Physical Characteristics of Blood
advertisement

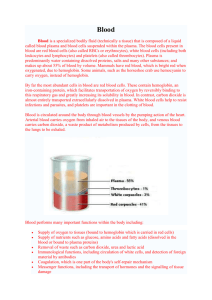
Physical Characteristics of Blood • Thicker (more viscous) than water and flows more slowly than water • Temperature of 100.4 degrees F • pH 7.4 (7.35-7.45) • 8 % of total body weight • Blood volume – 5 to 6 liters in average male – 4 to 5 liters in average female – hormonal negative feedback systems maintain constant blood volume and osmotic pressure Blood components • 55% plasma: 7 to 8% dissolved substances (sugars, amino acids, lipids & vitamins), ions, dissolved gases, hormones – most of the proteins are plasma proteins: provide a role in balancing osmotic pressure and water flow between the blood and extracellular fluid/tissues – loss of plasma proteins from blood – decreases osmotic pressure in blood and results in water flow out of blood into tissues – swelling – most common plasma proteins: albumin, globulins, clotting proteins (fibrin) Blood: Cellular elements • 45% of blood is the cellular elements or formed elements • 99% of this (44.55% of total blood) is erythrocytes or RBCs – formed by differentiation of hematopoietic stem cells (HSCs) in the red bone marrow of long bones and pelvis – makes about 2 million per second! – most numerous cell type in the body – 4 to 6 million per ul blood – as they mature in the marrow they lose most organelles and its nucleus – lack mitochondria and cannot use the oxygen they transport for ATP synthesis – lives only about 120 days – destroyed by the liver and spleen – liver degrades the hemoglobin to its globin component and the heme is degraded to a pigment called bilirubin - bile – Iron(Fe+3) • transported in blood attached to transferrin protein • stored in liver, muscle or spleen • attached to ferritin or hemosiderin protein -1% found in the Buffy coat : -leukocytes (WBCs) and platelets (thromobocytes) -neutrophils: phagocytic properties -release lysozymes which destroy/digest bacteria -release defensin proteins that act like antibiotics & poke holes in bacterial cell walls destroying them -release strong oxidants (bleach-like, strong chemicals ) that destroy bacteria - releases cytokines that attract other neutrophils -eosinophils: parasitic defense cells -also involved in the allergic response -release histaminase slows down inflammation caused by basophils -basophils: heparin, histamine & serotonin -heighten the inflammatory response and account for hypersensitivity (allergic) reaction -monocytes: enter various tissues and differentiate into phagocytic macrophages -lymphocytes: T and B cells Hematopoiesis Hematocrit • Percentage of blood occupied by cells – female normal range • 38 - 46% (average of 42%) – male normal range • 40 - 54% (average of 46%) • testosterone • Anemia – not enough RBCs or not enough hemoglobin • Polycythemia – too many RBCs (over 65%) – dehydration, tissue hypoxia, blood doping in athletes Blood Groups and Blood Types • RBC surfaces are marked by genetically determined glycoproteins & glycolipids – agglutinogens or isoantigens – distinguishes at least 24 different blood groups • ABO, Rh, Lewis, Kell, Kidd and Duffy systems RH blood groups • Antigen was discovered in blood of Rhesus monkey • People with Rh agglutinogens on RBC surface are Rh+. Normal plasma contains no anti-Rh antibodies • Antibodies develop only in Rh- blood type & only with exposure to the antigen – transfusion of positive blood – during a pregnancy with a positive blood type fetus • Transfusion reaction upon 2nd exposure to the Hemolytic Disease of Newborn • Rh negative mom and Rh+ fetus will have mixing of blood at birth • Mom's body creates Rh antibodies unless she receives a RhoGam shot soon after first delivery – can lead to miscarriage or spontaneous abortion of future Rh+ children – RhoGam binds to loose fetal blood and removes it from body before she reacts • Symptoms – oxygen-carrying capacity of blood is reduced – fatigue, cold intolerance & paleness Anemia • lack of O2 for ATP & heat production • Types of anemia – iron-deficiency = lack of absorption or loss of iron • type of nutritional anemia • failure to take in essential raw ingredients not made by the body – pernicious = lack of intrinsic factor for vitamin B12 absorption from the digestive tract • B12 is essential for normal RBC formation and maturation • binding of B12 to intrinsic factor allows its absorption • intrinsic factor – synthesized by the small intestine – hemorrhagic = loss of RBCs due to bleeding (ulcer) – hemolytic = defects in cell membranes cause rupture • rupture of too many RBCs by external factors such as malaria (normal RBCs) or genetic disorders like sickle cell anemia (defective RBCs) – thalassemia = hereditary deficiency of hemoglobin – aplastic = destruction of bone marrow (radiation/toxins) • failure of the bone marrow to produce enough RBCs • may selectively destroy the ability to produce RBCs only • but may also destroy the myeloid stem cells – affect WBCs and platelets Sickle-cell Anemia (SCA) • Genetic defect in hemoglobin molecule (Hb-S) that changes 2 amino acids in the globin protein – at low very O2 levels, RBC becomes deformed by changes in hemoglobin molecule within the RBC • sickle-shaped cells do not pass through capillaries well and get stuck = causing occlusions and decreased blood flow to organs • also rupture easily = causing anemia & clots • Found among populations in malaria belt – Mediterranean Europe, sub-Saharan Africa & Asia • Person with only one sickle cell gene – increased resistance to malaria because RBC Blood Clotting – in a test tube blood separates into liquid (serum) and a clot of insoluble fibers (fibrin) in which the cells are trapped – in the body the clot “plugs” damaged blood vessels and initiates healing – ultimate step is conversion of fibrinogen (soluble plasma protein) into insoluble fibrin • Substances required for clotting are Ca+2, enzymes synthesized by liver cells (clotting factors and plasma proteins) and substances released by platelets or damaged tissues – thrombin – released by damaged cells, catalyzes the conversion of fibrinogen to fibrin – 12 clotting factors involved • Clotting is a cascade of reactions in which each clotting factor activates the next in a fixed sequence resulting in the formation of fibrin threads – prothrombinase & Ca+2 convert prothrombin into thrombin – thrombin converts fibrinogen into fibrin threads Overview of the Clotting Cascade -may be triggered through two possible paths 1. extrinsic pathway 2. intrinsic pathway -either path leads to activation of the final common pathway in which thrombin cleaves fibrinogen to form fibrin Lymphatic & Immune System Lymphatic system: system of lymphatic vessels and organs -larger lymphatic vessels are similar to blood vessels - presence of valves -lymphatic vessels - for the transport of lymph -lymph: filtrate produced in tissues and NOT reabsorbed by the CV system -enters lymphatic capillaries from the tissues -low pressure system - moves by muscular contraction and breathing -capillaries join to form lymphatic vessels -vessels join to form: 1) thoracic duct 2) lymphatic duct - Right side head, arm & chest empty into right lymphatic duct and rest of body empties into thoracic duct -then dumped directly into left & right subclavian veins -lymphatic system is ONE WAY (from tissues to heart) Lymphatic organs: 1) lymph nodes: found at certain points along the lymphatic system -capsule surrounding an outer cortex and inner medulla -cortex contains immune cells = lymphocytes (fight pathogens) -medulla contains immune cells = macrophages (clean lymph) 2) tonsils: lymphatic tissue located in the pharynx (adenoids) or oral cavity (palatine tonsils) -defense against pathogens 3) spleen: upper left region of the abdomen -cleanses the blood -capsule, white and red pulp -white pulp contains lymphocytes -red pulp contains red blood cells & macrophages 4) bone marrow (red): adult - within the spongy bone of the epiphyses, pelvis, skull, clavicle, sternum -site of origin for all blood cells (RBCs, WBCs) -derived from hematopoietic stem cells (hematopoiesis) -also the site of origin for all mesodermal cells (bone, muscle, cartilage, fat…..) -derived from mesenchymal stem cells 5) thymus gland: located below the trachea, on top of the heart -divided into lobules -larger in children -production of T lymphocytes -production of hormones - thymosin - stimulates the lymphocytes located in other tissues 1) Non-specific defenses A)Mechanical barriers: first line of defense - Skin and mucus membranes lining the respiratory tract, digestive & reproductive systems e.g. ciliated epithelium of respiratory system - coated with mucus, coughed out B) Chemical barriers: first line of defense -acidic pH of the stomach interior -E.coli within the small intestine -gastric enzymes in gastric juice -high salt in perspiration kills some bacteria C) Fever: second line of defense -secretion of pyrogen by lymphocytes - raises body temp -rise in body temp enhances the phagocytic activity of immune cells D) Inflammation: second line of defense E) Phagocytosis Inflammation: 1) injury to tissue 2) synthesis of histamine, prostaglandins, pyrogens (heat) and kinins (pain) by damaged cells 3) histamine released - dilation of capillaries & increased blood flow 4) delivery of proteins (e.g. clotting response), increase of fluid in damaged area, reddening of skin - swelling 5) increased migration of neutrophils and monocytes/macrophages via dilated capillaries - phagocytosis of foreign particles 6) clotting response by blood - cascade/positive feedback - to minimize blood loss 7) macrophages release Colony stimulating factors - differentiation of more WBCs by the bone marrow 8) production and release of lymphocytes from lymph nodes - travel to infection site Prostaglandins • made by every cell in the body – stimulates smooth muscle contraction (PGE2) – stimulates synthesis of gastric juice • also made by damaged cells – stimulates blood clotting – thromboxane synthesis by platelets – stimulates the inflammatory pathway – pain and fever • • • • • • • • • work within the cell that makes them derived from arachadonic acid – phospholipid in the plasma membrane damaged cells release histamine – increases blood flow to damaged area – brings WBCs to the area – stimulates damaged cells to make prostaglandins – stimulates secretion