Park, D. & Estrada, G. (2012). Pension Systems and Old
advertisement
. Pension Systems and Old")
Pension Distribution Crisis: The Right Scheme between Defined Benefit and Defined
Contribution in Solving Inadequate Pension Coverage in Singapore
A Thesis Presented to the
College of Commerce and Business Administration
University of Santo Tomas
In Partial Fulfillment
of the Requirements for the Degree
Bachelor of Science in Commerce and Business Administration
Major in Business Economics
By
Lao, Princess Chezica T.
Cruz, Carla Felize C.
Kim Eun Hyun
1
ABSTRACT
Within the past years, the pensions systems around the world have experienced inadequate
pension distributions. More and more of the retiring workers and elderly fear of old – age
poverty. The pension distribution crisis was clear and evident for more developed countries like
the OECD countries. However, this is fast approaching to other parts of the globe. In South –
East Asia, these countries were labeled to be ‘youthful countries’ where much of its population
was much relatively younger. Unexpectedly, the sudden changes in the countries’ demographic
profiles now pose as an economic and social challenge, calling for policy attention regarding its
pension distribution. Singapore faces this public concern known as the pension distribution
crisis. There are several distinct factors that continue to deter this crisis namely, the unanticipated
sudden increases in life expectancies, the continuous decline in fertility rates, and mortality rates.
All these factors which have been looked upon are now seen as a threat for economic and social
stability of workers and pensioners.
The intent of this thesis is to serve as an eye – opener. The research provides different points
concerning on the matter of pension distribution crisis. This aims to raise the level of awareness
for future social and economic policy formations which could be adaptable to one’s home
country. Thus, in the long run, one’s home country can learn from and prepare for the impacts of
pension distribution crisis.
2
TABLE OF CONTENTS
Page
1.
2.
3.
4.
5.
Title
Abstract
Table of Contents
List of Tables
List of Figures
CHAPTER 1
CHAPTER 2
CHAPTER 3
CHAPTER 4
CHAPTER 5
INTRODUCTION
Background of the Study
Key Issues / Trends
Objective of the Study
Significance of the Study
REVIEW OF RELATED LITERATURE
Pensions
Defined Benefit Scheme
Defined Contribution Scheme
Pension Distribution Crisis
Life Expectancy
Women and Fertility Rates
Medical Care and Mortality Rates
Synthesis
Simulacrum
RESEARCH METHOD
Econometric Model
Statistical Treatment
Data Gathering Procedure
RESULTS AND DISCUSSIONS
Life Expectancy
Fertility Rates
Mortality Rates
CONCLUSIONS AND RECOMMENDATIONS
Life Expectancy
Fertility Rates
Mortality Rates
BIBLIOGRAPHY
APPENDICES
ABOUT THE AUTHOR
3
6
6
6
7
7
8
8
8
8
11
12
14
15
17
19
20
20
20
22
23
23
24
24
27
27
27
28
31
36
46
List of Tables
Table 1A. Central Provident Fund (CPF) Contribution Rates and Allocation Rates
38
Table 1B. CPF Contributions Credited to each Account for each Age Bracket
38
Table 2A. CPF Members by Age Group
41
Table 2B. Active CPF Members by Age Group
41
Table 3A. Withdrawals of CPF by Type (In Million Dollars)
42
Table 3B. Withdrawals of CPF by Type (In Numbers)
42
Table 4.Total CPF Savings at Age 55 among the Elderly who were Age 59 – Above in 1999
43
Table 5. Median Age for Singapore in 1911 – 2000
44
Table 6. Medical Research in Singapore in 2006 – 2012
44
4
List of Figures
Figure 1. Simulacrum
19
Figure 2A. Life Expectancy Regression Output
39
Figure 2B. Fertility Rates Regression Output
39
Figure 2C. Mortality Rates Regression Output
40
Figure 3. Singapore’s Dependency Ratios in 1960 – 2011
43
Figure 4. Singapore’s Health Expenditure (Thousands), PPP (Constant 2005, International $) 45
5
Introduction
People all over the world are living longer than before. The progressive fall in fertility
and greater longevity are changing the structure of the world’s population (UN, 2005).
According to the World Health Organization, global life expectancy at birth, now 66 years, is
projected to reach 73 years by 2025. Many thousands of people born at the end of the 20 th
century will live throughout the 21st century. For example, France is projected to have 150,000
centenarians by the year 2050 compared to only 200 in 1950 (see The World Health Report
1998). Thus, it is imperative for the worker to retire later than the usual retirement age of 65 to
have sufficient income when retirement comes.
Better medical care aggravates longevity risk. The pressures placed on national health –
care systems by the recent demographic and epidemiological transitions are amplified by the
growing demands of an increasingly educated and affluent population for high – quality health
care and the supply of the latest medical technology. (Chongsuvivatwong, et. al, 2011).
Increase in female education induces Asians to have fewer children and to participate in
the labor force, leading to a decline in the fertility rates. For example, in Indonesia, Singapore,
South Korea, Taiwan (Province of China) and Thailand—where modern contraception has been
widely accepted, many girls are educated, and family sizes have declined dramatically—the
number of women who have moved into professional, technical, and administrative positions
have increased substantially in recent decades. The decline in fertility rates translates to fewer
young workers. Thus, financial, economic and social problems regarding adequate pension funds,
6
equitable pension distribution, and sufficient retirement income is at stake (see Labour Force
Participation and Employment under Women’s Empowerment and Reproductive Health).
Old age income support will be one of the biggest social and economic challenges facing
developing Asia (henceforth Asia) in the 21st century. In contrast to industrialized countries,
most Asian countries do not yet have mature, well functioning pension systems. As a result, they
are ill prepared to provide economic security for the large number of retirees who loom on the
horizon (Park & Estrada, 2012).
Because of the emergence of the pension distribution crisis in South – East Asia, the main
goal of this research is to show how life expectancy, female participation, and medical care can
help better reshape Singapore’s pension system by taking all these factors into account. The
researchers highlight on the principle of horizontal equity and pension wealth in terms of
pensions received and how the chosen pension scheme may affect workers. Therefore, this paper
serves to provide fresh insights by looking at the issue on a different perspective because the
significance of doing so could mean a brighter retirement scene for elderly workers and for
future workers. In connection, this paper focuses solely on Singapore.
7
Review of Related Literature
Pensions are a form of compensation deferred or delayed until the worker decides to
leave his or her job (Friedberg & Webb, 2005). The retirement decision of the worker revolves
around two things: difference on derived utilities between work and leisure – which is retirement
in this sense – and net present value between current and expected rewards and future
compensation in the form of pensions (Friedberg & Webb, 2005). How the worker receives his
or her pensions is resolved through a pension scheme. A pension scheme can be thought of as a
long - term medium wherein resources are transferred from the current young workers to retiring
ones. The two key types of funded pension schemes are known to be either a Defined Benefit or
a Defined Contribution scheme (Duval, 2003; Blake, 2000).
Defined Benefit schemes (DB scheme hereafter) are traditional. Typically, retiree
benefits from this scheme depend on the number of years of service and his or her final
occupational salary. Defined Contribution schemes (DC scheme hereafter) on the other hand are
characterized by the firm’s promise of contributing a certain amount for the worker annually
(Blake, 2000; Kapinos, 2009). As to what type of pension scheme the rational worker should
choose from is based on several factors. At the bottom line, this is where he or she can derive
stable income sources for retirement when all costs and benefits for each pension scheme have
been looked upon (Sundali, Westerman, &Stedham, 2008). These sources of income are usually
referred to as “pillars” of the pension scheme (Hogler& Hunt III, 2008).
