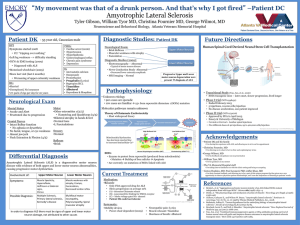
Clinically Possible ALS
advertisement

EMGer Beware! EMG and neuromuscular traps in your waiting room Shawn Jorgensen Albany Medical Center 2015 AAPM&R Annual Assembly Disclosures • None The Champ • 61 year old healthy male referred by PCP for bilateral upper limb EMG The Champ • 18 months of vague left upper limb pain and left lower limb pain without clear numbness and tingling • Complains that his abdomen “sticks out,” has trouble keeping his posture The Champ • No other sensory complaints • Generalized weakness • No trouble with vision, hearing, swallowing, speech, chewing • No trouble controlling his bowel or bladder The Champ • MRI cervical spine 3 months with “disc problems” • Followed by one neurosurgeon for the cervical spine • Followed by another neurosurgeon for an acoustic neuroma, no surgery planned The Champ • PMH ▫ Acoustic neuroma, congenitally absent left radius and right kidney • PSH ▫ Right carpal tunnel release, prostate surgery • Meds ▫ none • Family history ▫ No muscle, nerve, or rheumatological problems in the family that he can recall • Social history: ▫ Retired high school administrator and former teacher. Currently coaches golf and assistant coach basketball. Exercises twice a week, never smoked, drinks socially The Champ • Differential (based on history): ▫ Peripheral Focal mononeuropathy Brachial plexopathy Cervical radiculopathy ▫ Central Cervical myelopathy Intracranial process (right) The Champ • Physical exam ▫ General Appearing healthy, stated age, congenital left upper limb deformity ▫ Cranial nerves normal II-XII ▫ Motor MMT: 5/5 bilateral upper, lower limbs except: 4/5 left wrist extension 2/5 right thumb opposition 4/5 right thumb abduction 4/5 right finger abduction No atrophy Fasciculations frequent and continuous in biceps, triceps, quadriceps, lateral abdominal wall The Champ • Physical exam ▫ Reflexes 2+ right biceps, triceps, brachioradialis 1+ left triceps; bilateral patella and ankles 0 left biceps, brachioradialis No Hoffman, Babinski ▫ Sensation Pinprick Intact bilateral UE/LE, trunk, face Vibration Felt for 17 seconds at the bilateral toes ▫ Coordination No tremor The Champ • Differential (based on history and physical) ▫ Diffuse Generalized peripheral neuropathy Pure motor or with prominent motor involvement Neuromuscular junction disorder Myopathy Motor neuron disease ▫ Focal Radiculopathy Plexopathy Focal mononeuropathy The Champ • Studies ▫ Imaging MRI cervical spine 3 months earlier C5-6 disc osteophyte with right greater than left foraminal narrowing Minor DDD/DJD at other levels No significant central stenosis, cord compression, or myelomalacia The Champ • Next step (while in the office)? ▫ EMG The Champ • Studies ▫ Motor NCS: Right ulnar: nl latency, amplitude, CV, no TA/CB Bilateral median: nl latency, amplitude, CV, no TA/CB Right fibular: nl latency, amplitude, CV, no TA/CB ▫ Sensory NCS: Right sural: nl peak latency, amplitude Bilateral median D4: right prolonged peak latency, left normal, both amplitudes normal Ulnar D4: nl peak latency, amplitudes bilaterally The Champ The Champ • Differential (based on EDX) ▫ Diffuse ▫ Primarily motor Motor neuron disease LMN only Neuromuscular junction disorder Myopathy With abnormal spontaneous activity With large MUAP - chronic Neuropathy Multifocal motor neuropathy The Champ • End of office visit • Next step ▫ Diagnosis? ▫ More tests? The Champ • Diagnosis? ▫ ALS, LMN predominant The Champ • ALS ▫ Motor neuron disease ▫ A (primarily) pure motor process with features of both upper and lower motor neuron death and dysfunction The Champ • EMG/neuromuscular Take Home Point #1 ▫ Pure motor processes Small portions of nervous system where sensory and motor fibers diverge The Champ • EMG/neuromuscular Take Home Point #1 ▫ Pure motor processes Must be ANATOMICALLY selective to the motor system Pure motor nerve Neuromuscular junction Muscle Or METABOLICALLY selective to the motor system Motor neuron diseases Multifocal motor neuropathy AMAN (pure motor GBS) Case #1 - The Champ • EMG/neuromuscular Take Home Point #1 ▫ Pure motor processes Rare (and often bad) The Champ • ALS ▫ Presentation History Often