Alex Malone, Marion Ridley USF Dept. of Otolaryngology
advertisement

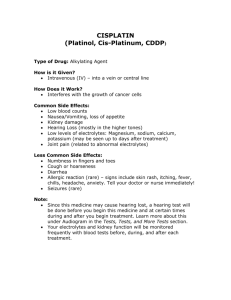
Intratympanic Steroids for the Treatment of Sudden Sensorineural Hearing Loss Alex Malone, Marion Ridley USF Dept. of Otolaryngology – Head & Neck Surgery 12901 Bruce B Downs Blvd, MDC 73 Tampa, FL 33612 Introduction: Idiopathic sudden sensorineural hearing loss (SSNHL) is a poorly understood clinical entity. It is classically defined as hearing loss that occurs in less than three days, involves a drop of at least 30 decibels in three contiguous frequencies on an audiogram, and with no other identifiable cause identified 1. There are 66,000 new cases reported annually in the US2. Some patients will experience spontaneous return of hearing to baseline while others suffer permanent deficits. No treatment regimen has been definitively shown to improve hearing outcomes but steroids have been proposed as a possible treatment and are commonly used in clinical practice. As many patients cannot tolerate steroids due to side effects intratympanic injections have arisen as a novel alternative, allowing higher doses to be delivered to the inner ear while minimizing systemic exposure3. Here we will report on the results of intratympanic injections performed at the James A Haley VA. Methods: A retrospective chart review was performed from 2010-2016 to identify all patients who presented to the James Haley VA Otolaryngology clinic with sudden onset hearing loss. All patients diagnosed with SSNHL after a thorough clinical exam and work-up were included. An audiogram demonstrating a 30 dB drop or greater in at least three contiguous frequencies was required to be included. In cases where no previous audiogram was available the contralateral ear was used to assess baseline-hearing threshold. All patients treated with intratympanic steroids were included in our analysis. Treatment modality, clinical notes, and serial audiogram results were evaluated to assess patient outcomes. The earliest audiogram occurring at least one year following pre-treatment audiogram was used to assess for changes in hearing level. If no audiogram greater than one year following treatment was available then the most recent audiogram was used. Time until treatment was also evaluated to assess for difference in outcome base on the time of presentation from initial reported symptoms. Treatment outcomes were broken down into ordinal categories based on recommendations from the American Academy of Otolarygnology – Head & Neck Surgery clinical practice guidelines1. Hearing recovery (using pure tone average) to within 10 dB of baseline and word recognition score (WRS) within 10% of baseline was defined as complete recovery. Case Number Age 1 2 3 4 5 6 7 9 11 12 13 15 16 17 19 20 23 24 25 26 27 29 30 31 34 35 77 59 60 65 62 72 80 74 70 76 66 85 33 39 70 39 84 68 61 65 63 67 65 65 56 87 Time Until Treatment (Days) 10 11 14 92 2 10 10 38 6 1 23 10 7 42 2 9 6 5 67 37 2 18 3 1 3 17 Initial Primary or Salvage Audiogream Treatment Shape Salvage Flat Salvage Flat Primary Flat Primary Down Sloping Primary Down Sloping Primary Down Sloping Primary Down Sloping Primary Flat Primary Flat - Profound Primary Up Sloping Primary Flat Primary Flat - Profound Primary Down Sloping Primary Down Sloping Primary Flat - Profound Primary Flat Primary Flat - Profound Primary Flat - Profound Primary Flat Primary Down Sloping Primary Down Sloping Primary Flat Primary Down Sloping Primary Flat - Profound Primary Flat - Profound Primary FlatProfound Recovery Type Complete Partial-Significant Complete None Complete Partial-Significant Partial-Significant Partial-Insignificant Partial-Significant Complete None None Complete None Complete Complete Partial-Insignificant Partial-Insignificant None Partial-Insignificant Partial-Insignificant Partial-Insignificant Complete Partial-Insignificant Partial-Significant None Audiogram Shape and Recovery 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Flat Complete Profound Partial-Significant Down Sloping Up Sloping Partial-Insignificant None Bibliography 1. Stachler RJ, Chandrasekhar SS, Archer SM, et al. Clinical practice guideline: sudden hearing loss. Otolaryngol Head Neck Surg 2012;146:S1-35. 