Declaration of brain death checklist 11-2013
advertisement

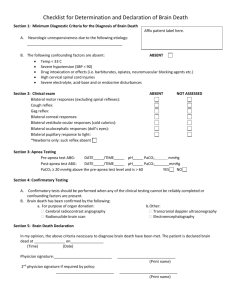
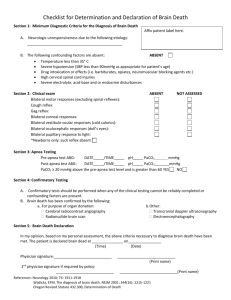
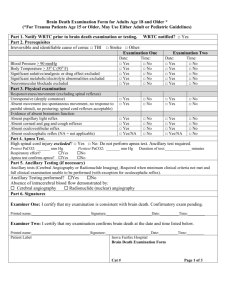
Checklist for Determination and Declaration of Brain Death Section 1: Minimum Diagnostic Criteria for the Diagnosis of Brain Death Affix patient label here. A. Neurologic unresponsiveness due to the following etiology: ______________________________________________ B. The following confounding factors are absent: ABSENT Temperature less than 36° C Severe hypotension (SBP less than 100mmHg as appropriate for patient’s age) Drug intoxication or effects (i.e. barbiturates, opiates, neuromuscular blocking agents etc.) Severe electrolyte, acid-base and or endocrine disturbances Section 2: Clinical exam Bilateral pupillary response to light: Bilateral corneal responses: Gag reflex: Cough reflex: Bilateral vestibulo-ocular responses (cold calorics): Bilateral oculocephalic responses (doll’s eyes): Bilateral motor responses (excluding spinal reflexes): *Newborns only: suck reflex absent ABSENT NOT ASSESSED Section 3: Apnea Testing Pre-apnea test ABG: DATE_____/TIME_____ pH_____ PaCO2__________ mmHg Post-apnea test ABG: DATE_____/TIME_____ pH_____ PaCO2_______mmHg PaCO2 ≥ 20 mmHg above the pre-apnea test level or ≥ 60 mmHg YES NO Section 4: Ancillary Testing Only one ancillary test needs to be performed; to be ordered only if clinical examination cannot be fully performed due to patient factors, or if apnea testing inconclusive or aborted. □ Radionuclide cerebral blood flow □ Transcranial Doppler study □ EEG □ Cerebral angiography □ CT angiogram Section 5: Brain Death Declaration I certify that the above tests have been performed. The patient is declared brain dead at _______________ on________________ (Time) (Date) Physician signature:____________________________ References: Neurology 2010; 74: 1911-1918 Oregon Revised Statute 432.300, Determination of Death ____________________________ (Print name) Revised 11-20-2013