8
Both pension schemes incur economic costs and benefits but they differ in kind. In a DB
scheme, the pension provider accumulates assets held in trust. The uncertainty it brings are the
pension fund’s investment rate of return and final occupational salary. The latter is daunting
since employers do not know the progression of its workers. Also, the promise of the DB scheme
provider can be indeterminate since final cost is not known until the worker’s retirement (Eaton
&Nofsinger, 2008). A DB scheme can provide a reasonable replacement ratio – the ratio of
annual benefits to earnings just prior to retirement (Duval, 2003; Blake, 2000) – to workers who
only opt to use the DB scheme over his or her career. Thus, frequent job changers would be
worse off since these workers would experience large portability losses. This is because
employers give different schemes when workers shift from one job to another (Friedberg &
Webb, 2005; Friedberg, Owyang, & Sinclair, 2006). As a result, these workers lose their pension
entitlement.
With DC schemes, it is important to distinguish between accumulation and decumulation
stages. Starting from the accumulation stage, a DC scheme – sometimes referred to as a personal
pension scheme – would be more ideal for the frequent job changer since the portability losses
here do not take any effect. However, following a DC scheme is often connected with higher
charges since DC schemes are frontloaded. This means that the initial charges are drawn from
the start of the scheme rather than having it dispersed evenly throughout – leading to higher
operating costs. From the decumulation stage known as annuities, DC schemes would prove to
be reliable if it were only able to provide adequate pensions in retirement. Unfortunately, this is
impeded by the cases of annuities. Annuitants and annuity providers both face several serious
problems. The major reason behind this blockage is the adverse selection bias connected to
9
mortality risk. This is the risk where workers who believe that they would live longer would
purchase annuities. Apparently, annuities markets are known to be relatively thin. Another is the
uncertainty of assumptions on mortality risks. It would be consequential for annuity providers to
update their mortality assumptions (Blake, 2000; Byrne & Winter, 2009). Furthermore, while
there is the presence of portability of jobs in the DC scheme, this is not the case between pension
scheme providers. Transfers from DB schemes to DC schemes translate to greater economic
costs. DB plan users transferring to DC plans forego the accrued benefits – the ’backloading loss’
– and incur portability loss. The marginal benefit derived from an additional year from the newly
chosen scheme (DC scheme) only equals the return of that year’s contributions (Blake, 2000).
Despite the numerous flaws of the DC scheme, much of the private – sector pension provision
still has shifted away from using the traditional DB schemes (Kiosse & Peasnell, 2009; Kapinos,
2009).
The declining popularity of DB schemes to pension providers directly stem from:
longevity risk – employees, on average, have longer life expectancies – which is the most
significant risk borne by DB schemes (Byrne & Winter, 2009) – interest rate risk – interest rates
might fall, increasing the risks associated from long – term liabilities, inflation risk – final
salaries might increase higher than predicted, and investment return risk – employer’s rate of
return from contributions to the plan are lower (Kiosse&Peasnell, 2009). Default risks are also
associated with a DB scheme due to the incidence of the adverse selection problem where
employers are likely to default on their obligations (Kiosse&Peasnell, 2009). In retrospect, the
DB schemes are ultimately linked with higher net losses than DC schemes (Banks, Blundell,
10
Emmerson, 2005) and are seen to be unsustainable during today’s economic conditions (Sundali,
Westerman, Stedham, 2008).
One prominent issue found on pension is its distribution. Specifically, it is tied to the
recurring thought of inadequate coverage. There is a widespread fear that retiring workers are not
saving enough for their future consumption and public awareness has elevated the concerns on
the adequacy of retirement savings (Kiosse&Peasnell, 2009).
The pension distribution crisis has been evident throughout the OECD countries whereby
international organizations raise concerns on the sustainability of these pensions systems. The
two principal concerns are maintaining the level of economic activities of older workers and
preserving their living standards. In other words, these organizations see the need to raise or
delay the effective retirement age of older workers and secure them from poverty during old –
age (Pestieau, 2003). However, increasing the pensionable age creates inconsistencies regarding
their reduced competitiveness in the labor market. Older workers are also more prone to health
issues. Thus, these workers could not compete as extensively as they did during their younger
years (Bredt, 2008). Transition economies are now facing the same social and economic
challenges of pension distribution. Countries coming from Asia are now left with the same crisis
– but at a greater cost. Singapore’s pension system is not tailor – fitted to the rapid changing of
demographics and economic conditions that continue to deter the already imperfect pension
schemes and its distribution (Salditt, Whiteford, &Adema 2008; Brodjonegoro&Simanjuntak,
2002).
11
The ongoing trend of increasing life expectancy of the population has been the most
popular dominant factor of pension distribution crisis. This trend of a longer life expectancy has
accelerated in a way not previously anticipated (Everness, 2001). Life expectancy risk relates to
the projected length of life of a cohort or generation while longevity risk relates to individuals.
Though the increasing life spans are seen to be wonderful and worth celebrating, it challenges
the economic and social stability of pensions systems. In line with the risks that life expectancy
bears against DB and DC schemes are the regrettable decisions which have been based on
miscalculated estimates. Most Asian countries still follow an unrealistic retirement age ranging
from 55 – 60. Many were set during the onset of world war. Perceptively during the 1950’s, life
expectancy would be much lower than today. Indeed this was the case since Asian life
expectancy was at 41 back then. However, more recent is the fact that many Asians are now
living longer – experiencing longer life expectancies – ranging from 60 – 80. This happens to be
the case for women since women live longer than their counterparts. Since women live longer
than males, they are more prone to the risk of poverty since they would accumulate fewer
resources (Dordea & Popovici, 2008). With this understanding, pension payments would be
much more expensive since retirees live longer than expected for pension providers. In DC
schemes, benefits received by the worker would be lower due to higher life expectancy. This is
because there is a longer duration for pension payments. This also verifies the asset
decumulation of the elderly (De Nardi, French, & Jones, 2009). In DB schemes, there is a fixed
amount regardless of life expectancy (Whitehouse, 2007) which causes a shift from DB schemes
to DC schemes.
12
On a different light, population ageing is occurring more rapidly in Asia than in Western
countries. Population ageing induces ‘greying’ of the working – age population. Given that these
workers have weaker labor market attachment as compared to prime – age workers, the tendency
is that old – age dependency ratios will rise which is caused by the decline in aggregate
participation levels and employment rates of these workers. Simply stated, the serious effect of
population ageing due to longer life expectancies reduces workers in the labor force (Goh, 2005).
Eventually, it all adds pressure to the current pensions systems and living standards of the
retiring workers (Duval, 2003). Population ageing is a classic demographic transition. It
increases adult longevity and thus, increases life expectancy. It becomes evident that pensions
become expensive as the number of workers for every retiree falls since pensions for these
retiring workers are taken from young workers. Raising the effective retirement age could help
alleviate the burden of ageing populations since they would be able to compensate for reduced
pensions (Ghilarducci, 2010). However, some distinct factors greatly affect the retirement
decision of the worker and thus, the supply of labor. The two major components are the strong
preference of the worker for leisure and the increased wealth effects which are associated with
rising living standards (Duval, 2003; Ghilarducci, 2010; Roberts, Rice, & Jones, 2010). Also,
work is not necessarily good for the older workers. In fact, more time for retirement could be the
cause of longer lives assuming that retirement produces healthier outcomes (Ghilarducci, 2010;
Roberts, Rice, & Jones, 2010).
𝐻0 : The increase in life expectancies in Singapore does not affect the pension distribution crisis
𝐻𝑎 : The increase in life expectancies in Singapore affects the pension distribution crisis
13
Fertility rates are defined as birth rates per female (Blake & Mayhew 2006). The
dramatic increase on population ageing due to longer life expectancies is concurrent to a
decrease in fertility rates. Thus, the replacement level of young – to – old needed for the
sustainability of old age pensions becomes problematic. Taken differently, declining birth rates
per woman results to fewer workers contributing to the pensions system; and labor force
participation of the young workers would be relatively lower (Hogler& Hunt III, 2008). Thus,
the decline in fertility rates raises the ratio of the elderly to the working age (Brooks, 2005).
