HEPAHP 2
==
HEALTH EDUCATION & PROMOTION
FOR
All HEALTH PROFESSIONS
(HEPAHP)
The Way ahead Towards
Assertive Patient Centered Health Education with Best Evidences
Johali APCHE'R QUALITY
Book vision
الطريق إلى تثقيف وتعزيز صحي معتمد على المرضى مبني على البراهين
Book vision
Eisa Ali Mohammad Johali
1صفحة
عيسى بن علي بن محمد الجوحلي
Riyadh الرياض
2011/1432
JOHALI HEPAHP 2011
PART SIX
HEPHAP Most related
ETHICAL BASES
Chapter 10
JOHALI HEPAHP 2011
2صفحة
JOHALI HEPAHP 2011
HEPAHP ETHICAL BASES
THE MOAJOR ISLAMIC ETHICAL BASES
ISLAMIC ESSENTIALS
The main Islamic sources (Holly Qura’an & the Prophet
Sunnah) have many essentials deal with Personality development &
ethics. As Islam is the Holly Comprehensive Religion, Its essentials
are covered all “Life & Day After Sciences” including the Basic
Sciences of Health Education & Human Communication, the Major
related Essentials ) محمد أبو زهرة/ (االمامare:
1) Individual/Personal Nature & Educational Development
التربية والتطور الطبيعي للفرد
2) Social Security/Welfare & Relationships
التكافل واألمن والعالقات االجتماعية
3) COMMUNICATION RIGHTS
حقوق التعامل والتواصلل
As a Muslim learner, you have to find at least (Aiah or Hadeeth) as scientific evidence for each
3صفحة
JOHALI HEPAHP 2011
THE MOAJOE ISLAMIC ETHICAL BASES
ISLAMIC FOUNDATIONS FOR HEPAHP QUALITY
Derived from its essentials, Islam is the life and the day after, The Major
related are:
الكرامة اإلنسانية
1. HUMAN NOBILITY / Dignity
العدالة والمساواة
2. JUSTICE & EQUITY
3. HUMAN COOPERATION
التعارف والتعاون اإلنساني
4. FORGIVENESS/COMPASSION/AFFECTION
الرحمة والمودة/ التسامح
اإلخالص/األمانة
5. HONESTY / FIDELITY
6. BENEFIT/ USEFULNESS المنفعة والمصلحة/البر/اإلحسان
===========
As a Muslim learner, you have to find at least (Aiah or Hadeeth) as scientific evidence for each
----------------------------------------------------------Compare these FOUNDATIONS with the later Global Ethics
4صفحة
JOHALI HEPAHP 2011
HEPHAP ETHICAL BASES
GLOBAL ETHICS
ETHICS are essential not only to overcome health professions’ problems and
barriers, but for all life and professions, by which we can improve the quality of life.
ETHICS always connected to the religions, as a main source or bases, thus, many
social and ethical references are started with "Moral Reasoning & Development".
DEVELOPMENT OF MORAL REASONING
In Islamic nations, Moral is the religion “Values, Beliefs, Attitudes…”, due to global
disagreement, the West & worldwide create “THREE MAJOR LEVELS with SIX STAGES:
1) PRE-CONVENTIONAL LEVEL
STAGE 1: Moral Realism
STAGE 2: Individual & Instrumental Morality
2) CONVENTIONAL LEVEL
STAGE 3: Interpersonal Normative Morality
STAGE 4: Social System Morality
3) POST-CONVENTIONAL LEVEL
STAGE 5: Human Rights & Social Contract Morality
STAGE 6: Universal Ethical Principles (because People seen as having
value in themselves rather than as agent of social values, thus it emphasis
the “Self chosen for best Justice; Human dignity & Rights → Optimum
Quality,
JOHALI HEPAHP 2011
5صفحة
HEPAHP ETHICAL BASES (Cont.)
ETHICS PRINCIPLES
Drives from their moral reasoning, there are many Western Ethical Principles, The
MOAJOR ARE:
1) BENEFIENCE : Act in the best interest of the patient, it is a moral
(religious) principles, the Western traced to Hippocratic pledge. Meanwhile,
it is one of the major Islamic Principles.
2) AUTONOMY: Patients rights to self-determination; to chose what will be
done to them.
3) HONESITY : Patients have the right to the truth about their medical
conditions, the course of their disease, the treatments recommended &
alternative treatment available.
4) INFORMAL CONSENT : this is a part of Autonomy & honesty principles.
The patients have the right to be informed about all the relevant medical
aspects including the treatment.
5) CONFIDENIALITY : based on the human dignity, patients have the right to
assure that all the information about their medical conditions & treatment
will not be given to other without their prior permission.
6) FIDELITY/ Loyalty: Your responsibilities should be directed toward the
“Patients Welfare”, not to the physician interests
=================
Ego Reflective:
Compare these with “Islamic Teachings”
6صفحة
JOHALI HEPAHP 2011
ETHICAL – COMMUNICATION BASES (Cont.)
