Simple Approach to Heart Failure
advertisement

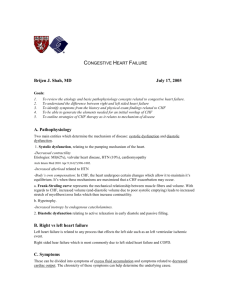
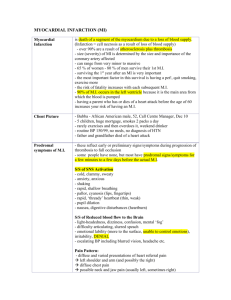
Optimizing Heart Failure Management 2005 Bridging the CARE GAP CME Needs of Family Physicians re CHF • • • • Early detection Etiology Prognosis Diagnosis – Physical exam – Asymptomatic LV dysfunction • How to use beta blockers – Which beta blocker – Better standardization of therapy • Rx titration – Diuretics – Beta blockers • Post hospital interventions – Lifestyle – Patient education • Diet • Rx • Exercise Rx • Compliance • Multi-system disease – Renal disease Measuring the Impact of HF • • • • • Currently, there are over 500,000 Canadians with HF Incidence 50,000 cases/year One year mortality after diagnosis ranges between 25-40% (ICES Atlas) 1% of Canadians over age 65 and 4% of Canadians over 70 have CHF The age-adjusted mortality for CHF is 106/100,000 Measuring the Impact of HF • Median survival currently 1.7 years for males, 3.2 yrs for females • 5-year age adjusted mortality rate of 45% based on the time period 1990-1999 • Commonest diagnosis that brings a patient to hospital for medical admission. • Re-admission rates are 46% within 3 months of discharge and 54% within 6 months. Heart Failure Epidemiology • Heart failure associated with high morbidity and mortality • Contemporary Canadian data to quantify the burden of CHF is limited • In 2000/01: – – – – – Total of 106,130 discharges for 85,679 CHF patients 32.7% of discharges were readmissions 19.9% of patients were re-hospitalized once or more during 2000 Total in-hospital mortality was 15.8%. CHF is associated with the second highest total number of hospital days and third highest number of patients affected. Can J Cardiol. 2003 Mar 31;19(4):436-8. Contemporary burden of illness of congestive heart failure in Canada. Tsuyuki RT, Shibata MC, Nilsson C, Hervas-Malo M. Contemporary burden of illness of congestive heart failure in Canada. Tsuyuki RT, Shibata MC, Nilsson C, Hervas-Malo M. “These figures should signal a call to action for researchers, administrators and health care providers regarding the need for more efficacious therapies, better application of already-proven therapies and patient education.” Can J Cardiol. 2003 Mar 31;19(4):436-8. Heart Failure is the Quintessential Disorder of Cardiovascular Aging • Convergence of – Age related changes in cardiovascular structure and function • Rising prevalence of – Hypertension – Coronary heart disease – Valvular heart disease Chronic Congestive Heart Failure Evolution of Clinical Stages NORMAL Asymptomatic LV Dysfunction No symptoms Compensated Normal exercise CHF Abnormal LV fxn No symptoms Decompensated Exercise CHF Abnormal LV fxn Symptoms Refractory Exercise CHF Abnormal LV fxn No symptoms Normal exercise Normal LV fxn Symptoms not controlled with treatment Ventricular Remodeling in CHF Jessup, NEJM 2003 Symptoms of HF • • • • • Fatigue Activity decrease Cough (especially supine) Edema Shortness of breath DIET Approach to the Patient With Heart Failure • Diagnose – Etiology – Severity (LV dysfunction) • Initiate – – – – Diuretic/ACE inhibitor -blocker Spirololactone Digoxin • Educate – – – – Diet Exercise Lifestyle CV Risk • Titrate – Optimize ACE inhibitor – Optimize -blocker Therapy of CHF Clinical Approach to CHF: Consider etiology Identify triggers Exclude ischaemia General measures Symptomatic therapy Prognostic therapy See Guide for HF Management Check-list Guide for HF Management Approach Recommendations Symptoms & Signs of HF: Fatigue (low cardiac output), SOB, JVP, rales, S3, edema, radiologic congestion, cardiomegaly. Elevated BNP. CXR to r/o infection, interstitial lung disease & PPH Ejection fraction (obtain echo or LV gated study) 40% = systolic dysfunction 40-55% = mixed systolic and diastolic dysfunction 55% = diastolic dysfunction - treat underlying disorder (HPT/ischaemia/pericardial constriction/restrictive