There are several factors that affect the decline of total fertility rates and one of which is
the higher participation rates of women. Women were underrepresented in the labor market.
These women were mostly found in the informal sector and this displays inequality in labor
outcomes (Caceres – Delpiano, 2012). But now, more women are given brighter opportunities in
their career and changes in preferences must have increased the female participation rate too
(Euwals, Knoef, & van Vuuren, 2011). The increase of female participation in the labor market
occurs when females consider the opportunity cost of income foregone from disregarding paid
employment. Another form of opportunity cost is the career path the female worker has set for
herself. She forgoes future higher income, recognition and awards, and other benefits. These
females would put off having children when opportunity cost is relatively higher (Mishra,
Nielsen, & Smyth, 2010). The increase in female employment induces the female worker to
delay her childbearing which causes the decline in fertility rates (Caceres – Delpiano, 2012). In
addition, they have greater control over their fecundity (Cesaratto, 2006). Since more women are
now participating in the labor force, women’s role has changed.
14
As times have changed, family ties and work for women became more optional as well.
The fertility decision – in short – offers a negative impact on the increase of female participation
(Caceres – Delpiano, 2012). Moreover, the choice between the two results to a trade – off. Since
this is the case, this leads to lower levels of fertility. The introduction of family planning
contributed much to the decline as couples have used such method during the formation of their
family. The dramatic decline of fertility rates – in effect – causes demographic transitions too or
what can be referred to as a ‘demographic dividend’ (Blake & Mayhew, 2006). The impact poses
a great threat to Asia since 60% of the world’s population is Asians (Goh, 2005).
𝐻0 : The declining fertility rates in Singapore do not affect the pension distribution crisis
𝐻𝑎 : The declining fertility rates in Singapore affect the pension distribution crisis
The impact of new medical technologies (NMT’s) in Asia has increased the financial
insolvency in their healthcare systems. This is due to the insurgence of high demand for
technologically advanced medicine and medical services of the receiving population. The high
demand for medical care services and healthcare is due to the increased awareness of the benefits
of better health status (Grosskopf, Self, & Zaim, 2006; Sheiner, 2007) and creation of wider
access to health care systems (Sheiner, 2007). In addition, medical advances have contributed
much in the decline of mortality rates. There are two contradicting theories that matter on the
mortality of persons. The theory on compression of morbidity – disabilities would appear at
shorter periods before death – suggests that medical progress and healthier lifestyles cause a fall
in mortality rates (Shiu& Chiu, 2008; Espigares, Torres, & Munoz, 2008). States with lower
mortality rates lead to healthier populations (Thornton & Rice, 2008). This confirms the
15
importance of societal health which is growing than ever (Shaw, Horrace, & Vogel, 2005). The
theory on expansion of morbidity – reduction of risk associated with healthier lifestyles –
explains the zero effect of appreciable health gains to the elderly, which is also true since more
of the elderly experience old age sickness and diseases (Shiu & Chiu, 2008; Espigares, Torres, &
Munoz, 2008). The deterioration of health of the elderly means more medical costs to incur
especially for the cohort ages 65 and above as compared to lower cohorts (Thornton & Rice,
2008). As a result, the disability prevalence of these workers reacts negatively to the fall of
mortality rates (Espigares, Torres, & Munoz, 2008). This also proves to generate adverse
consequences on the funding of pension schemes since pensioners would have to pay longer.
Relatively speaking, older workers would consume more of health care than with younger
workers since they are more exposed to health problems (Shaw, Horrace, & Vogel, 2005;
Sheiner, 2007).
Many believe that health care expenditures rise along with life expectancy. However,
research has found that population ageing is not the primary factor of rising health care
expenditures. Rather, it highlights the time of death and health status of these workers which is
explained by mortality rates. In fact, most empirical evidence suggests that longevity or longer
lives of people does not necessarily entail higher health care expenditures. It is argued that
economic development is the root cause of such longer natural life spans and medical progress
(Shiu& Chiu, 2008). This simply means that there are improvements in mortality risk because of
the technological advancement in medical technology.
16
An individual has two stages in life: working period and retirement period. This is
important to note in understanding the declining mortality rates of workers. This is shown when
the certain worker chooses a health investment on the first or second stage. If health investment
was placed on the preceding stage, it is imperative to conclude that this worker would reduce his
or her probability of death and thus, improve his mortality. If the health investment of the worker
is placed on the second period, then he or she becomes less susceptible to chronic diseases since
the worker has benefited from the fruits of more efficient medical technology. These fruits are
known to be the worker’s resiliency against sickness and better health. These both contribute to
the decline of mortality risk (Zhang, Zhang & Leung, 2006).
Much of the pension providers use mortality tables to calculate scheme valuations for the
retiring workers. Mortality tables are set out on the probability of the certain worker’s death
period. These tables are based on historical data on death rates (Byrne & Winter, 2009; Espigares,
Torres, & Munoz, 2008) and unfortunately, mortality assumptions are considerably
underestimated (Blake, 2000; Byrne & Winter, 2009).
𝐻0 : The declining mortality rates in Singapore do not affect the pension distribution crisis
𝐻𝑎 : The declining mortality in Singapore affects the pension distribution crisis
In totality, the pension distribution crisis is further intensified by the differing factors of:
unexpected increases in the life expectancies of workers where many workers fear that they are
not saving enough for retirement. The continuing decline of fertility rates due to the increased
participation rate of women in the labor force since there would be less of resources to pass on to
17
retiring workers since there would be relatively fewer marginal additions to the working – age
population. The declining mortality rates of workers make people less susceptible to chronic
diseases because of the innovation of medical technology due to its high demand. Apparently,
these workers fear of old age poverty considering too of longer pension payments and high
medical costs.
This is known to be the cases of OECD and other developed countries in the world where
pensions systems are known to be inadequate in coverage. Hence, the researchers came to test if
this is also true for Singapore that happens to find difficulties in their pension distribution.
18
Simulacrum – Figure 1.
Life Expectancy
(+)
Fertility Rates
(-)
Pension Distribution
Crisis
(-)
Mortality Rates
19
Research Method
Censored Normal Regression (Tobit) Model: Maximum Likelihood Method
𝒀∗ ,
𝒀𝒊 = { 𝒊
𝟎,
𝒊𝒇 𝒀∗𝒊 > 𝟎
𝒊𝒇 𝒀∗𝒊 ≤ 𝟎
𝒀∗𝒊 = 𝛂 + 𝜸′ 𝑳𝒊𝒇𝒆𝑬𝒙𝒑𝒆𝒄𝒕𝒂𝒏𝒄𝒚𝒊𝒕 + 𝒆𝒊𝒕
𝒀∗𝒊 = 𝛂 + 𝜸′ 𝑴𝒐𝒓𝒕𝒂𝒍𝒊𝒕𝒚𝑹𝒂𝒕𝒆𝒊𝒕 + 𝒆𝒊𝒕
𝒀∗𝒊 = 𝛂 + 𝜸′ 𝑭𝒆𝒓𝒕𝒊𝒍𝒊𝒕𝒚𝑹𝒂𝒕𝒆𝒊𝒕 + 𝒆𝒊𝒕
Where:
𝒀∗𝒊 = Required sufficient amount of pensions (in constant LCU)
𝛾 ′ 𝑥 = Vector of regression coefficients on independent variables, x
i = ith country observation
t = tth time observation
Econometric Model:
In this model, the variable of interest, 𝒀∗𝒊 is left – censored at zero. Left – censoring
indicates that all values that fall below or from the left of 0 will be cut – off. When the latent
variable takes up the value of 0, it is therefore, left - censored while values taking up 1 are still
observed and therefore, are uncensored.