HEPAHP SEVEN SEAS (7 C’s)
OF
QUALITY HUMAN COMMUNICTION
1. Credibility: You the source “the Sender (S)” must be competent and
reliable to Motivate
2. Context: HE Message (HEM) must be relevant to the receiver
3. Content: HEC must have genuine meaning “meaningfulness”
4. Clarity: the R “Patient” must be able to understand the message
5. Continuity: Though repeated with variations, HE Message must be
consistent (steady reliable) enough NOT to Confuse the R
6. Channels: HE must use the most acceptable communication
channels\media (HE methodology & technology) to the R
7. Capability: The R must be able to communicate effectively with Least
amount of Effort
JOHALI HEPAHP 2011
7صفحة
HEPAHP ETHICAL BASES (Cont.)
THE SEVEN (7) TOPS
OF
HEALTH COMMUNICTION SKILLS
1. Give accurate & Adequate Feedback
2. Listening Carefully
3. Interpreting Accurately
4. Giving Clear Directions
5. Treating Others in Professional Manner
6. Communicating Information Clearly
7. Establishing One’s Credibility
(Pagano & Ragan 1992; 29)
Also you can visit: http://www.ehow.com/how_4489822_achieve-great-communication-skills.html
8صفحة
JOHALI HEPAHP 2011
COMMUNICATION BASES & SKILLS (Cont.)
Three Major Steps to Improve Quality of Patient Communication
1. Prepare a list of questions for you before the appointment. Even if time is limited,
having a list of questions will help keep the visit on track. According to Medical News
Today website, doctors and all HPs should also always encourage patients to ask questions
about their medical care. This will also ensure that the patient believes that the appointment
was productive.
2. Check for misunderstandings between you and your patient. To prevent
misunderstandings regarding medical services care, all HPs should verify that their patients
understands what was discussed during the appointments, as well as any instructions they
were given about care.
3. Involve the patient in medical decisions . All of you should ask patients their
opinions on introducing new medication or new plans for care. Though the you is more
knowledgeable about care, the patient should be incorporated in the decision-making
process, so she/ he feels respected and involved. According to the "British Medical
Journal," patients who think that they are not involved in decisions about their care tend to
leave their doctors.
Modify from:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1113402/ in http://www.ehow.com/how_7583545_create-communication-between-doctors-patients.html
9صفحة
JOHALI HEPAHP 2011
HEPAHP ETHICAL-COMMUNICATION BASES (Cont.)
HEPAHP COMMUINICATION TOTAL QUALITY
In addition to the tradition to Top 10s Quality:
Who really understand the term "Quality" just as (Ideal & Excellency), will consider
its deep Islamic roots and the "Japonica–American" principles which focus on:
- Patient humanity and ethical based communication, by which you
will reach…
- Crosby's Zero Defect: HEPAHP without defects, then you will
meet..
- Patient fulfill needs and satisfaction, your patients will be full
satisfy if your activity meet their interests and needs.
Almost all these concepts are in the following Parts & Chapters.
10صفحة
JOHALI HEPHAP 2011
PART SEVEN
APCHE’R
QUALITY
Assertive Patient Centred HE’R
with
Best Evidence
Chapter 11
JOHALI HEPAHP 2011
JOHALI HEPAHP 2011
11صفحة
HEPAHP SCIENCE OF MANAGEMENT
In our step by step HEPAHP, the style of managing HEPAHP Process is
the last step towards "APCHER, it is a vital which will lead our model to
achieve its overall aim "Quality of Healthful Life".
There a huge numbers of management theories and approaches. For this
course, the most related is “WHO Open System Planning Approach (OSPA)or
it is called the 7-S Management framework:
“WHO Training Manual on Management of Human Resource For Health”
http://www.anythingresearch.com/Strategic-Planning/7-S-Management-Framework.htm
Why OSPA in HEPHAP?;
There are many reasons, the major is to remind you with your work environment
“with whom you are working: with persons under legal and not only with MOH and
related medical professions but with academic sectors, people and technologies. Shared
value with patients feelings, is the most significance for HEPAHP, it is a part of our
quality model that we have to look for the best style to achieve our aim. .
JOHALI HEPAHP 2011
12صفحة
HEALTH EDUCATION MANAGERIALSTYLES
ASSERTIVE (FEELING) THE IDEAL WAY TOWARDS QUALITY OF HEPAHP
The Behavioral, Psychological, Social & Educational Sciences & Scientists (e.g Carol Rogers
father of Person Centred Psychotherapy”; Jean Piaget; Bloom; Dewey....etc) create many
behavioral/managerial responses. As arranged from the “Highest to the Lowest” effect on the quality
of human communication & Education, the MOST COMMON STYLES ARE:
The Highest the Most Trusted Styles “Ethically–Humanity” the Highest Quality HEPAHP
ASSERTIVENESS (Confidence, Self assure, Be empathic –feel others Feeling; Communicate
without Attack..):
Give patient freedom for direct expression of ideas, opinions ands desires. The intent of Assertive
PT behavior is to communicate in an atmosphere of TRUST. It is “how to communicate straight
without hurting others”. It focuses “On What we should Do rather than What we want others to Do”
The Assertive communicate message caries Feeling, Behavior and Effect”:
Example: I feel angry (Feeling), when you are not comply with medication (Attitude/Behavior)
and/thus, I blame you (Effect)
For deep understanding of (feeling, attitude, effect)
(Reflect on/in personality structure & Behaviorism – the Bloom Taxonomy of educational Objectives).