complain of loss of a functional task, rather than weakness ▫ “weakness”=fatigue, loss of specific function=weakness (Amato 2008) Initial weakness ▫ 1/3 bulbar ▫ 1/3 upper limbs ▫ 1/3 lower limbs (Chancellor 1993) Often focal atrophy without sensory complaints The Champ • ALS ▫ Presentation Physical examination Clinical pearl! Upper and lower motor neuron signs ▫ Upper ▫ Weakness, clumsiness, spasticity, increased MSR, Hoffman, Babinski ▫ Preserved reflexes in an atrophic limb is considered an increased reflex! (Rowland 1995) ▫ Lower ▫ Weakness, atrophy, flaccidity, decreased MSR, fasciculations The Champ • EMG/neuromuscular Take Home Point #2 ▫ Upper and lower motor neuron signs together Most likely: ALS Radiculomyelopathy The Champ • EMG/neuromuscular Take Home Point #2 ▫ Upper and lower motor neuron signs together Radiculomyelopathy When both are seen, it is your next job to rule this out – treatable ▫ Unlikely if there is: ▫ No sensory signs ▫ Prominent bulbar signs ▫ UMN signs ROSTRAL to LMN signs • Lesion at the cervical cord ▫ LMN at the site of injury ▫ UMN below the injury ▫ UMN always below LMN • Clinically Probable ALS • Is defined on clinical or electrophysiological evidence by LMN and UMN signs in at least two regions with some UMN signs necessarily rostral to (above) the LMN signs • Clinically Possible ALS • Is defined when clinical or electrophysiological signs of UMN and LMN dysfunction are found in only one region: or UMN signs are found alone in two or more regions; or LMN signs are found rostral to UMN signs. Neuroimaging and clinical laboratory studies will have been performed and other diagnoses must have been excluded. (de Carvalho 2008) •Just get the MRI!! The Champ • EMG/neuromuscular Take Home Point #2 ▫ Upper and lower motor neuron signs together ALS without UMN signs? On presentation ▫ Increased reflexes about ½ ▫ Babinski about 1/3 (Gubbay 1995) • What is in the picture above: ▫ A) MUAP ▫ B) Fasciculation potential ▫ C) You can’t actually tell without seeing if it live to see if there is a regular pattern of firing and if the waveform changes every time or is the same morphology and size The Champ • EMG/Neuromuscular Take Home Point #3 ▫ Fasciculations Randomly occurring isolated MUAP Does not have a regular firing pattern Not the same one back to back Often visible if occurring near the surface – others deep, only dx with NEE or US (Misawa 2011) The Champ • EMG/Neuromuscular Take Home Point #3 ▫ Fasciculations Differential diagnosis (Dumitru 2002) LMN injury ▫ ▫ ▫ ▫ Radiculopathy Plexopathy Peripheral neuropathy Motor neuron disease Tetany Hyperthyroidism Viral illnesses Medications ▫ Mestinon NORMAL VARIANT!!! The Champ • EMG/Neuromuscular Take Home Point #3 ▫ Fasciculations NORMAL VARIANT!!! 70% of healthy patients Anxiety, fatigue, heavy exercise, coffee, smoking all increase likelihood in normal individuals (Blexrud 1993) Majority in the foot intrinsics or gastroc-soleus (Dumitru 2002) • Is the fasciculation potential shown here: Otherwise, they are distinguished by the presence of other signs of LMN injury such as abnormal spontaneous activity and neurogenic MUAP ▫ A) benign ▫ B) malignant ▫ C) You can’t actually tell with standard needle EMG. There have been attempts based on polyphasicity but they are not reliable. SFEMG can tell malignant ones by increased jitter and blocking. The Champ • EMG/Neuromuscular Take Home Point #3 ▫ Fasciculations Relevance Very difficult to distinguish “malignant” from “benign” fasciculations in isolation ▫ Cannot be done reliably with needle EMG ▫ Increased jitter and/or blocking = abnormal (Dumitru 2002) Importance dictated primarily by the “company that they keep” The Champ • EMG/Neuromuscular Take Home Point #3 ▫ Fasciculations Relevance (Blexrud 1993) 121 patients at Mayo clinic followed diagnosed with benign fasciculation syndrome by normal neurological exam and EMG (except fasciculations) NONE developed symptomatic motor neuron disease in follow up phone calls 2-32 years after The Champ • EMG/Neuromuscular Take Home Point #3 ▫ Fasciculations Relevance With a normal neurological exam and normal EMG ▫ Unlikely motor neuron disease In setting of weakness or signs of motor