Binary values (0, 1) represent our latent variable. Thus, 𝛾 = max(0|𝑦 ∗ ). These values
have been used as an indicator wherein 1 = Pension Distribution Crisis or 0 otherwise
20
(See Appendix I; pp.29-30). The required sufficient amount of pensions (in constant
LCU) is solved through the use of Singapore’s current pension structure. In order to
properly determine whether pensions accrued for future consumption is sufficient;
retirement income must equal or go beyond Singapore’s living standards (See Appendix
I; pp.29-30). This makes life more promising for the retiree in financial and social
security terms. Pension computations were patterned to Singapore’s current pension
system as reference for the binary values (See Appendix I; pp.29-30). Therefore, if
pensions computed fall below the required amount for sufficient retirement income, then
it will take up the value of 1 as this indicates that pensions received by current and future
retirees is and will experience pension distribution crisis. If pensions computed exceed
the required amount for sufficient retirement income, then it states otherwise. Thus,
pensions are compared to Singapore’s GDP per capita or prices (constant, LCU) of
Singapore’s living standards. This is a useful indicator of standard of living or quality of
life. Its significance is deemed necessary to understand how the current pension structure
becomes obsolete and thus, creates an air of old age financial insecurity.
Life Expectancy is defined as expected number of years of life of the worker which
quantifies for Life Expectancy. Fertility rate is defined as birth per woman during her
reproductive years which quantifies for Female Participation Rate. Mortality rate is defined as
incidence of death in a population which quantifies for Medical Care.
Maximum Likelihood (ML) is more appropriate since OLS estimates can cause bias in
interpretation and can provide inconsistent estimates of the parameters. The time – series, t, and
21
cross section data, 𝑖, were gathered from year 1960 – 2011 for Singapore – where pension
distribution crisis is arguably evident and troubling. The data were taken from IndexMundi, and
Social Security Association: Office of Retirement and Disability Policy of the United States.
In order to simplify the process of determining pensions, several basic assumptions must
be formulated:
a.) the retiree is eligible and entitled to receive pensions
-
This means the pensioner for Singapore has passed all qualifications necessary for
pension entitlement and eligibility
b.) Pensioner has started accumulating resources at the age of 35 years old up to the
retirement age of 55 years old. 35 years old is the youngest age necessary for
eligibility and pension entitlement. 55 years old is the retirement age mandated by
each of the country’s social security laws
-
This information is useful in pension computations for Singapore’s Defined
Contribution scheme
22
Results and Discussions
Singapore uses 3 types of accounts: Ordinary Accounts, Special Accounts, and Medisave
Accounts. Ordinary Accounts can be used for housing and investment schemes, Medisave
Accounts can be used for hospitalization expenses and catastrophic health insurance while the
Special Accounts can be used solely on retirement and other purposes. The pensioners can
choose among the 3 types depending on their preferred contribution rate or where their pensions
are credited to based solely on the pensioner’s level of preference (See Appendix II: Table1A;
p.31). Thus, the final pensions accrued do not depend on whether it should be under an Ordinary,
Special, or Medisave account. It simply states that under any of the 3 accounts, there is a certain
credit rate from the estimated contributions for each age bracket.
I.
Ordinary Accounts, Special Accounts, and Medisave Accounts
Pensioners who have invested in an Ordinary Account, Special Account, and Medisave
Account are all collectively reflected in the regression outputs (See Appendix III: Fig.2A,
Fig.2B, & Fig.2C; pp.32-33). Tobit coefficients are all statistically significant at 5%.
Analysis and Interpretation
Life Expectancy
Life expectancy positively affects our latent variable, which is the required sufficient
amount of pensions (in constant LCU) that will cover the pensioners from financial insecurity. In
the case of Singapore, for every 1 year increase in the life expectancy of a Singaporean pensioner
who invests in any of the 3 accounts, there is a corresponding 0.267030 Singaporean dollar
23
increase required to sufficiently cover the pensioners’ future. The intercept, on the other hand, negatively affects our latent variable. This is the case when the regressor, LE, is equated to zero.
With this, there is no need for an increase of -20.40154 Singaporean dollars. Simply stated, when
a Singaporean is not expected to live (LE = 0), then there is no needed requirement of an
additional -20.40154 Singaporean dollars.
Cohort differences in the CPF coverage are important. Table 2A (Appendix IV; p.34)
clearly depicts that during 2012; 30% of the age bracket 56 – above are actually covered by the
CPF as compared to 18% of the age bracket 31 – 40. However, this is not truly the case because
the active CPF members depicted in Table 2B (Appendix IV; p.34) clearly shows that only 18%
of the age brackets 56 – 60 and 60 – above are truly covered and are actively contributing against
26% of the age bracket 31 – 40. In connection to CPF savings shown in table 4 (Appendix IV;
p.36), 30.7% of the elderly has accumulated less than the ordinary wage ceiling of S$5,000 while
24.9% have none at all (See Appendix IV: Table 4; p.36). Because of low coverage rates among
the elderly, this will result to low reliability on the CPF savings overtime.
Fertility Rates and Mortality Rates
Fertility rates and Mortality rates negatively affect our latent variable, which is the
required sufficient amount of pensions (in constant LCU) that will cover the pensioners from
financial insecurity. In the case of a Singaporean pensioner who invests in any of the 3 accounts,
for every 1 increase in birth per woman and 1 increase in incidence of death, a -4.815733 and 1.634027 Singaporean dollar is not needed respectively (See Appendix III: Fig.2B, & Fig.2C;
pp.32-33). The intercepts of Fertility Rates and Mortality Rates, on the other hand, both
positively affect our latent variable. This is the case when the regressors, LOG(FR) and
24
LOG(MR), are both equated to zero. With this, there is a need for an increase of 2.158468 and
2.411387 Singaporean dollars respectively. Simply stated, when there are no births per female
during her reproductive years(LOG(FR) = 0) and no incidence of death (LOG(MR) = 0) in
Singapore, then there is a needed requirement of an additional 2.158468 and 2.411387
Singaporean dollars respectively.
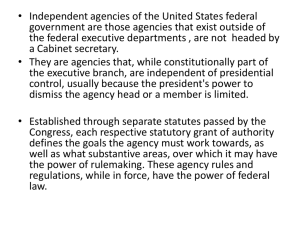
Because of low replacement levels due to a decline in the fertility rates, the continuous
decline exacerbates the ratio of the elderly to the working age. This is depicted in figure 3 (See
Appendix IV; p.36) where the increasing old age dependency ratio also leads to the decreasing
support ratio as well. Since less of workers are entering the labor force, then there are less of
workers contributing to the pension systems. A smaller resource base unfortunately, makes
pensions relatively more expensive. This can also be portrayed in table 5 (Appendix IV; p.37)
where the total median age in Singapore has risen and is projected to further increase until 2030.
Because of this, Singapore will continue to experience a demographic dividend.
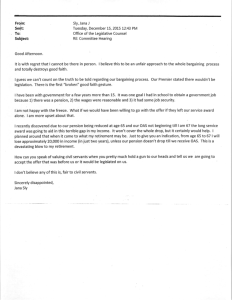
Singaporeans continue to put emphasis on better health status that leads to a growing
demand for new medical technologies (NMT’s) and its continuous innovation shown in table 6
(Appendix IV; p.37). Because of this thinking, pensioners face to live a life full of old age
disease and sickness (theory on expansion of morbidity) or an extended healthier life (theory on
compression of morbidity). Figure 4 (Appendix IV; p.38) also shows Singapore’s rising total
health expenditure. In addition, Singapore’s healthcare systems place the responsibility of
ensuring better health on the pensioner through the Medisave account (if chosen). This is also
known as the national medical savings scheme where 80% of primary care is delivered by
private practitioners while the remaining 20% is provided by public polyclinics. However,
25
hospital care is mainly delivered by public hospitals (80%) while the remaining 20% is delivered
by private hospitals.