PASSIVE AGRESSIVENESS (Indirect Attack, non assertive):
Indirect attack, who has the intent to attack, but is carried out in an indirect avoiding way. Passive
behavior designed to avoid conflict at all cost; The Passive or non assertive PTs do not say what they
really think out of fear, that other may not agree. They “hide” at pharmacy corner or behind window..
The recipient/Receiver is often left Puzzle & Confused?!
OFFENSEVENESS/ACTIVE AGGRESSIVE(Direct attacker; Not friendly, non peaceful/ not
healthy):
Aggressive people seek to “win” in conflict situation by dominating or intimidating (threatening)
other.
Offensive is the direct attack behavior by which a parson decide to hit out others using blame and
putdown words e. g: “As usual you are being hopeless”.
Aggressive/Offensive PTs, the persons who promote their own interests or points of view indifferent
way or hostile to the feeling, thoughts and needs of others.
The Lowest the Less Trusted Styles “Ethically–Humanity” the Less Quality HEPAHP
JOHALI HEPHAP 2011
13صفحة
WHAT & WHY
APCHER QUALITY ?
APCHER based on the above Assertive Style the Feeling of others the patients
“HPs feel that they are he is the patient” this is the Ideal way to assure quality
In addition to ”caries feeling of patient”, It covers all related scientific concepts
that we have learn with (e.g Carol Rogers father of Person Centred
Psychotherapy”; Jean Piaget; Bloom; Dewey....etc)
As a Muslim, its overall goal is not just "Quality of Healthful Life" the intent goal,
the desire and the need for every person, patient and every community and nations,
but it will achieve the quality of our life today and the day after.
APCHE’R Quality Model consists of “Three Major Models”:
Patient Centred HEPHAP; the Patients Self Awareness;
Readiness, and Willingness. When our people aware, ready and
willing sure they will
Assertive based HEPHAP Style;
Moral, spiritual and
emotional ideal religious "Islamic - Sympathetic" Feelings; By
which all health leaders, planners, and providers have to feel that
they are the Patients, they are carrying others' pains, sickness,
healthful and happiness feelings.
Best Evidence HEPHAP; the scientific research & assessment
of all patients health and his its associated factors, the nature,
characters, interests and needs …
Our creative APCHER Quality model arranged “Highest to the Lowest” effect on
the quality of human communication & Education as follow:
JOHALI HEPAHP 2011
14صفحة
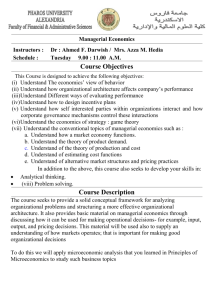
ASSERTIVE PATIENT CENTREDHE'R
With BEST EVIDENCE
Johali APCHER QUALITY Model
PATIENT CENTRED Based on BEST
EVIDENCE With ASSERTIVE SYLE
Health Care & Cost effective
↔
QUALITY
↔
QQ
Patient–People–Community–the whole Nation
ِ HEPAHP
ASSERTIVE
EMPATHETIC– FEELINGS
↕
RELIGIONS &IICULTURE
V
Values
AِA
READENESS
Attitude
Needs
PATIENTS/
PERSONS
Behave
Risk
WELLINGNESS
Norms
Interests
Problems
Factors
FrF[
Best Evidence
the HEP
Scientific
Research&- Environment
Assessment
Progressive
& Promotion
Education;
Professions
Knowledge(Johali
– Attitude
; Affect
Act as modified
Other's Feel,
need
and Interests
23-25
– 03 –– 2006;
8 Sep
2007)
↔
↔
Health Care - Cost effective
QUALITYmodified
Patient
– People – Community
– the whole Nation
(Created 23-25-03-2006;
8 September
2007)
HE & MLT Educational & Professional Sciences & Experiences
15صفحة
JOHALI HEPAHP 2011
PART EIGHT
HEPAHP
METHODOLOGIES
&
TECHNOLOGIES
Johali
Chapter 12
JOHALI HEPAHP 2011
JOHALI HEPHAP 2011
16صفحة
METHODOLOGIES & TECHNOLOGIES
Methodology refers to the sciences (theories and models) of teaching and learning
approaches, strategies and methods that appropriate to specific nature, character
and objectives...
Technology refers to sciences of teaching and learning aides “audio- visual,
materials..” that appropriate to the methodologies....
The literature of health education and its boundaries has huge numbers of
methodologies and technologies that associate with philosophies and theories of
teaching and learning. Each philosophy and theory of teaching and learning has its
own strategy to meet its own concepts, and to achieve its objectives.
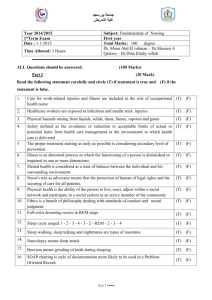
Based on philosophers and theories of education and health, and the Fox’s four
theories, this is my overall model for choosing the most appropriate HEPAHP
methods, media and strategie:
Johali Approach to decide the appropriate M & T
DEPENDENT
T& L Theories
Transferring
Shaping
Traveling
PASSIVE
-VE
T& L Methods & Strategies (e.gs)
Lecture Knowledge
Drill, Labs Skills
informal field study\visit\gurney Self ability
Computing Technologies & Networks: CDs, IAL.. Saudinet, Gulfnet, Internet)
Growing
“Tran.+Trav.+ Shap”.
Formal & Informal teaching Learning: sharing, co-operative,
self\open learning;
Reading Ref., book, materials - CTs & Networks..