axon loss on needle EMG ▫ Likely motor neuron disease Motor neuron disease almost never presents with chief complaint of fasciculations ▫ 3% (Gubbay 1985) The Champ • ALS ▫ Diagnostic studies No imaging or lab study can diagnose sporadic ALS In a patient with a suspicious clinical and EDX presentation, no lab test can rule out ALS (Brooks 2000) The Champ • ALS ▫ Diagnostic studies Almost every case of suspected ALS gets: EDX ▫ document evidence of widespread denervation, both active and subacute-chronic ▫ exclude neuropathies, especially MMN MRI ▫ Bulbar signs – brain ▫ No bulbar signs – cervical spine ▫ OK to do both The Champ • ALS ▫ Diagnostic errors False positives (diagnosed with ALS but don’t have it) 5-10% of cases About half have a treatable diagnosis, such as mulitfocal motor neuropathy or a cervical radiculomyelopathy (Davenoport 1996) The Champ • ALS ▫ Diagnostic errors False negatives (diagnosis of ALS missed) Nearly 50% of cases (Belsh 1990) Usually lumbar and cervical stenosis About 30% have unnecessary surgery (Belsh 1996) The Champ • Summary ▫ Pure motor processes are rare and often bad ▫ Upper and lower motor neuron findings in the same patient are rare and a radiculomyelopathy has to be excluded ▫ Fasciculations with abnormal EMG/exam are often motor neuron disease; with a normal EMG/exam are usually benign The Champ • Post script ▫ Work up for LMN predominant ALS CK, serum immunofixation, AChR antibodies, copper, ceruloplasmin, zinc, CBC, Lyme and West Nile virus serology, Anti GM-1 antibodies All normal except CK 432 ▫ 2nd level workup for LMN predominant ALS Genetic testing for SMA-IV - declined The Champ • Post script: ▫ 2nd opinion locally Suspicious for Kennedy disease – genetic testing negative ▫ 3rd opinion – secondary academic center LMN predominant ALS Enrolled in local ALS multidisciplinary center ▫ 4th opinion – tertiary academic center Noted upgoing right toe, maintained reflexes in atrophic limb Likely ALS Investigating clinical trials The Champ • Thank you!! The Champ • Bibliography ▫ ▫ ▫ ▫ ▫ ▫ ▫ ▫ ▫ ▫ ▫ Amato AA, Russel lJA. Approach to the Patient with Neuromuscular Disease. In: Amato AA, Russell JA (ed)., Neuromuscular Disorders., 1st edn. McGraw-Hill, New York, pp. 3-16. Belsh, J.M. and P.L. Schiffman, Misdiagnosis in patients with amyotrophic lateral sclerosis. Arch Intern Med, 1990. 150(11): p. 2301-5.Belsh, J.M. and P.L. Schiffman, The amyotrophic lateral sclerosis (ALS) patient perspective on misdiagnosis and its repercussions. J Neurol Sci, 1996. 139 Suppl: p. 110-6. Blexrud MD, Windebank AJ, Daube JR: Long-term follow-up of 121 patients with benign fasciculations, Ann Neurol 34(4):622–625, 1993 Brooks BR, Miller RG, Swash M, et al: El Escorial revisited: revised criteria for the diagnosis of amyotrophic lateral sclerosis, Amyotroph Lateral Scler Other Motor Neuron Disord 1(5):293–299, 2000. Chancellor, A.M., et al., The prognosis of adult-onset motor neuron disease: a prospective study based on the Scottish Motor Neuron Disease Register. J Neurol, 1993. 240(6): p. 339-46. Davenport, R.J., et al., Avoiding false positive diagnoses of motor neuron disease: lessons from the Scottish Motor Neuron Disease Register. J Neurol Neurosurg Psychiatry, 1996. 60(2): p. 147-51.de Carvalho, M., et al., Electrodiagnostic criteria for diagnosis of ALS. Clin Neurophysiol, 2008. 119(3): p. 497-503. Dumitru D, Zwarts MJ. Needle Electromyography. In: Dumitru D, Amato AA, Zwarts MJ, Electrodiagnostic Medicine, 2nd edn. Hanley & Belfus, Inc, Philadelphia, pp. 278-279. Gubbay SS, Kahana E, Zilber N, et al: Amyotrophic lateral sclerosis. A study of its presentation and prognosis, J Neurol 232(5):295–300, 1985. Brooks 2000 Haverkamp LJ, Appel V, Appel SH: Natural history of amyotrophic lateral sclerosis in a database population. Validation of a scoring system and a model for survival prediction, Brain 118(3):707–719, 1995. Misawa, S., et al., Ultrasonographic detection of fasciculations markedly increases diagnostic sensitivity of ALS. Neurology, 2011. 77(16): p. 1532-7. Rowland LP. Amyotrophic lateral sclerosis. In: Rowland, LP (ed), Merrit’s Textbook of Neurology, 9th edn. Williams and Wilkins, Baltimore, pp. 744-749.