving the corticospinal tract and resulting in leftsided weakness. Case 4 Corticospinal tract--Companion Case • 57 year old male status post MVC with injury to the alar ligaments and a cervical cord injury resulting in left sided weakness. • Axial T2 image demonstrates T2 hyperintensity within the left hemicord at the level of C3-C4 (red circle). Summary • Through these cases of cervical cord ischemia, we show the various arterial and venous etiologies, including an often underappreciated contribution of the vertebral vascular supply. • Understanding spinal cord function and neuroanatomy can aid in prompt diagnosis and management of ischemic cord lesions. • A thorough clinical exam and appropriate imaging including advanced techniques such as diffusion tensor imaging can be combined to localize the injury and help predict functional outcome. References MR Imaging of Spinal Cord and Vertebral Body Infarction. William T . C. Yuh, E. Eugene Marsh, Angela K. Wang, James W. Russell , Francis Chiang, Timothy M. Koci,4 and Tony J. Ryals. AJNR 13:145-154, January/February 1992. Vascular anatomy of the spinal cord. Santillan A1, Nacarino V, Greenberg E, Riina HA, Gobin YP, Patsalides A. J Neurointerv Surg. 2012 Jan 1; 4(1):67-74. C.-É. Brown-Séquard: De la transmission croisée des impressions sensitives par la moelle épinière. Comptes rendus de la Société de biologie, (1850)1851, 2: 33-44) Multisection CT Angiography Compared with Catheter Angiography in Diagnosing Vertebral Artery Dissection. Chen CJ1, Tseng YC, Lee TH, Hsu HL, See LC. AJNR Am J Neuroradiol. 2004 May; 25(5):769-74. Clinical features and outcomes of spinal cord infarction following vertebral artery dissection: a systematic review of the literature. Hsu CY1, Cheng CY, Lee JD, Lee M, Huang YC, Wu CY, Hsu HL, Lin YH, Huang YC, Weng HH, Huang KL. Neurol Res. 2013 Sep; 35(7):676-83 Causes of Misinterpretation of Cross-Sectional Imaging Studies for Dissection of the Craniocervical Arteries. Provenzale JM, Sarikaya B, Hacein-Bey L, Wintermark M. AJR Am J Roentgenol. 2011 Jan; 196(1):45-52. Cervical transforaminal injection of corticosteroids into a radicular artery: a possible mechanism for spinal cord injury. Baker R, Dreyfuss P, Mercer S, Bogduk N. Pain 103/1-2, 2003. http://teachmeanatomy.info/neuro/pathways/ascending-tracts-sensory/brown-sequard-syndrome/