of kinins (pain) and pyrogens (fever) also by damaged cells related cousin = leukotrienes AA is converted either into leukotrienes or into prostaglandins first PG made is called PGG2 – converted into PGH2 this conversion is done by a enzyme complex called cyclooxygenase – contains an enzyme called COX most cells express COX1 – normal production of PG damaged cells express COX2 – abnormal production of PGs (inflammation) and thromboxane (clotting) http://cti.itc.virginia.edu/~cmg/Demo/pdb/cycox/cycox.html http://users.rcn.com/jkimball.ma.ultranet/BiologyPages/I/Inflammation.html Blood clotting • step 1 (extrinsic): injured cells in vessel walls release tissue factor or thromboplastin or platelets contact the collagen of the damaged vessel wall and release factor VII (intrinsic) step 2 (extrinsic or intrinsic): these factors convert an inactive clotting factor X to its active form (requires calcium) • • – active factor X converts an inactive protein into an activator – prothrombin activator/prothrombinase • • • step 3 (common): PA converts prothrombin to thrombin (liver) step 4 (common): thrombin converts fibrinogen to fibrin step 5: fibrin forms a network which traps RBCs and platelets to form a clot – trapped platelets release factor XIII stabilizing the fibrin threads • Normal clotting requires adequate vitamin K – fat soluble vitamin absorbed if lipids are present – absorption slowed if bile release is insufficient • Required for synthesis of 4 clotting factors by hepatocytes – factors II (prothrombin), VII, IX and X • Produced by bacteria in large intestine 2) Specific Defenses (Immunity) Immunity: ability of the body to defend itself from infectious agents, foreign cells, cancer cells Antigens: -before birth, the body takes an “inventory” of all self proteins = antigens -lymphocytes develop receptors that allow them to distinguish between self and foreign -non-self antigens combine with T and B cell receptors and stimulate an immune reaction T Cell-mediated immunity:/Cell-mediated immunity -T = thymus derived -respond to antigens by cell-cell contact - attach to foreign cells directly -antigens are processed before interacting with T cells -antigen-presenting cells (B cells, macrophages) Antigen Presenting Cell (APC) • Foreign antigen in body fluid is phagocytized by the APC – macrophage, B cell, dendritic cell (Langerhans cell in skin) • • • Antigen is digested and fragments are bound to MHC-II molecules stuck into antigen presenting cell membrane APC migrates to lymphatic tissue to find T cells most of the antigens presented to T cells are self-antigens – so the T cell learns what is self and what is foreign • • • • • • APC displays the foreign antigen to the T cell this requires cell-cell contact between the APC and T cell in order to activate the T cell both T helper and cytotoxic T cells can be activated by an APC interaction between the MHC complex with the Ag and a complex of proteins on the T cell called the T cell receptor TCR = multiple proteins associated with a co-receptor (CD4 for a T helper or CD8 for a cytotoxic T cells) activation of the T cell now causes it to synthesize specific soluble chemicals called cytokines – interleukins and interferons APC T cell types • 1. Cytotoxic T cells (Tc cells) destroy virally infected cells and tumor cells – also implicated in transplant rejection. – are also known as CD8+ T cells, since they express the CD8 glycoprotein at their surface. – secrete perforin which punches holes in the foreign membrane • 2. Helper T cells, (Th cells) participate in bacterial infections – need to be activated by an APC – once activated - divide rapidly (clonal expansion) and secrete small proteins called cytokines that regulate or "help" the immune response. – also called CD4+ T cells – are a target of HIV infection - virus infects the cell by using the CD4 protein to gain entry. The loss of Th cells . • 3. Memory T cells - T cells that persist long-term after an infection has resolved. – quickly expand to large numbers of effector T cells upon re-exposure to their cognate antigen, – provide the immune system with "memory" against past infections. – comprise two subtypes: central memory T cells (TCM cells) and effector memory T cells (TEM cells). – may be either CD4+ or CD8+. B Cell-mediated immunity/Antibody mediated immunity -antibody producing cells -activated by interacting with an antigen that fits with an antibody displayed on the surface of the B cell -activation is helped by T helper cells - releases cytokines that induce the B cell to proliferate - clonal expansion -activated B cell differentiates into a plasma cell - secretes antibodies specific to the bound antigen and therefore similar in structure to the antigen receptor on the B cell surface Antibodies = Immunoglobulins -B cells produce a polyclonal response several types of antibodies against one type of foreign particle -comprised of 4 chains of amino acids linked by pairs of sulfur atoms (disulfide bonds) -two light chains, two heavy chains -each light and heavy chain has a variable region that recognizes a specific antigen -also called an antigen-binding site Antibody types: 5 major types 1) IgG = immunoglobulin G -plasma and tissue fluids -effective against bacteria, viruses and toxins -activates the complement system 2) IgA - exocrine gland secretions e.g. breast milk, tears, nasal discharge, gastric juices 3) IgM - blood plasma -develops in response to contact with certain antigens in foods and bacteria -also activates complement 4) IgE - exocrine secretions with IgA -associated with the allergic response 5) IgD - surfaces of most B cells -activation of B cells B cell types • 1) Plasma B cells (also known as plasma cells) – large B cells that have been exposed to antigen – produce and secrete large amounts of antibodies • 2) Memory B cells - formed from activated B cell – activation requires interaction with between the B cell and an antigen encountered during the primary immune response. – are able to live for a long time – respond quickly following a second exposure to the same antigen. • 3) B-2 cells are the conventional B cells most texts refer to. B cell activation • requires binding of a foreign antigen to the antibody displayed on the surface of the B cell – antigen is internalized and processed into fragments which are displayed in association with the MHC-II complex = APC • the membrane bound antibody is called a B cell receptor (BCR) – the BCR recognizes the unprocessed form of an antigen – the TCR recognizes a processed form of the antigen • • interaction of the B cell displaying the antigen activates the T helper cell interaction leads to the differentiation of the B cells into a plasma cell and production of soluble antibodies – activated T cells secrete lymphokines which stimulates the differentiation of the B cell Antibody actions 1) direct attack on antigens - combine with antigens and cause them to agglutinate or clump -easier to phagocytose -or neutralizes the toxic portions of an antigen by binding -or causes antigens to precipitate and become insoluble 2) activation of complement -group of proteins in plasma and body fluids -activation of complement proteins by IgM and IgG results in several effects including: coating Ag-Ab complexes (susceptible to phagocytosis), attraction of macrophages and neutrophils (Chemotoxis), rupturing of foreign membranes, altering structure of viruses 3) stimulates changes in local environment making spread of antigens difficult Immune Responses Primary response: when B or T cells become activated after an intial exposure -release of IgM then IgG by plasma cells into the lymph -several weeks -several B and T cells become dormant but persist in the lymph = memory cells -if an identical antigen is encountered - clonal expansion and an immediate response called a Secondary response -lasts years Immunity Types 1) Passive - when an individual is given prepared antibodies to combat a disease -temporary because the Ig’s are not produced by the individual -passed from mother to child in breast milk -usually given as a gamma globulin injection (blood serum) from a person who have recovered from an infection 2) Active - develops after exposure to an antigen -also can be induced through exposure to small amounts of the pathogen Immunization = administration of a vaccine -vaccine = contains small amounts of an antigen to which the immune system responds -antigens are treated so that they are no longer virulent (i.e. no longer replicates or no longer viable) -today - bacteria can be engineered to mass produce specific proteins from a pathogen e.g. Hepatitis B vaccines -active immunity depends on the presence of memory T and B cells -long lasting - although booster shots may be required e.g. Diptheria, tetanus, pertussis - age 4 to 6 years, tetanus boosters at 11 and 14 years and older e.g. Polio - age 2, 4 and 6 months, 4 to 6 years, no booster e.g. measles, mumps, rubella - 12 to 15 months, 4 to 6 years, booster at 11-12 years Allergies -hypersensitivities to substances such as pollen, dander, or other substances that normally do no damage to others -these antigens = allergens -four types of allergic responses 1. Immediate response: -within seconds of contact -cold-like symptoms -caused by release of IgE antibodies by allergen activated B cells -IgE are also found on cell surface of mast cells in tissues and basophils in the blood -allergen-IgE interaction causes release of histamine from these cells -severe reaction = anaphylatic shock e.g. bee sting - first exposure results in high sensitivity -second exposure can be fatal due to massive histamine release, resulting in increased vessel permeability and a drastic drop in blood pressure -allergy shots - build up of IgG which will react with the allergen before the allergens can interact with IgE Allergic reactions • • • • allergen stimulates the B cell to secrete IgE antibodies these IgE antibodies bind to mast cells and basophils these release histamine immediately – immediate reaction but they also wait and release prostaglandins and leukotrienes – longer term cold like symptoms - inflammation 2. Delayed response: -intiated by memory T cells -regulated by cytokines secreted by T cells e.g. tuberculosis skin test - positive = red and hardened at injection site e.g. contact dermatitis - poison ivy, jewelry, cosmetics