26
V. Conclusions and Recommendations
A step forward for the Singaporean pension system is to analyze the labor market
attachment of their workers. This can provide one solution to address its inadequate pension
coverage. If Singaporean workers tend to keep their jobs up until their retirement then it would
be best to use a Defined Benefit scheme since pensioners would accumulate more of resources. If
Singaporean workers tend to shift from one job to another (job portability), then it would be wise
to use a Defined Contribution scheme since job portability losses here do not take any effect.
The Singaporean government needs to address the longevity risk associated with
retirement. Apparently, there is less emphasis on how rapid Singaporeans spend their
accumulated balances. There is significance in knowing since if the pensioner has too few of
resources due to longer life then there is a need to address the income received especially by the
older workers. On average, women live longer than men yet they experience lower exposure in
the labor market and receive relatively lower income as well. In this case, gender equality plays a
huge part. This policy relates to delaying the formal effective retirement age from 55 – 65 years
old. With this, formal discussions will arise between the employer and employee regarding the
terms and conditions on work and employment. Because there would be more of elderly workers,
workplace arrangements and services should then be conducive for them as well. Social risk
pooling arrangements is one way for Singapore’s pension structure to cover all pensioners from
different socio – economic and demographic classes. This means creating public pension systems
that is available for Singaporeans of different walks in life.
In order to induce female workers not to delay their childbearing in the short run, it is
imperative for Singapore to provide family – friendly services and workplace environments
27
through financial incentives. This means that workplace policies and other discussions that may
arise between the employer and the female worker relating to this matter should be formally
given attention to. In order for female workers to be further encouraged in childbearing in the
short run, daycare centers, childcare centers, and other infant and children – based services
should be considered. Since childcare centers are privately – run, these centers become
expensive and thus, add up to their cost of living. In order to help ease the financial burden, the
government may subsidize for a certain period of time as well under licensed infant care and
childcare centers.
Since Singaporeans do place a huge value on staying healthy and having healthier
lifestyles, unfortunately and even so, healthcare systems are actually relatively more expensive to
the elderly as compared to younger workers. This is the case since the elderly consume more of
these goods than the younger population. There is an increase in the use of Medisave Accounts
and other elderly – based schemes like ElderShield Accounts. However, not much attention is
given to these since most of the pensioners choose the Ordinary Accounts where housing and
investment schemes take place (See Appendix, Tables 3A & 3B; p.35). Therefore, our 1st policy
will focus on expanding medical services in order for ‘medical accounts’ to be more competitive
in nature. The Singaporean government should issue more licenses to approved institutions or
qualified institutions of medical services and the like to make healthcare systems more
affordable and more redistributive to all Singaporeans. At the same time, the Singaporean
government should continue to fund medical research in order to combat popular and deadly old
age diseases. In this case, top old age diseases will be shouldered under Medisave accounts and
similar accounts. This will meet the demand of the elderly who are experiencing old age diseases
who are users of Medisave accounts. The 2nd policy will focus on the estimated actuaries where
28
annuitants buy life annuities. This is needed in order to reduce the adverse selection bias
connected to mortality rates. The Singaporean government should also consider the mortality
rates between a male and a female since there are certain health risks and lifestyles that are
distinctive between the two categories.
29
References
Population Division of the Department of Economic and Social Affairs of the UN Secretariat.
World population prospects: the 2005 revision highlights. Retrieved July 2012, from
http://www.un.org/esa/population/publications/wpp2005/ wpp2008_highlights.pdf
World Health Organization. The World Health Report 1998. Retrieved July 2012, from
http://www.who.int/inf-pr-1998/en/pr98-WHA4.html.
Chongsuvivatwong, et. al. (n.d.). Health and Healthcare Systems in Southeast Asia. United
Nations University. Retrieved July 2012, from http://unu.edu/publications/articles/health-andhealthcare-systems-in-southeast-asia.html.
Women’s Empowerment & Reproductive Health. Labour Force Participation & Employment.
Retrieved July 2012, from http://web.unfpa.org/intercenter/cycle/labour.htm.
Park, D. & Estrada, G. (2012). Pension Systems and Old-Age Income Support in East and Southeast Asia.
Overview and Reform Directions. Routledge publisher.
30
Bibliography
Banks, J., Blundell, R., &Emmerson, C. (2005). The Balance Between Defined Benefit, Defined
Contribution, and State Provision. Journal Of The European Economic Association, 3(2/3), 466476.
Bardasi, E., & Jenkins, S. P. (2010).The Gender Gap in Private Pension. Bulletin Of Economic
Research, 62(4), 343-363.
Blake, D. (2000). Does It Matter What Type of Pension Scheme You Have? Economic
Journal, 110(461), F46-F81.
Blake, D., & Mayhew, L. (2006).On The Sustainability of the UK State Pension System in the
Light of Population Ageing and Declining Fertility.Economic Journal, 116(512), F286-F305.
Bongaarts, John. (2004). Populations Aging and the Rising Cost of Public Pensions.Population
and Development Review, Vol. 30, (No. 1), pp. 1-23.
Bong-Min, Y. (2009).The Future of Health Technology Assessment in Healthcare Decision
Making in Asia. Pharmacoeconomics, 27(11), 891-901.
Bredt, S. (2008). Between labour market and retirement pension — flexible transition as a new
paradigm for ageing societies?. International Social Security Review, 61(4), 95-112.
Brodjonegoro, Bambang; Simanjuntak, Robert. (2002). Pension Plan in Indonesia: Avenues for
Reform. HitotsubashiJournal of Economics, 43(2): pp. 151-162.
Brooks, Sarah M. (2005). Interdependent and Domestic Foundations of Policy Change: The
Diffusion of Pension Privatization around the World. International Studies Quarterly, Vol.
49(No. 2), pp. 273-294.
Brugiavini, A., Maser, K., & Sudén, A. (2005). Measuring Pension Wealth. Journal of Pension
Measurement.
Byrne, A., &Winter, N. (2009). Living with longevity. Pensions: An International Journal, 14(2),
115-127.
Cáceres-Delpiano, J. (2012). Can We Still Learn Something From the Relationship Between
Fertility and Mother's Employment? Evidence From Developing Countries. Demography, 49(1),
151-174.
Cebula, R., & Coombs, C. (2008).Recent Evidence on Factors Influencing the Female Labor
Force Participation Rate. Journal Of Labor Research,29(3), 272-284.
31
Cesaratto, S. (2006). Pensions in an ageing society: a symposium. Review Of Political
Economy, 18(3), 295-299.
Cohen, C. (1983). The Impact on Women of Proposed Changes in the Private Pension System: A
Simulation. Industrial & Labor Relations Review, 36(2), 258-270.
Creedy, J., &Scobie, G. M. (2005).Population Ageing and Social Expenditure in New
Zealand. Australian Economic Review, 38(1), 19-39.
De Nardi, M., French, E., & Jones, J. (2009).Life Expectancy and Old Age Savings. American
Economic Review, 99(2), 110-115.
Dordea, S. & Popovici, V. (2008). The Different Impact of Pension Reform on Women and Men.
Awards Of the Oradea, Economic Science Series, 17(1), 294-287.
Duval, Romain.(2003). The Retirement Effects of Old-age Pension and Early Retirement
Schemes and OECD Countries. OECD Economic Studies, Vol. 2003 (No. 2), p7-50.
Eaton, T. V., &Nofsinger, J. R. (2008).Funding Levels and Gender in Public Pension
Plans. Public Budgeting & Finance, 28(3), 108-128.
Engelhardt, G. V. (2002). Pre-Retirement Lump-Sum Pension Distributions and Retirement
Income Security: Evidence from the Health and Retirement Study. National Tax Journal, 55(4),
665-685.
Espigares, J., Torres, E., & Muñoz, T. (2008).Population Ageing, Dependency and Healthcare
Services Utilisation. Estudios De EconomíaAplicada, 26(2), 1-30.
Euwals, R., Knoef, M., & van Vuuren, D. (2011). The trend in female labour force participation:
what can be expected for the future?.Empirical Economics, 40(3), 729-753.