INDEPENDENT
ACTIVE
+ VE
Who looks for the Quality, should use more than one theory as possible.
In order to achieve our overall aim, we have to move from dependent to independent,
from passive to active and positive learning theories.
JOHALI HEPAHP 2011
17صفحة
THE MOST COMMON “HE” METHODOLGIES
Johali Approach to choose the best HEP Methodology
The most common health education strategies, methods are ordered according to its
effectiveness on the following concept:
The First/ Formal/Single/Dependent & Passive /-VE The Last/ the Informal & Multi- Independent & Active / +VE
ARE
DEPENDENT
PASSIVE
-VE
LECTURE: traditionally, a verbal speech to teach, instruct, transfer
knowledge or information and, progressively with others to help
learning.
QUESTIONING & DISCUSSION (Individual & Group) to
explain and exchange for groups, and may be with individuals.
DIALOGUE & DEBATE for free and wide exchange, the best
recommended for HA
DEMONSTRATION to see / show how to:…
CASE STUDY show by example how to decide
ROLE PLAYING an experiential learning to demonstrate opinions
and feelings and to copy skills
SIMULATIONS & GAMES for imaginative & attractive practice
LABS\DRILL the real practice at labs & field
PROBLEM SOLVING a self confident if it is independent
PATIENT/EVIDENCE/ASSERTIVE CENTRED HE new
concepts for optimum quality
SELF/INDEPENDENT HEHA the highest quality for those who
ready & welling
INDEPENDENT
ACTIVE +VE
INTERACTIVE + VE
Johali 1413 (HENUR); Johali HEHA2006 ; modified 2011
Who looks for the APCHER Quality have to use more than one with highest approaches
In order to achieve our overall aim, we have to move from dependent to independent,
from passive to active and positive methodologies.
18صفحة
JOHALI HEPAHP 2011
THE COMMON “HE” TECHNOLOGIES
Johali Approach to choose the best HEP Technologies
The most common health education technologies as listed according to its effectiveness
ARE
PASSIVE
-VE
PRINTED MATERIALS
e.g; Leaflet/ Folder, Poster, Pamphlet, Booklet, Books…..
AUDIO-VISUAL AIDES
e.g; Overhead/ Slide projectors, Recorder….
MASS MEDIA
Television, Radio, Newspapers, Magazines, Satellite
HIGH HIYPER-INTERACTIVE COMPUTING TECHNOLOGIES
HYPER
Interactive& Attractive
TELCOM / SPACE TELECOM/ INTERNET
INDEPENDENT
ACTIVE +VE
INTERACTIVE + VE
Who thinks about the quality have to use more than one of the latest accepted ..
Other General & HEPAHP methodologies, technologies (Strategies): Advantages and Disadvantages &
Relations.. are shown in the Tables:..
Discover which we are looking for – which can achieve APCHER Quality
19صفحة
JOHALI HEPAHP 2011
Example of HEPAHP Strategies
( CAP Objective Based Methodologies)
Teaching Objectives
O kinds
Strategy
(M \T)
Patient
Status
Advantages
• Economic times
and resources
• Large patients
& information
Disadvanta
ges
• Quantity
only
• Passive
Think/Pro
mote
- Very
limited
1. Present \Provide
Information
- Cognitive
- Lecture
- AVAs
- Reading
Passive
2. Encourage
understanding
- Cognitive
- Affect
- Problem
Solving
- G work
- Programme
d learning
Active
- Need
experts
- Moderate
limited
3. Encourage
investigation of
attitude and
value
- Affect
- Cognitive
• G. work
• Share
experiences
Active
Limited
-Cognitive
-Affect
-Psycho
• Demonstrati
on
• Games
• Simulation
Active
4. Develop
psychomotor
and
interpersonal
skills,
Example
(Recommen
d)
• Large
group of
patient
at 1st visit
Recommended
with al
HEPAHP
Adapted from Kiger 2004; Redman1993; Gilbert & Sawyer2000
Despite that almost the results are acceptable, it is projected to conduct similar local surveys soon.
JOHALI HEPAHP 2011
20صفحة
HEPAHP TECHNOLOGIES 1
Advantages _ Disadvantages & Practice with different situations
Aid
Advantages
Disadvantages
Example
1.Pilnted matterbooks,hand-outs
• Allows self-pacing.
• Learners can relar to when required .
• Reduces need for note-taking,
therelcre anxiety.
• Hand-outs can be made specitle to
individual learning needs.
• Supplements teaching session
•Books expensive and rapidly out
of date.
• Hand-outs must be carafully
Planned and used appropriately
should not replace teaching.
• Copyright law prohibits mass
duplicalion of copyrighted
material.
In discussion of nutrition,
Hand-outs about essential
Food groups and how to
assess if family me mbers are
eating properly
2.Models of life,
e.g. skeleion .
•Three-dimensional
• Resemble reality.
• Allow for close examination
• Allow for practic e.
• Visual and tactile senses stimulated.
•Ma/be expensive
• Cannot replace reality
• Useful for small groups only.
Use of doll in antenalal class
demonstrations for expectant
parents.
3. Real specimens
• Present reality
• Three – dimensional
• Visual and tactile senses stimulated
•Not easily available
• Useful for small groups only
• May be expensive, difficult to
store.
