Urinary System
advertisement

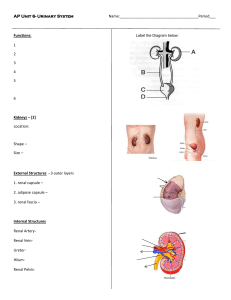
Chapter 26 Urinary System 26-1 I. Functions of the Urinary System • A. Filtering of blood: involves three processesfiltration, reabsorption, secretion. • B. Regulation of – 1. Blood volume – 2. Concentration of blood solutes: Na+, Cl-, K+, Ca2+, HPO4-2 – 3. pH of extracellular fluid: secrete H+ – 4. Blood cell synthesis • C. Synthesis of vitamin D 26-2 II. Kidney Anatomy and Histology • A. Retroperitoneal • B. Right kidney overshadowed by liver • C. Renal artery and renal vein enter and exit hilum • D. Protected by layer of fat 26-3 E. Internal Anatomy of Kidneys • • • • • • • • • • • 1. 2. 3. 4. 5. 6. cortex pyramids renal papilla medulla renal columns calyx a. Minor b. Major 7. renal pelvis 8. ureter 9. hilum 26-4 F. The Nephron 1. Functional and histological unit of the kidney 2. Renal corpuscle a. Bowman’s capsule b. Glomerulus 3. Proximal convoluted tubule 4. Loop of Henle 5. Distal convoluted tubule 6. Collecting Ducts 7. Cortex 8. Renal pyramid 9. Renal papillae 10. Juxtamedullary nephrons (15%) 11. Cortical nephrons 26-5 G. Renal Corpuscle-General view Bowman’s capsule a. Parietal layer b. Visceral layer made up of podocytes 2. Glomerulus 3. Afferent arteriole 4. Efferent arteriole 5. Juxtaglomerular cells 1. 26-6 H. Bowman’s Capsule more closely • 1. parietal layer • 2. visceral layer with podocytes with filtration slits • 3. glomerular capillary covered with visceral layer of Bowman’s capsule • 4. juxtaglomerular cells with macula densa making up the juxtaglomerular apparatus-site of renin production • 5. notice diameters of afferent and efferent arterioles 26-7 I. Filtration Membrane 1. Fenestrae: 2. Filtrations slits: 26-8 J. Cells of nephron reflect function 1. Proximal tubule: simple cuboidal epithelium with many microvilli-site of reabsorption 2. Loops of Henle-production of osmotic gradient – Descending limb: simple squamous epithelium – Ascending limb: distal part thicker and simple cuboidal 3. Distal tubule: shorter than proximal tubule. Simple cuboidal, but smaller cells and very few microvilli-site of secretion 4. Collecting ducts: Larger in diameter, simple cuboidal epithelium. Site of urine concentration 26-9 K. Arteries and Veins of the Kidneys 1. 2. 3. 4. Afferent arterioles Glomerulus Efferent arterioles Peritubular capillaries form a plexus around the proximal and distal tubules 5. Vasa recta: specialized parts of peritubular capillaries that course into medulla along with loops of Henle, then back toward cortex 26-10 III. Urine Production A. Three basic steps 1. Filtration 2. Reabsorption 3. Secretion 26-11 B. Amount of Filtration • Movement of fluid, derived from blood flowing through the glomerulus, across filtration membrane • Filtrate: water, small molecules, ions that can pass through membrane • Pressure difference forces filtrate across filtration membrane • Renal fraction: part of total cardiac output that passes through the kidneys. averages 21% • Renal blood flow rate: 5600 ml/min X .21 = 1176 ml/min • Renal plasma flow rate: renal blood flow rate X fraction of blood that is plasma: 1176 ml/min X .55 = 650 mL/min • Filtration fraction: part of plasma that is filtered into lumen of Bowman’s capsules; average 19% • Glomerular filtration rate (GFR): amount of filtrate produced each minute. therefore 650ml/min X .19 = 124ml/min • Amount of filtrate formed per day = 180 liters/day • Average urine production/day: 1-2 L. Most of filtrate must be reabsorbed 26-12 C. Filtration Pressure = GCP-CHP-BCOP Changes in afferent and efferent arteriole diameter alter filtration pressure Dilation of afferent arterioles/constriction efferent arterioles increases glomerular capillary pressure, increasing filtration pressure and thus glomerular filtration 26-13 D. Regulation of GFR 1. Autoregulation – Involves changes in degree of constriction in afferent arterioles – Myogenic mechanism: As systemic BP increases, afferent arterioles constrict and prevent increase in renal blood flow – Tubuloglomerular feedback: Increased rate of blood flow of filtrate past cells of macula densa: signal sent to juxtaglomerular apparatus, afferent arteriole constricts 26-14 2. Sympathetic regulation:norepinephrine a. What do you think will happen? b. Constricts small arteries and afferent arterioles c. Decreases renal blood flow and thus filtrate formation d. During shock or intense exercise: intense sympathetic stimulation, rate of filtrate formation drops to a few mm e. Not a problem over short duration-normal response as blood is shunted to skeletal muscle f. Prolonged shock can damage kidneys 26-15 E. Tubular Reabsorption in general: 1. occurs as filtrate flows through the lumens of proximal tubule (majority), loop of Henle, distal tubule, and collecting ducts 2. Processes involve diffusion, facilitated diffusion, active transpot, and osmosis 3. Substances transported to interstitial fluid and reabsorbed into peritubular capillaries 4. 99% of filtrate volume is reabsorbed. 5. These substances return to general circulation through venous system 26-16 F. Reabsorption in PCT 1. Substances pass through – Apical surface – Basal surface: – Lateral surfaces 2. Active transport of Na+ across the basal membrane from cytoplasm to interstitial fluid linked to reabsorption of most solutes 3. Number of carrier molecules limits rate of transport ie. diabetes mellitus 4. Filtrate volume reduced by 65% due to osmosis of water 5. Osmotic pressure of filtrate remains 300 mOsm due to permeability char of membrane 26-17 G. Reabsorption in Loop of Henle 1. Descending loop of Henle passes into an ever increasing concentrated environment. Simple squamous epithelium. 2. Descending limb is highly permeable to water and moderately permeable to urea, sodium, most other ions 3. In descending limb, water moves out of nephron, solutes in. Volume of filtrate reduced by another 15%. 26-18 Reabsorption in Loop of Henle 4. The wall of the ascending limb of the loop of Henle is not permeable to water. 5. Ascending limb moves Na+ across the wall of the basal membrane by active transport. 6. At the end of the loop of Henle, inside of nephron is 100 mOsm/kg. 7. Interstitial fluid in the cortex is 300mOsm/kg. 8. Filtrate within DCT is much more dilute than the interstitial fluid which surrounds it. 9. Loop of Henle like the trap below the sink in the kitchen 10. Establishes concentration gradient as you pass into the medulla 26-19 H. Reabsorption in DCT and Collecting Duct 1. 2. 3. 4. 5. 6. Filtrate which reaches DCT is dilute with respect to interstitial fluid DCT and collecting duct are the sites where hormonal control of urine volume occurs-finishing touches Two ducts are affected by ADH In presence of ADH these two become very permeable to water In absence of ADH, relatively impermeable DCT can also reaborb more sodium ion, but this is also under hormonal control of aldosterone 26-20 I. Tubular Secretion 1. Moves metabolic by-products, drugs, molecules not normally produced by the body into tubule of nephron 2. Active or passive 3. Ammonia: produced by epithelial cells of nephron from deamination of amino acids. Diffuses into lumen 4. H+, K+, penicillin, and substances such as para-aminohippuric acid (PAH): actively secreted into nephron 5. Hydrogen ions are moved into tubule as Na ions are reabsorbed-major mechanism of body in regulating tissue fluid pH 26-21 Urine Production Summary • In Proximal convoluted tubules – Na+ and other substances removed – Water follows passively – Filtrate volume reduced by 65% • In descending limb of loop of Henle – Water exits passively, solute enters – Filtrate volume reduced an additional 15%-only 20% of original filtrate remains • In ascending limb of loop of Henle – Na+, Cl-, K+ transported out of filtrate – Water remains • In distal convoluted tubules and collecting ducts – Water movement out regulated by ADH • If absent, water not reabsorbed and dilute urine produced • If ADH present, water moves out, concentrated urine produced 26-22 Loop of Henle 26-23 26-24 Urine Concentrating Mechanisms 26-25 IV. Regulation of Urine Concentration and Volume: A. Renin/Angiotensin/Aldosterone Mechanism 1. 