Even, W. E., & MacPherson, D. A. (1994).Gender Differences in Pensions. Journal Of Human
Resources, 29(2), 555-587.
Everness, G. (2001). The Effect on Pensions of Increasing Life Expectancy. Journal Of Pensions
Management, 7(2), 178.
Frericks, P. H., & Maier, R. M. (2008). Pension norms and pension reforms in Europe - the
effects on gender pension gaps. Community, Work & Family, 11(3), 253-271.
Frericks, P., Knijn, T., & Maier, R. (2009).Pension Reforms, Working Patterns and Gender
Pension Gaps in Europe. Gender, Work & Organization, 16(6), 710-730.
Friedberg, L., & Webb, A. (2005).Retirement and the Evolution of Pension Structure. Journal Of
Human Resources, 40(2), 281-308.
32
Friedberg, L., Owyang, M. T., & Sinclair, T. M. (2006).Searching For Better Prospects:
Endogenizing Falling Job Tenure and Private Pension Coverage. B.E. Journal Of Economic
Analysis & Policy: Topics In Economic Analysis & Policy, 6(1), 1-40.
Ghilarducci, T. (2010).The future of retirement in aging societies.International Review Of
Applied Economics, 24(3), 319-331.
Goh, Victor HH. (2005). Aging in Asia: A cultural, socio-economical and historical perspective.
Department of Obstetrics and Gynaecology, National University of Singapore, National
University Hospital, Singapore, Vol. 8, No. 2 , Pages 90-96.
Grosskopf  , S. S., Self  , S. S., &Zaim, O. O. (2006). Estimating the
efficiency of the system of healthcare financing in achieving better health. Applied
Economics, 38(13), 1477-1488.
Guralnik, J. M., Alecxih, L., Branch, L. G., & Wiener, J. M. (2002). Medical and Long-Term
Care Costs When Older Persons Become More Dependent. American Journal Of Public
Health, 92(8), 1244-1245.
Gyu-Jin, H. (2007). The Rules of the Game: The Politics of National Pensions in Korea. Social
Policy & Administration, 41(2), 132-147.
Hashimoto, K., &Tabata, K. (2010).Population aging, health care, and growth. Journal Of
Population Economics, 23(2), 571-593.
Higuchi, T. (1977).Pensions in the Japanese rural sector. International Labour Review, 116(3),
315.
Hogler, R. L., & Hunt III, H. (2008). Pension Reform in the United States: Lessons from the
Italian Experience. Labor Law Journal,59(1), 26-39.
Jean, S., Causa, O., Jiménez, M., &Wanner, I. (2010).Migration and Labour Market Outcomes in
OECD Countries. OECD Journal: Economic Studies, 2010(1), 235-268.
Johnson, J. M., & Williamson, J. B. (2006). Do universal non-contributory old-age pensions
make sense for rural areas in low-income countries?International Social Security Review, 59(4),
47-65.
Kapinos, K. (2009). On the Determinants of Defined Benefit Pension Plan Conversions. Journal
Of Labor Research, 30(2), 149-167.
Kaur, A. (2010). Labour migration in Southeast Asia: Migration Policies, LabourExploitation
and Regulation. Journal Of The Asia Pacific Economy,15(1), 6-19.
Kemnitz, A. (2003). Immigration, Unemployment and Pensions.Scandinavian Journal Of
Economics, 105(1), 31-48.
33
Kemnitz, A. (2005). Discrimination and Resistance to Low-skilled Immigration. LABOUR:
Review Of Labour Economics & Industrial Relations,19(2), 177-190.
Kiosse, P., &Peasnell, K. (2009). Have changes in pension accounting changed pension
provision? A review of the evidence. Accounting & Business Research (Wolters Kluwer
UK), 39(3), 255-267.
Krieger, T. (2004). Fertility rates and skill distribution in Razin and Sadka’s migration-pension
model: A note. Journal Of Population Economics,17(1), 177-182.
Krieger, T. (2008). Public pensions and return migration. Public Choice,134(3/4), 163-178.
Lacomba, J. A., & Lagos, F. (2010).Immigration and Pension Benefits in the Host
Country. Economica, 77(306), 283-295.
Lagos, F., &Lacomba, J. (2005). The Role of Immigration in the Retirement Age Reform : A
Theoretical Analysis. B.E. Journal Of Economic Analysis & Policy: Topics In Economic
Analysis & Policy, 5(1), 1-20.
Malhotra, N., & Witt, M. (2010). Determinants Of Financial And Retirement Planning: A
Female Perspective. Journal Of Business & Economics Research, 8(6), 40-46.
McKinnon, R. (2007). Dynamic social security: A framework for directing change and extending
coverage. International Social Security Review,60(2/3), 149-168.
Mishra, V., Nielsen, I., & Smyth, R. (2010). On the relationship between Female Labour Force
Participation and Fertility in G7 Countries: Evidence from Panel Cointegration and Granger
causality. Empirical Economics,38(2), 361-372.
Mohan, R., &Mirmirani, S. (2008). An Assessment of OECD Health Care System Using Panel
Data Analysis. Southwest Business & Economics Journal, 1621-35.
Pestieau, P. (2003). Ageing, retirement and pension reforms. World Economy, 26(10), 1447-1457.
Philip, L. J., & Gilbert, A. (2007). Low Income amongst the Older Population in Great Britain: A
Rural/Non-rural Perspective on Income Levels and Dynamics. Regional Studies, 41(6), 735-746.
Rammohan, A. (2004). Fertility Transition in South and Southeast Asia.ASEAN Economic
Bulletin, 21(2), 183-197.
Roberts, J., Rice, N., & Jones, A. (2010). Early Retirement Among Men in Britain and Germany:
How Important is Health? Geneva Papers On Risk & Insurance - Issues & Practice, 35(4), 644667.
34
Salditt, F., Whiteford, P., &Adema, W. (2008).Pension reform in China.International Social
Security Review, 61(3), 47-71.
Serrano, F., Eguia, B., &Ferreiro, J. (2011). Public pensions' sustainability and population
ageing: Is immigration the solution?InternationalLabour Review, 150(1/2), 63-79.
Shaw, J. W., Horrace, W. C., & Vogel, R. J. (2005). The Determinants of Life Expectancy: An
Analysis of the OECD Health Data. Southern Economic Journal, 71(4), 768-783.
Sheiner, L. (2007). The Effects of Technology on the Age Distribution of Health Spending: A
Cross-Country Perspective. Public Finance & Management, 7(1), 44-72.
Shih-Jiunn, S. (2006). Left to Market and Family – Again? Ideas and the Development of the
Rural Pension Policy in China. Social Policy & Administration, 40(7), 791-806.
Shiu, Y., & Chiu, M. (2008).Re-estimating the Demographic Impact on Health Care
Expenditure: Evidence from Taiwan. Geneva Papers On Risk & Insurance - Issues &
Practice, 33(4), 728-743.
Simona-Luize, D., & Veronica, P. (2008).The Different Impact of Pension Reform on Women
and Men. Annals Of The University Of Oradea, Economic Science Series, 17(1), 284-287.
Sundali, J., Westerman, J. W., &Stedham, Y. (2008). The Importance of Stable Income Sources
in Retirement: An Exploratory Study. Journal Of Behavioral & Applied Management, 10(1), 1846.
Thornton, J. A., & Rice, J. L. (2008). Determinants of healthcare spending: a state level
analysis. Applied Economics, 40(22), 2873-2889.
Whitehouse, E. (2007). Life Expectancy Risk and Pensions: Who Bears the Burden? OECD
Papers, 7(10), 1-45.
Zhang, J., Zhang, J., & Leung, M. M. (2006).Health investment, saving, and public
policy. Canadian Journal Of Economics, 39(1), 68-93.