4.Graphicscharts,posters,
drawing,
photographs
• Visual sense stimulated
• Production of materials should be
• Promote organization and correlation of high standard
of material
• Useful for small groups only
• Help to approximate reality
• Easily stored, retrieved
Used for discussion different
behavioral health problems:
e.g. drugs, alcohol, smoking,
accidents ….
5.Blackboard
• visual sense stimulated
• Inexpensive
In sexuality leaching use of
this aid in diagramming
orgasm response in
• skill needed for effective use
• It using daring presentation
Adapted from Kiger 2004; Redman1993; Gilbert & Sawyer2000
21صفحة
JOHALI HEPAHP 2011
HEPAHP TECHNOLOGIES 2
Advantages _ Disadvantages & Practice with different situations
Technologies
Advantages
Disadvantages
Example
Cont 5.
• Accommodates larger audience 30-50
• Allows for development of
presentation
• Allows for clarification , summary
• Usable for a range of purposes
• Back to audience
• Work erased
6. Boards:
Flannel,
magnetic,
bulletin and eblac k boards
• Easy to assemble and use
• Can use repeatedly
• Others may participate
• Visual sense stimulated
• Limited usefulness
• Inappropriate for certain
purposes and audiences
For young diabetics ,
choosing correct food items
and creating a daily menu
7. Field Trips
• Motivating
• Active involvement
• Presentation of reality
• costly in time for organization
and accomplishment
• Transport needed
• For small appropriate groups
only
For psychiatric patients ,
visits to shops to assess
appropriate selection of
clothing items
8. Overhead
projection
• Visual sense stimulated
• Easy to prepare and use
• Available to large audiences
• Can be preplanned or used on spot
• can illustrate process stages and
develop material
• Can allow for participation of leamers
• Electricity required
• Equipment costly
• Transparencies need to be
careiully planned for effective use
With renal failures patients,
to explain the mechanism of
kidney function and to
illustrate what renal allure
means
Adapted from Kiger 2004; Redman1993; Gilbert & Sawyer2000
22صفحة
JOHALI HEPHAP 2011
HEPAHP STRATEGIES
Health Problem and Behavior Based Characters
Diagnostic
Criterion
Desired
Educational
Outcomes
Prevalent
category
Cognitive
HEPAHP Strategies
Audiov
isual
aids
Lecture
Individu
al
instructi
on
Mass
media
Program
med
Learning
\ ETV
Inquiry
Learning
Simulati
ons and
games
Peergroup
discussi
on
√
√
√
√
√
√
√
√
√
√
√
Affect
Psycho.
HI
√
Simple
√
Modelin
g
Behavior
modifica
tion
√
√
√
Complexity
√
Complex
HB
Simple
Complexity
Complex
HB
Short
Duration
Long
HB
Infrequent
Frequency
HB Extent
√
√
√
√
√
√
√
√
√
√
√
√
√
√
√
√
√
√
Frequent
Rare
√
Widespread
HB
Nature
Additive
√
√
√
Substantive
Adapted from Kiger 2004; Redman1993; Gilbert & Sawyer2000
√
23صفحة
JOHALI HEPHAP 2011
Recommended HEPAHP Strategies To Age; Believe & Socioeconomic Status
Diagnosti
c Criterion
Prevalent
category
HEPAHP Strategies
Audiovisu
al aids
Age
Mass
media
Primary
school
children
√
√
√
√
Secondar
y school
√
√
√
√
√
√
Programe
d
Learning \
TV
√
√
Inquiry
Learning
Simulatio
ns and
games
√
√
√
√
√
√
√
√
√
√
√
√
Weak
Moderate
Socioeco
nomic
statue
Individual
instruction
Infants
and
preschool
children
Adults
Believes
HBM
Lecture
√
√
√
Strong
√
High
intermedi
ate
√
Adapted from Kiger 2004; Redman1993; Gilbert & Sawyer2000
Peergroup
discussio
n
Modeling
Behavior
modificati
on
√
√
√
24صفحة
JOHALI HEPAHP 2011
Taxonomy CAP Based Recommended HEPAHP Strategies
Diagnos
tic
criterion
Stage in
diffusio
n
process
Prevale
nt
categor
y
Recommended HEPAHP Strategies
Progra
m
learning
\ TV
Educati
onal
televisio
n
Simulati
ons and
games
Peergroup
discussi
on
√
√
√
√
Cognitiv
e
applicati
on
analyse
s
synthesi
s and
evaluati
on
√
√
Affectiv
e
√
√
Cognitiv
e
knowled
ge
compre
hension
Audiovi
sual
aids
Lecture
Individu
al
instruct
or
√
√
√
Mass
media
√
Modelin
g
Behavio
r
modific
ation
√
√
Psycho
motor
Adapted from Kiger 2004; Redman1993; Gilbert & Sawyer2000
Commu
nity
develop
ment
25صفحة
JOHALI HEPAHP 2011
Etiology based Characters of Some HEPAHP Strategies