2. Alexander TH, Harris JP. Incidence of sudden sensorineural hearing loss. Otol Neurotol 2013;34:1586-9. 3. Parnes LS, Sun AH, Freeman DJ. Corticosteroid pharmacokinetics in the inner ear fluids: an animal study followed by clinical application. Laryngoscope 1999;109:1-17. 4. Merchant SN, Durand ML, Adams JC. Sudden deafness: is it viral? ORL J Otorhinolaryngol Relat Spec 2008;70:52-60; discussion -2. 5. Byl FM, Jr. Sudden hearing loss: eight years' experience and suggested prognostic table. Laryngoscope 1984;94:647-61. 6. Cinamon U, Bendet E, Kronenberg J. Steroids, carbogen or placebo for sudden hearing loss: a prospective double-blind study. Eur Arch Otorhinolaryngol 2001;258:477-80. 7. Moskowitz D, Lee KJ, Smith HW. Steroid use in idiopathic sudden sensorineural hearing loss. Laryngoscope 1984;94:664-6. 8. Nosrati-Zarenoe R, Hultcrantz E. Corticosteroid treatment of idiopathic sudden sensorineural hearing loss: randomized triple-blind placebo-controlled trial. Otol Neurotol 2012;33:523-31. 9. Wilson WR, Byl FM, Laird N. The efficacy of steroids in the treatment of idiopathic sudden hearing loss. A doubleblind clinical study. Arch Otolaryngol 1980;106:772-6. 10. Alexander TH, Harris JP, Nguyen QT, Vorasubin N. Dose Effect of Intratympanic Dexamethasone for Idiopathic Sudden Sensorineural Hearing Loss: 24 mg/mL Is Superior to 10 mg/mL. Otol Neurotol 2015;36:1321-7. 11. Filipo R, Attanasio G, Russo FY, Viccaro M, Mancini P, Covelli E. Intratympanic steroid therapy in moderate sudden hearing loss: a randomized, triple-blind, placebo-controlled trial. Laryngoscope 2013;123:774-8. 12. Mattox DE, Simmons FB. Natural history of sudden sensorineural hearing loss. Ann Otol Rhinol Laryngol 1977;86:463-80. Partial-significant recovery was defined as improvement in hearing to of an aidable level of hearing with improvement in WRS to 50% or greater. Partial-insignificant recovery was defined as hearing improvement of pure tone average of >10 dB or improvement of WRS of >10%. No recovery was defined as improvement hearing improvement of <10 dB with improvement in WRS of <10%. Discussion: SSNHL is a clinical conundrum. Owing to the intricacy of the inner ear no pathologic specimens are able to be obtained from living subjects and because of its rarity there and relatively benign nature there are an extremely small number of post-mortem specimens available for review – with only one such specimen in existence during the acute phase of onset of this process4. A litany of treatment options have been proposed and studies but there is scant evidence to prove any effective5. Steroids had shown some evidence of efficacy in early trials but this has since come under question6-9. There has been some recent evidence that intratympanic steroids may have an effect on patient outcomes but more data is needed10,11. Historical data has suggested that approximately two-thirds of patients will experience some level of recovery in hearing, with one-third failing to improve5,12. Our data are similar, with approximately ½ of patients experiencing significant improvement and ¼ of patient’s experiencing no improvement. When examined more closely several interesting findings do arise. Most notable, our demonstration of some level of improvement in 94% of patients treated with intratympanic injection less than 14 days following onset of symptoms is dramatically higher than reported outcomes. Also noteworthy, our patient population was predominantly over the age of 60, which is associated with significantly decreased odds of recovery. Our only treatment failure of those treated within 14 days was an 85 year old with profound hearing loss, one of the oldest subjects in our cohort. All patients 60 and younger had a significant level of recovery aside for one patient who presented over one month after initial onset of hearing loss. Conclusion: Our data demonstrate the importance of early identification of SSNHL and importance of prompt referral to an audiologist and otolaryngologist. We have also demonstrated an improved chance of overall recovery compared to the historical literature in cohort. Our data supports the importance of intratympanic steroids in the treatment of SSNHL. Further studies are needed to verify our findings.