35
Appendix I
Tables of Statistical Figures, Regression Outputs, and Graphs
Singapore
Data Summary
Year
1960
1961
1962
1963
1964
1965
1966
1967
1968
1969
1970
1971
1972
1973
1974
1975
1976
1977
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
Life
Fertility
Expectancy Rate, Total
65.66
5.45
66.09
5.26
66.43
5.20
66.70
5.01
66.91
4.85
67.09
4.70
67.26
4.50
67.45
3.95
67.67
3.56
67.95
3.25
68.28
3.09
68.66
3.04
69.07
3.05
69.48
2.80
69.89
2.36
70.27
2.08
70.62
2.11
70.93
1.82
71.21
1.76
71.45
1.79
71.68
1.74
71.91
1.72
72.16
1.71
72.45
1.61
72.78
1.62
73.16
1.61
73.60
1.43
74.07
1.62
74.57
1.96
75.08
1.75
75.58
1.87
76.05
1.77
76.48
1.76
76.86
1.78
76.30
1.75
76.40
1.71
Mortality
Rate, Infant
35.60
33.60
31.80
30.20
28.80
27.50
26.30
25.10
24.00
22.90
21.70
20.30
18.70
17.20
15.90
14.70
13.90
13.10
12.40
11.90
11.50
11.00
10.50
9.90
9.30
8.80
8.30
7.80
7.30
6.70
6.10
5.50
5.00
4.60
4.30
4.10
36
GDP per Capita,
constant, LCU
3,881
4,272
4,153
4,410
4,321
4,797
5,189
5,696
6,361
7,122
7,979
8,779
9,784
10,667
11,170
11,517
12,208
12,938
13,888
15,001
16,304
17,204
17,646
18,915
20,200
20,039
20,320
22,168
24,008
25,697
27,216
28,167
29,256
31,799
34,077
35,463
Accounts
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
Pensions
848.13
1,848.13
2,848.13
3,848.13
4,848.13
5,848.13
6,848.13
7,848.13
8,848.13
9,848.13
10,848.13
11,848.13
12,848.13
13,848.13
14,848.13
15,848.13
16,848.13
17,848.13
18,848.13
19,848.13
20,848.13
21,848.13
22,848.13
23,848.13
24,848.13
25,848.13
26,848.13
27,848.13
28,848.13
29,848.13
30,848.13
31,848.13
32,848.13
33,848.13
34,848.13
35,848.13
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
76.75
77.05
77.40
77.55
78.05
78.35
78.70
79.04
79.49
79.99
80.14
80.44
80.79
81.24
81.64
81.89
1.70
1.64
1.49
1.48
1.60
1.41
1.37
1.27
1.26
1.26
1.28
1.29
1.28
1.22
1.15
1.20
3.80
3.60
3.40
3.10
2.90
2.70
2.60
2.40
2.40
2.30
2.30
2.20
2.20
2.10
2.10
2.00
Source: IndexMundi
37
36,647
38,452
36,361
38,307
41,053
39,500
40,785
43,287
46,664
48,939
51,588
53,866
51,943
49,906
56,269
57,801
0
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
36,848.13
37,848.13
38,848.13
39,848.13
40,848.13
41,848.13
42,848.13
43,848.13
44,848.13
45,848.13
46,848.13
47,848.13
48,848.13
49,848.13
50,848.13
51,848.13
Appendix II
Singapore’s Defined Contribution Scheme Valuation
Table 1A. Central Provident Fund (CPF) Contribution Rates and Allocation Rates
Employee
Age (Years)
Contribution Rate
(Ordinary wage ceiling: S$5,000)
Total
Employer
Employee
(% of wage) (% of wage) Contribution
35 – below
36 – 45
46 – 50
51 – 55
55 – 60
60 – 65
65 – above
16
16
16
14
10.5
7
6.5
20
20
20
18.5
13
7.5
5
Credited to
(% of wage)
Ordinary
Account
(% of wage)
Special
Account
(% of wage)
Medisave
Account
(% of wage)
36
36
36
32.5
23.5
14.5
11.5
23
21
19
13.5
12
3.5
1
6
7
8
9.5
2
1.5
1
7
8
9
9.5
9.5
9.5
9.5
Sources: Social Security Association: Office of Retirement and Disability Policy of the United States;
mycpf.cpf.gov.sg
Equation: (employee – employer contribution in current year) x (no. of years contributing) x (adjustment
factor)*
*adjustment factor: assumed rate of return on the contributions and also adjusts for the growth in
contributions over the years contributing
Given:
Ordinary Wage Ceiling: S$5,000
Adjustment Factor: 2.5%
0 = No PDC 1 = PDC where;
Total Contributions > GDP per Capita = 0; Total Contributions < GDP = 1
Table 1B. CPF Contributions Credited to each Account for each Age Bracket
Employee Age
(Years)
35 – below
Total
Contributions per
Age Bracket (S$)
1,845
36 – 45
18,450
46 – 50
9,225
51 – 55
8,328.125
Total
37,848.125
Ordinary
Account (S$)
Special Account
(S$)
Medisave
Account (S$)
1,178.75
(23% / 36%)
10,762.5
(21% / 36%)
4,868.75
(19% / 36%)
3,459.375
(13.5% / 32.5%)
307.5
(6% / 36%)
3,587.5
(7% / 36%)
2,050
(8% / 36%)
2,434.375
(9.5% / 32.5%)
358.75
(7% / 36%)
4,100
(8% / 36%)
2,306.25
(9% / 36%)
2,434.375
(9.5% / 32.5%)
Sources: Social Security Association: Office of Retirement and Disability Policy of the United States;
mycpf.cpf.gov.sg
38
Appendix III
Regression Outputs
Figure 2A.Life Expectancy
Figure 2B.Fertility Rates: log(fr)
39
Figure 2C. Mortality Rates: log(mr)
40
Appendix IV
Life Expectancy, Fertility Rates, and Mortality Rates Tables and Figures
Table 2A. Central Provident Fund (CPF) Members by Age Group
Age Group
(Years)
Total
Thousand
2006
2007
2008
2009
2010
2011
2012
3,099.6
3,163.0
3,234.4
3,291.3
3,343.3
3,376.3
3,418.6
20 – below
21 - 25
26 – 30
31 – 35
94.5
197.2
249.8
303.5
105.5
198.0
256.5
299.8
104.5
210.3
265.3
299.4
101.3
214.8
271.4
303.4
106.0
220.5
267.8
305.1
110.4
229.4
257.6
301.8
112.8
236.6
252.6
303.7
36 – 40
41 – 45
46 – 50
336.2
416.7
410.6
334.2
404.7
417.9
336.6
389.8
425.0
340.0
372.5
428.2
335.6
359.4
425.7
333.9
349.6
419.6
326.8
346.6
407.3
51 – 55
56 – above
Not
Specified
336.8
727.5
26.8
349.2
770.9
26.3
359.6
818.1
25.8
369.5
864.8
25.4
379.3
919.0
24.8
384.9
965.2
24.1
390.5
1,018.1
23.7
*Includes self – employed persons who had made CPF contributions
Source: Social Security Association: Office of Retirement and Disability Policy of the United States;
mycpf.cpf.gov.sg
Table 2B. Active CPF Members by Age Group
Age Group
(Years)
Thousand
2006
2007
2008
2009
2010
2011
2012
1,461.9
38.9
107.1
193.2
217.6
1,545.0
44.0
108.2
200.9
220.0
1,610.1
40.5
110.3
207.8
222.8
1,644.6
38.9
109.7
211.7
227.5
1,700.4
43.9
115.5
209.3
231.1
1,735.4
42.5
118.6
202.2
229.4
1,788.8
45.7
122.4
199.8
232.2
36 – 40
41 – 45
46 – 50
203.1
201.0
183.0
213.3
206.7
191.6
222.4
209.0
198.0
229.3
208.0
201.8
232.0
210.6
206.9
234.3
214.0
210.4
233.2
220.9
212.6
51 – 55
56 – 60
60 – above
Not
Specified
144.0
95.4
78.7
-
157.3
105.9
97.0
-
168.1
116.1
115.0
-
174.2
122.3
121.3
-
182.7
132.0
136.2
-
188.1
142.6
153.3
-
194.4
153.9
173.5
-
Total
20 – below
21 - 25
26 – 30
31 – 35
Source: Social Security Association: Office of Retirement and Disability Policy of the United States;
mycpf.cpf.gov.sg
41
Table 3A. Withdrawals of Central Provident Fund by Type
Withdrawals of Central Provident Fund by Type
2007
2008
2009
2010
Million Dollars
14,351
11,562
10,966
10,719
9,617
2006
2011
10,437
Tota𝐥𝟏
Housing Scheme𝒔𝟏
4,957
4,679
4,500
4,058
4,007
5,464