Diagnostic
criterion
Prevalent
category
Recommended Strategies
Audio
visual
aids
Etiology of
problem
Stage of
intervention
Lecture
Program
learning
\ TV
Educatio
nal
televisio
n
Simulati
ons and
games
Peergroup
discussi
on
Modelin
g
Behavi
or
modifi
cation
Primarily
medical /r
behavioral
√
√
√
√
√
√
√
√
Primary
prevention
√
√
√
√
√
√
√
√
Secondary
prevention
√
√
√
Treatment
and
rehabilitati
on
√
√
√
√
√
√
√
√
√
Low
High
Communit
y
developme
nt
√
Primarily
enviroeconomic
Post
treatment
follow – up
Degree of
scientific
and social
consensus
on etiology
and priority
problem
Individua Mass
l
media
instructio
ns
√
√
√
√
Adapted from Kiger 2004; Redman1993; Gilbert & Sawyer2000
√
√
26صفحة
JOHALI HEPAHP 2011
HYPER TECHNOLOGY (HT)
(Move HEP from Black\White Board to HT )
HE Hyper Technology
Johali
27صفحة
JOHALI HEPAHP 2011
PART NINE
Looking for the Quality of HEPHAP
HEPAHP PLANNING
Chapter 13
PROBING & DEFINING HEPAHP TERMS
Key Terms
JOHALI HEPAHP 2011
28صفحة
JOHALI HEPAHP 2011
PROBE & DEFINE PLANNING TERMS
The HEPAHP Most Related
HEPAHP PLANNING Defining Terms just the most repetitive
Updated 9 Feb 2010
Johali HEPT 2011
29صفحة
JOHALI HEPHAP 2011
PROBE & DEFINE PLANNING TERMS
HEPAHP Planning Defining most constant Terms
Updated 9 Feb 2010
Johali
30صفحة
JOHALI HEPHAP 2011
HEPAHP Planning Defining most constant Terms
Updated 9 Feb 2010
Johali
31صفحة
HEPAHP Planning Defining most constant Terms
Updated 9 Feb 2010
Johali
32صفحة
JOHALI HEPHAP 2011
HEPHAP PLANNING DEFINTION & PRINCIPLE
As we have noticed from defining key terms. Generally; “HEALTH PLANNING /
PLANNING FOR HEALTH” is define as :
“A
Process of establishing priorities, diagnosing causes of problems
and allocating resources to achieve objectives”.
Meanwhile, its is scientific PRINCIPLE is:
PEOPLE ACT POSITIVE IF HEALTH EDUCATION RESPECTS THIER PERSONALITY
NATURE, CHARACTERS, INTERESTS & MEET THIER NEEDS.
Thus;
The “HEHA PLANNING is “a dynamic process of integrating the following major
activities:
Understanding “Personality”/ clients nature & behaviors..,
Assessing their needs,
Defining objectives,
Establishing priorities,
Allocating resources,
Acting/working to achieve/improve Quality of Health
33صفحة
JOHALI HEPHAP 2011
PROBING (WHY & HOW..) QUALITY OF PLANNING?
To prepare well, manage, validate and grantee the quality of H. E. activities & outcomes
LEARNING & PLANNING FOR QUALITY
As we have taught and may be learnt, for understanding the boundaries and its
concepts, normally, we have to start by defining health education; its goals and
objectives; its philosophical and theoretical concepts; methodologies, technologies and
research and finally, the planning process.
Outcomes
QUALITY HEALTH/WHY
Inputs
QUALITY EDUCATION/HOW
In order to plan for the quality of health of clients, people and community, it is
recommended to “start from the end or bottom, from the field (patient, clients, people,
community) as follow:
Inputs
QUALITY EDUCATION/HOW ..
Outcomes
QUALITY HEALTH/WHY
(THINKING IN THE FOLLOWING MODELS)
General Models (Ross & Mico fig 13 “Model 1” p 209 & table 11 p 210-211; fig 14 “Model
2” p 212 and table 12 p 214-215)
The FOCUS MODEL “PRECEDE framework” (Ross & Mico fig 12 p 206-207; fig 3 p7071)
HEHA PLANNING MODELS: The Concise
34صفحة
JOHALI HEPHAP 2011
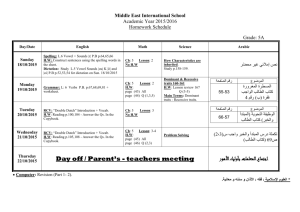
Predisposing Reinforcing Enabling Causes in Educational Diagnosis Evaluation
FRAMEWORK
HEPHAP PLANNING BY “P..R...E...C..E..D..E..”
Administrative Diagnosis
Social
Phase 6
Educational Diagnosis
Behavioral Diagnosis
Phase 5 , 4
Phase 3
Impact
Epidemiology &
Phase 2 , 1
Outcomes
Predisposing
HEMLT
Components
Reinforcing
Behavior
Healthy- non
Healthy
HEMLT
Quality
Enabling
7)Evaluation
Process
Impact Factors
Outcomes
To understand think what is PRECEDE; from it comes ?
-
PRECEDE is P……….; .………. ; ………... Causes in ……….. Diagnosis ……….
PRECEDE is Predisposing; Reinforcing; Enabling Causes in Educational
Diagnosis Evaluation
35صفحة
JOHALI HEPHAP 2011
Applying “P..R...E...C..E..D..E..”
