The components of inflammation.

‘Laudable pus’
the cells of inflammation.
Lecture 2
Rod Flower, WHRI, London.
The components of inflammation.
• Cells..
- Fixed cells such as vascular cells.
- Migratory cells such as PMNs.
• Mediators..
- many chemicals released into the body.
• Immune system..
-Innate.
-Acquired.
Migratory cells.
• Platelets.
• Polymorphonuclear leukocytes.
• Macrophage/monocytes.
• Lymphocytes.
• Eosinophils.
• Basophils.
• Dendritic cells.
Platelets.
• Small 2-3 m m enucleate cells.
• 150-400,000/ m l blood.
• Derived from megakaryocytes.
• Vital to haemostasis.
• Contain or generate mediators such as amines and eicosanoids.
Polymorphonuclear (PMN) cells.
• Most abundant (>50% total )
2500-7500/ m l blood.
• ‘Shock troops’ of the system.
• Early involvement in the response.
• Contain many microbiocidal weapons and enzymes.
• Phagocytic.
• Short lived.
• Crucial to host defence.
Macrophage/monocytes.
• 100-800 / m l blood. 6-7% total.
• Blood borne monocytes mature to macrophages in tissues.
• Crucial to antigen presentation.
• Secrete many important mediators and enzymes.
• Phagocytic.
• Long lived.
Eosinophils.
• Relatively small population
2.5% total; 50-400/ m l blood.
• Specialised for anti-parisitic defence.
• Granules contain enzymes and proteins with microbiocidal properties.
• Important in asthma and allergies.
Lymphocytes.
• 1000-4000/ m l blood;
30% total cells.
• Specialised for the production of antibodies and immune recognition.
• T- and B - cells.
• NK cells.
• Homing properties.
Basophils.
• 1-100/ m l blood; 0.5% total cells.
• Circulate in blood and
‘home' into tissues.
• Precursors of mast cells.
Dendritic cells.
• Macrophage – like cells.
• Distributed in blood and tissues.
• Long cytoplasmic processes.
• Intimate contact with lymphocytes.
• Play a key role in early host defence.
Fixed cells.
• Vascular endothelial cells.
• Liver cells.
• Airway cells.
• Nervous tissue.
• Many other cell types.
Vascular endothelial cells.
• Have a barrier function but can undergo fenestration.
• Contain adhesion molecules crucial for cell transmigration.
• Can elaborate mediators such as NO,
PGI
2
.
Liver cells.
• Liver cells especially
Kupffer cells are involved in phagocytic functions.
• The liver elaborates
‘acute phase’ proteins.
Airway cells.
• Airway epithelial, and other, cells play a crucial role in host defence and elaborate mucus and microbiocidal enzymes.
• Especially important in asthma and allergies.
Nervous tissue.
• Obviously important in pain transmission.
• Many receptors and enzymes in DRG cells and elsewhere are upregulated during inflammation.
• Cranial nerves and
CNS structures are also important.
Many other cells and tissues.
• Inflammation can affect virtually any structure in the body!
• Follows physical trauma, injury or infection.
Two ‘types’ of inflammation.
• Acute…
- short lived
- doesn’t always involve the immune system.
- healing usually occurs.
- little systemic disease.
• Chronic…
- long lived.
- often inappropriate.
- healing poor or absent.
- tends to be the most usual indication for therapy.
- often severe systemic effects including bone and cartilage breakdown.
The healing response.
• The ultimate objective of inflammation, it involves…
- angiogenesis.
- remodelling of damaged tissues.
- the correct hormonal and cytokine milieu.
- sometimes migrating cells also play a role
(e.g.platelets).
What goes on at the tissue level in inflammation?
• Vascular ‘fenestration’ and plasma leakage.
• Cellular degranulation.
• Leukocyte migration.
• Liver acute phase response.
Vascular changes.
• Post-capillary venules most important site.
• Extravasation of plasma proteins e.g. immunoglobulins.
• Role of PMNs in this process.
• Promotes access of protective proteins to invading organisms.
Cellular degranulation.
• Principally by PMN, monocytes, eosinophils, platelets and mast cells.
• The latter release enzymes, histamine and eicosanoids.
• Very important in allergic reactions and asthma.
Leukocyte emigration.
• Dutrochet first reported leukocyte emigration in
1824.
• Addison first induced the phenomenon experimentally in 1843.
• Multi-step paradigm for emigration developed from 1970s-1990s by several groups.
• Leukocyte emigration important in many pathologies (Epstein, 1989).
Leukocyte emigration.
• Mainly PMN, monocytes and eosinophils.
• Mediated by adhesion molecules.
• Brings cells into contact with microorganisms.
• Crucial to host defence.
Adhesion molecules.
• L-selectins.
• V- CAM & I- CAM.
• Integrins.
• PECAM.
Adhesion molecules.
• Reversible interaction with L-selectin responsible for rolling phenomena.
• More stable adhesion mediated through increases in ICAM-1 and VCAM-1 .
• Integrins ( b
1 & b
2) mediate a stable adhesion and have important signalling properties.
• Most of these adhesion molecules are up-regulated during inflammation in response to cytokines etc.
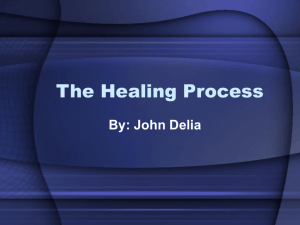
Cellular migration - free flowing.
PMN
Direction of blood flow
Vascular endothelium
selectins
- selectin adhesion.
!
- integrin attachment, signalling.
integrins
!
!
- shape change.
- pseudopodia formation.
!
PECAM
!
- extravasation..
!
- full migration.
Acute phase response.
• A diverse collection of proteins and factors including, protease and other enzyme inhibitors.
• Released in from the liver in response to many forms of inflammatory response.
• Often accompanied by a fall in albumin synthesis.
• Clinically useful marker.
Summary of lecture 2.
• Many cells participate in the development of the inflammatory response.
• Migrating cells are particularly crucial.
• Fixed tissues such as the liver secrete factors which help co-ordinate the response.
Picture credits.
• Life Art.
•
Austrian Rheumatology Teaching slides .
• ‘Mediators of Inflammation’,
GP Lewis .
• ‘Cellular and Molecular Immunology’,
Abbas et al.
•
N Goulding .
•
St Barts Hospital Medical Illustration service .
•
A du Vivier .
• Leo & Astra .
• ‘Atlas of Clinical Endocrinology’,
Besser et al.