Public Housing
3,398
1,189
1,347
1,769
846
1,347
Residential
Properties
2,357
2,404
2,061
1,800
1,771
1,940
Reached 55 Years of
Ag𝐞𝟐
391
436
443
455
506
Leaving Singapore & 367
Malaysia
Permanentl𝐲 𝟑
284
269
286
359
378
435
Death
445
517
558
601
678
722
Medisave Scheme
136
173
195
234
286
336
Private Medical
Scheme
2,406
1,940
1,583
1,446
1,196
-312
Others
Source: Social Security Association: Office of Retirement and Disability Policy of the United States;
mycpf.cpf.gov.sg
2012
11,727
5,703
2,291
2,048
542
488
767
385
-497
Table 3B. Withdrawals of Central Provident Fund by Type (Numbers)
Housing Scheme𝐬 𝟓
Public Housin𝐠 𝟒
Residential
Properties
Reached 55 Years
of Ag𝐞𝟐
Leaving Singapore
& Malaysia
Permanentl𝐲 𝟑
Death
Withdrawals of Central Provident Fund by Type
2006
2007
2008
2009
2010
Number
2011
2012
12,904
40,576
11,059
48,512
15,016
32,355
15,349
47,222
14,154
49,617
37,608
43,560
46,690
46,789
274,246 204,808
189,610
199,552
207,868
227,540
245,645
10,479
10,848
11,130
12,255
13,454
14,619
15,038
23,358
17,075
17,258
19,802
18,544
19,869
18,472
Source: Social Security Association: Office of Retirement and Disability Policy of the United States;
mycpf.cpf.gov.sg
Notes:
1 – Refers to net amount withdrawn (gross amount withdrawn less amount refunded) by members in the
year
2 – Includes first and subsequent withdrawals
3 – Includes Malaysians leaving Singapore permanently
4 – Includes withdrawals by persons who are physically / mentally incapacitated and under the various
CPF schemes – Minimum Sum, Medishield, Home Protection, Dependants’ Protection, Education, Non –
Residential Properties, Investment, Delgro Shares (ceased Feb 04), Special Discounted Shares and
Eldershield Scheme
42
5 – Refers only to members who joined the scheme this year
6 – Data refer only to the increase in membership size for the year
Table 4. Total CPF Savings at Age 55 among the Elderly who were Age 59 and above in
1999
Total CPF Savings (S$)
4,999 – below
5,000 – 9,999
10,000 – 19,999
20,000 – 29,999
30,000 – 39,999
40,000 – 49,999
50,000 – 99,999
100,000 – 149,999
150,000 – above
None
Total
Percent
30.7
7.8
12.0
5.6
4.7
3.2
6.1
2.7
2.4
24.9
100.0
Source: 1999 Transitions in Health, Wealth, & Welfare of Elderly Singaporeans: 1995 – 1999;
mycpf.cpf.gov.sg
Figure 3. Singapore’s Dependency Ratios
Singapore Dependency Ratios: 1960 - 2011
100
90
80
70
60
50
Support Ratio
40
Old - Age Dependency Ratio
30
20
10
1960
1962
1964
1966
1968
1970
1972
1974
1976
1978
1980
1982
1984
1986
1988
1990
1992
1994
1996
1998
2000
2002
2004
2006
2008
2010
0
Source: IndexMundi
43
Table 5. Median Age for Singapore (1911 – 2000)
Census Year
1911
1921
1931
1947
1957
1970
1980
1990
2000
2010
2020
2030
Median Age
28
28
26
23
19
20
24
29
34
37
39
41
Source: Singapore Census Population 2000 and the Inter – Ministerial Committee Report on Ageing Population
(1999)
Table 6. Medical Research in Singapore
Medical Research Grants committed under
National Medical Research Council
(NMRC) ($M)
% of Medical Research Grants:
a. Enabling Grants / Centre / Program
Grants1
b. Individual Research Grants
c. Exploratory / Developmental Grants
d. New Investigator Grants
e. Singapore Translational Research
(STaR) Investigator Awards 3
f. Talent Development 2
g. Enablers & Infrastructure
h. Individual PI – Initiated Research
Grants (inclusive of New Investigator
Grants)
i. Strategic Research Grant Programs
FY
2006
53.5
FY
2007
125.7
FY
2008
94.4
FY
2009
121.3
FY
2010
95.0
FY
2011
116.0
FY
20𝟏𝟐𝟒
213.4
57.9
22.3
30.7
21.0
10.0
-
-
32.1
-
24.4
4.5
4.2
4.2
33.0
5.4
5.6
5.6
28.2
4.6
4.2
4.2
42.6
6.0
5.4
5.4
29.2
4.7
4.7
4.7
-
10
-
14.4
-
25.3
-
18.5
-
26.0
-
28.5
-
13.4
4.4
40.6
-
-
-
-
-
-
37.1
-
Source: Social Security Association: Office of Retirement and Disability Policy of the United States;
moh.gov.sg/content/moh_web/home.html
Notes:
1 – There was no commitment in FY2011 because NMRC is in the process of revamping the centre grants
framework for the new tranche of funding (RIE2015)
2 – Awards are only given to established researchers (local & international). No award will be given if
NMRC cannot find any suitable researchers
3 – Includes Clinician Scientific Award, Master Clinical Investigation, NMRC fellowship, etc.
4 – NMRC programs have ceased and transited to new funding initiatives FY2012
44
Figure 4. Health Expenditures (Thousands), PPP (Constant 2005, International $) in
Singapore
Helth Expenditure in Singapore
3000
In Thousands
2500
2000
Health Expenditure
1500
1000
500
Source: IndexMundi
45
2011
2010
2009
2008
2007
2006
2005
2004
2003
2002
2001
2000
1999
1998
1997
1996
1995
0
ABOUT THE AUTHOR
Princess Chezica T. Lao (tan_lao789@yahoo.com.ph) is currently a fourth year
Business Economics student in the College of Commerce and Business
Administration. She is a member of 3 organizations namely, Thomasian Writer’s
Guild, UST Scarlet Commerce Organization, and UST – Economics Society. She
had her internship program in the Philippine National Bank head office under the
Corporate Planning and Economic Research Department where she had utilized
her skills and knowledge that she acquired in UST.
Carla Felize C. Cruz (carlafelizecruz@yahoo.com) is currently a fourth year
Business Economics student in the College of Commerce and Business
Administration. She was a Student Coordinator of the College of Commerce
Student Council (2010-2011) and is a member of UST Scarlet Commerce
Organization, RCYC Red Cross Youth Council, and UST Economics Society.
She also offered her services in the Guidance Office as a Peer Facilitator. In
addition, she took her internship at the Philippine National Bank where she had
applied what she had learned from UST.
EunHyun Kim (k_eunhyun@yahoo.com) is currently a fourth year Business
Economics student in the College of Commerce and Business Administration.
She finished her secondary education in Miriam College High School Quezon
City (S.Y. 2010). She is a member to a total of three school organizations
namely, The UST Economics Society, UST International Student Association,
and UST Red Cross Youth Council. She had her practicum at the Philippine
National Bank Delta branch where she had applied what she had learned from
UST.
46
47