Practice PRECEDE with
Hypertension a General Example
Practice PRECEDE with any common health problem in your specialty
36صفحة
JOHALI HEPHAP 2011
TURING
MANAGEMENT HBM & NURSING PROCESS
Into
A HEPHAP PROCESS CYCLED PLANNING MODEL
As HE is a new course introduced into HA, Its planning must take in consider the most related
scientific concepts of “HE & HA, with HBM the common medical model and the Nursing Process. The
Best modified “HEPHAP QUALITY PROCESS PLANNING MODEL” can be illustrated
as follow:
Practice PPCM, turned it with your specialty
(Johali 1997; modified 29/03/2006)
37صفحة
JOHALI HEPHAP 2011
Johali's CONCISED HEPHAP PLANING MODEL
(Based on all above HEPHAP Sciences)
HEPHAP the QUALITY OF HEALTHFUL LIFE
PROMOTE/DEVELOP
QUALITY OF HEALTH / LIFE
Why What/When/ Where/How & Who
EVALUATION
QUALITY OF HEALTH / LIFE
Why What /Where/When/Who & How
INTERVENTION\ACTION PLAN
QUALITY OF HEALTH / LIFE
Diagnose assessments Define needs
(Physical, Environmental\ Health, Non health causes & needs?\
Predisposing, Enabling and Reinforcing educational factors & needs?)
Objectives, Priorities, Resources PLAN
EMPATHETIC DIAGNOSIS & PLAN SETTING (Why, What & How?)
QUALITY OF HEALTH / LIFE
1. Assessing personality structure & needs (heredity, culture, social and self)
2. Assessing personality health problems, related factors & needs
3. Assessing personality behaviors & needs
4. Assessing educational requirements & needs
How good communication & observation
ASSERTIVE (Empathetic) ASSESSMENT (Why & How?)
"Learners have to invent similar self concise model"
(HENUR 1997; Modified to HEHA/HEMLT; HEPT & HERT 30 March 2006; HEPHAP Dec 2010)
38صفحة
JOHALI HEPHAP 2011
HEALTH EDUCATION
FIELDS/SPECIALTIES & RESOURCES
HEALTH EDUCATION FIELDS/SPECIALTIES
Either it is accepted or rejected; it is carried out or may neglected, it is the fact that
health education is a part of all health professions, institutions & activities. Furthermore,
it has many (FEILDS/TYPES) Specialties, The Majors Are:
General/Public Health Education (G/PHE)
Hospital Health Education (HHE): Patient & Outpatients
Primary Health Care Education (PHCE)
Community Health Education (CHE)
School Health Education (SHE)
Nursing Health Education (NHE)
Clinical Nutrition Health Education (CNHE)
Environmental Health Education (EHE)
Occupational & Safety Health Education (OSHE)
Chronic Diseases Health Education (CDHE): Diabetic, HBP, Cancer….
Drugs Control & Pharmaceutical Health Education
These specialties can be reorganized as: Individual or Personal; Group, Community and
Public ….Health Education
39صفحة
JOHALI HEPHAP 2011
HEALTH EDUCATION RESOURCES
LOCALLY
In Saudi Arabia, despite that there is no special “Association or Board”… as it is the case of
global HE, there are many HE Resources.
In addition to a department within every government and private health service sectors, the major HE
government sectors are:
1. Department of Health Education, General Directorate of Preventive Health, Ministry of Health,
which is located at “Al Suliamnia, King Abdul Azis Road.
2. Department of Health Education, King Khalid Eyes Specialist Hospital, Riyadh. The most active
HE hospital department now, mainly in regarding of HE symposium.
3. Department of Health Education, Kin Fahd Specialist Hospital, King Abdul Aziz Medical City,
National Guard.
4. Department of Health Education, Riyadh Military Hospital. It is the oldest department, and it was
the most active hospital HE department mainly with HE researches & materials.
5. Department of Health Education, King Fisal Specialist Hospital & Research Centre.
6. Department of Health Education, General Directorate of Schools Health, Ministry of Education,
“the place of “Uniceef HE Seat Fond”.
7. Department of Health Education, Security Force Hospital, Riyadh.
8. Academic Department of Health Education, College of Applied Medical Sciences, King Saud
University, Riyadh. The lonely academic department. It establishes at 1403 AH.
9. Saudi Health Specialties Council (Association), It services all health professions including heath
education specialists & heath educators.
“independently, you have to discover the activities of these sectors and other national sectors”
40صفحة
JOHALI HEPHAP 2011
ملخص التثقيف والتعزيز الصحي للمدير الصحي وكافة المهن الصحية
HEPHAP COURSE CONCISED SUMMARY
"Book philosophy framework"
By EISA JOHALI, the lecturer
The PLACE OF HE IN HA SCIENCE-EDUCATION & PRACTICE
(1)
HISTO-PROBE “EDUCATION?HEALTH?HEHA DEF.& RELATIONS
(2)
GOAL/OBJECTIVES
HEHA (TEACHING+LEARNING+PRACTICE QUALITY OF LIFE
(3)
MAJOR HEHA SCIENCES
PERSONALITY THEORIES
(HEREDITY + ISLAMIC CULTURE & SOCIETY YOU & CLIENT)
(4)
HEHA (TL + HA) THEORIES
LEARNING = MOTIVATION (READY & ACTIVE LEARNER & CLIENT) +VE BEHAVIOR
(5)
HEHA ISLAMIC & GLOBAL ETHICS & COMMUNICATION
(6)
HEHA METHODOLOGY & TECHNOLOGY
Interactive Strategy +VE Method & Technique Excite Media
(7)
QUALITY-ASSERTIVE HEHA PLAN
(7) + (6) + (5) + (4) + (3) + (2) + (1)
ASSESSMENT DIAGNOSIS INTERVENTION\ASSERTIVE ACTION PLAN
(8)
ASSERT. EVALUATION\RESEARCH DEVELOPMENT(8 -1)
(HEHA2006, 29 Mar. Johali)
"Learners have to invent similar self concise model"
41صفحة
JOHALI HEPHAP 2011
Annexes
Researches; References &
Resources
JOHALI HEPHAP 2011
42صفحة
HEPHAP STUDIES & RESEARCHES
43صفحة
Author Studies & Researches
(Soon will send )
44صفحة
Global Studies & Researches
ERIC #:
ED156649
Title:
Authors:
Descriptors:
The Place of Health Education in Health Administration. Report on a Working Group.