2. 3. 4. 5. 6. 7. 8. 9. Mainly a mechanism to regulate blood pressure Cascade of events occurs to result in Na ion reabsorption and therefore water Sensory mechanism for the system is located in the juxtaglomerular complex Two stimuli result in the release of renin from this area a. Decreased stretch of the afferent arteriole of the glomerulus b. Decreased concentration of Na ions in the distal convoluted tubule Released renin converts a liver protein “angiotensinogen” into angiotensin I AngiotensinI -> angiotensinII by a proteolytic enzyme found in capillaries of lung Enzyme is called angiotensin-converting enzyme (ACE) Angiotensin II is a very powerful vasoconstrictor Angiotensin II also increases aldosterone secretion-increases reabsorption from distal convoluted tubule 26-26 The juxtaglomerular complex is the site of renin release 26-27 26-28 B. ADH Mechanism 1. 2. 3. 4. 5. 6. 7. 8. 9. Mainly regulating osmolarity of the blood and tissue fluids Secondarily affecting blood pressure Osmoreceptors are found in hypothalamus of the brain Reacts secondarily to pressure receptors in atria, carotid sinuses, and aortic arch ADH effects the permeability of the distal convoluted tubule and collecting ducts Water reabsorption before this portion of the nephron is obligatory Filtrate entering the distal convoluted tubule possesses an osmolarity of 100 mOsm Depending upon the amount of ADH released, urine’s final osmolarity can vary from 100 to 1200 mOsm From as little as less than 1 liter to 20 liters in the total absense of ADH (diabetes insipidus) 26-29 ADH Mechanism 26-30 C. ANH-atrial natriuretic hormone 1. 2. 3. 4. 5. Produced by right atrium of heart when blood volume increases stretching cells Inhibits Na+ reabsorption Inhibits ADH production Increases volume of urine produced Venous return is lowered, volume in right atrium decreases 26-31 Some Youtube sites • http://www.youtube.com/watch?v=uo-NOrP49I 26-32 V. Urine Movement A. Hydrostatic pressure forces urine through nephron B. Peristalsis moves urine through ureters from region of renal pelvis to urinary bladder. C. Occur from once every few seconds to once every 2-3 minutes 1. Parasympathetic stimulation: increase frequency 2. Sympathetic stimulation: decrease frequency D. Ureters enter bladder obliquely through trigone. Pressure in bladder compresses ureter and prevents backflow 26-33 VI. Anatomy and Histology of Ureters and Bladder A. Ureters: bring urine from renal pelvis to urinary bladder. Lined by transitional epithelium B. Urinary bladder: hollow muscular container. In pelvic cavity posterior to symphysis pubis. Lined with transitional epithelium; muscle part of wall is detrusor C. Trigone: interior of urinary bladder. Triangular area between the entry of the two ureters and the exit of the urethra. Area expands less than rest of bladder during filling 26-34 Anatomy and Histology of Urethra • Male: extends from the inferior part of the urinary bladder through the penis • Female: shorter; opens into vestibule anterior to vaginal opening • Internal urinary sphincter: in males, elastic connective tissue and smooth muscle keep semen from entering urinary bladder during ejaculation • External urinary sphincter: skeletal muscle surrounds urethra as it extends through pelvic floor. Acts as a valve 26-35