Source:
PeerReviewed:
Publisher:
Publication
Date:
Pages:
Pub Types:
Abstract:
Abstractor:
Reference
Count:
Note:
Identifiers:
Record
Type:
Level:
Institutions:
Sponsors:
N/A
Delivery
Systems; Foreign
Countries; Government
Role; Health
Education; Health
Programs; Organizational Theories; Public Health; Relationship; Role Theory
N/A
N/A
N/A
1977-00-00
27
Reports – Research
Four working papers presented at a World Health Organization Regional Office for
Europe Working Group meeting on the place of health education in health administration
are summarized, along with group discussion of the papers. General discussion of the
meanings of health education and health administration, types of integration, and methods
of achieving integration of the two are also presented in condensed form. Papers prepared
for the meeting were: (1) "Health Education Administration in the European Region;" (2)
"The Theory and Practice of Health Education as Related to the Place of Health Education
in Health Administration;" (3) "Health Education in the North Karelia Project: Principles
and Recommendations;" and (4) "The Place of Health Education in the Health
Administration of Yugoslavia." General group discussion focused on descriptions of
health education systems, types of health care systems, types of health education systems,
health education and health problems, health education agents, methods of development of
health administration services, general factors influencing future developments and
identification of present needs. Conclusions and recommendations of the Working Group
to the Regional Office conclude the paper. (MJB)
N/A
N/A
Meeting of a Working Group (Manchester, England, March 2931, 1976)
Europe; Health Administration
Non-Journal
1 - Documents indexed from January 1993 forward available for free through the ERIC
Web site; all others restricted to microfiche
N/A
World Health Organization, Copenhagen (Denmark). Regional Office for Europe.
45صفحة
HEPHAP SITED & ELECTRONIC RESOURCES
http://www.qurancomplex.org/searchsite/eng/hits.asp
American Health Administration Association ………...
http://www.utwente.nl/cw/theorieenoverzicht/Theory%20clusters/Health%20Communica
tion/Health_Belief_Model.doc/
Others HEP INTERNET SITES.
American Academy on Physician and Patient
European Association for Communication in Healthcare
Visit Patient Education and Counseling Online
Online Sample Copy
46صفحة
The Authors’ Collection & Publications
Johali
47صفحة
THE MAJOR REFERENCES & RESOURCE
JOHALI, E. A. (1427) A Concise Medical Laboratory Health Education: A Lecture’s Note
(you can by it “ready & bind” from AL Quwafil Centre, King Abdullah Road, south east of King Saud
University. (This Concise is the Major student Reference)
ROGERS R. C (1983) Freedom To Learn for the 80’S. New York: MacMillan Publishing C.
JOHALI, E. A. (2006) A Concise Health Profession History & Ethics: An Arabic & English
Lectures’ Note for Health Professions Students.
Al Mazrou et al (1410) Principles and Practice of Primary Health Care.
WEDDING, M. E & TOENJES, S. A. (1992) Medical Laboratory Procedures (Focus:
Preface, Units 1 & Appendixes ). Philadelphia: F. A. Davis
GREEN, L.W et al (1980) Health Education Planning: A Diagnostic Approach. USA:
Mayfield Publishing Co.
ROSS, H. S. and MICO, P.R. (1980) Theory and Practice in Health Education. USA:
Mayfield Publishing Co.
Redman, 1993 The Process of Patient Education. Mosby Year Book.
Tyler, R. W. (1949) Basic Principles of Curriculum and Instruction. USA: the University of
Chicago Press.
Brown, S. and MacIntyre (1993) Making Sense of Teaching: Developing teachers and
teaching. Buckingham: Open University Press.
Ministry of Health (MOH) 1398H/1978G Manual of Functions and Duties in Health
Education (Arabic)
MOH (1410) The Curriculum Guidelines for Clinical Laboratory Technicians Programmes.
KIMBROUGH, V.K. & HENDERSON, K. (2006) Oral Health Education “Part 4
Communication Styles”. New Jersey: Pearson Prentice hall.
TINDALL, W. N. et al 2003 (4th Ed) Communication Skills in Pharmacy Practice: : A
Practical Guide for Students & Practitioners. Williams & Wilkins.
KERPS. G. & KUNIMMOTO, E (1994) Effective Communication in Multicultural Health
Care Settings. Sage Publications.
PORRITT, L (1984) Communication Choices for Nurses. Churchill Livingstone.
WHO (undated) Training Manual on Management of Human Resources for Health.
48صفحة