CM (cardiomyopathy)/infiltrative disorders) Ischemic-CM HPT-CM Valvular HD-CM (AS/AR/MR) Metabolic: hyper/hypo thyroidism / hemochromatosis/pheochromocytoma Toxins: Alcohol/ anthracyclines/cocaine/amphetamines Viral CM Idiopathic Dilated CM Other: Consider etiology Identify triggers Acute-sudden onset Chronic-gradual onset Treatment: General measures Symptomatic therapy Therapy to improve prognosis Consider ACE-I/ARB combination in ACE-I and /or -blocked patients with worsening HF or hospitalization Caution:diabetics/renal disease/elderly/ NSAIDs & COX-2 inhibitors Anti-coagulant anti-platelet Rx Ischaemia, arrhythmia, infection, pulmonary embolism, acute valvular pathology Anemia, thyrotoxicosis, non-compliance, diet, Rx e.g. NSAID’s Correct triggers and precipitants of acute and chronic Heart Failure Low sodium diet D/C smoking Regular exercise/activity Treat lipid abnormalities Treat ischemia Treat and control diabetes Control hypertension Identify & Rx depression Diuretics-titrate to euvolemic state Maintain Ideal Body Weight (dry weight = JVP normal / trace pedal edema) Furosemide 20 - 80 mg OD-BID HCT/Zaroxolyn for refractory congestion Digoxin-for persisting symptoms in NSR (systolic dysfunction) or symptoms and rate control in Afib. Dose: 0.125 mg – 0.25 mg (Lower dose in elderly: 0.0625 mg) ACE Inhibitors-General Guideline: Trandolapril 1 4 mg mg OD‡ Start low and titrate to the target dose *Quinapril 10 mg 40 mg OD used in the clinical trials or the *Cilazapril 0.5 mg 10 mg OD MAXIMUM TOLERATED DOSE: *Fosinopril 5 mg 40 mg OD Captopril 6.25-12.5 mg *Perindopril 4 mg 8 mg OD 50 mg BID-TID *No large scale outcome trials Enalapril 2.5mg 10mg BID† † SoLVD/X-SoLVD § AIRE /AIREX‡TRACE Ramipril 2.5 mg 5mg BID § Consider ISDN 5-40mg QID+Hydralazine 10 Lisinopril 2.5 mg 30-40 mg OD 75mg QID for ACE-I/ARB intolerance VHeFT Angiotensin II receptor antagonists (ARB’s) ACE-Inhibitors remain first line therapy ARB’s indicated in ACE-I intolerant patients (CHARM candesartan 16-32 mg OD) (Val-HeFT /VALIANT valsartan 160 mg BID) Beta-blockers-Add Beta-blocker* to ACE-inhibitor/diuretic/+/- digoxin in stable Class II-IV CHF/LVEF 40% (*No outcome data for other beta-blockers) Bisoprolol* 1.25 10 mg OD (CIBIS II Trial) Carvedilol* 3.125 mg BID 25 mg BID (50 mg BID if weight > 85 kg) Metoprolol* 12.5 mg BID 75 mg BID (MERIT Trial) Aldosterone antagonist (follow K/Cr in 3-7 days/ furosemide to avoid azotemia) Spironolactone 12.5-25 mg OD added to ACE-inhibitor/diuretic/+/- digoxin in stable Class III-IV CHF/LVEF 35%/CR<220/K<5.0 (RALES Trial) ASA if CAD ( dose to ACE inhibitor interaction) Coumadin for Afib, LV thrombus, LVEF 20%, DVT or pulmonary embolism Duration of A/C therapy: Indefinite for Afib/recurring systemic TE or DVT/PE Consider Internal Medicine/Cardiology or Heart Failure Clinic referral for initiation/titration of - blocker. Consider EPS referral for symptomatic sustained or non-sustained ventricular arrhythmia (LVEF 30-40%) or AICD: Prior MI/CAD (LVEF 30% with IVCD 0.12 sec: MADIT II) CHF: (NYHA II-III & LVEF <35% SCD-HeFT) Cardiac Resynchronization Therapy(CRT):(NYHA Class III-IV with reduced ejection fractions; LVEF < 35%; QRS duration 0.13 with IVCD or LBBB: MIRACLE / MUSTIC) or both CRT/AICD: (NYHA III-IV;QRS 0.12:COMPANION). EECP/Transplant for refractory CHF. Symptoms & Signs of HF: • • • • • • • • Fatigue (low cardiac out-put) SOB JVP Rales S3 Edema Radiologic congestion Cardiomegaly Obtain CXR to r/o non-cardiac causes e.g. interstitial lung disease & PPH BNP in the Diagnosis of HF The role of natriuretic peptides • ANP-atrial natriuretic peptide – Produced in atria in response to wall stress • BNP-brain natriuretic peptides – Produced in ventricles in response to volume and pressure overload • CNP-central nervous system and endothelium – Produced in response to endothelial stress • Produced as prohormones and cleaved to active molecule (ANP/BNP)and inactive NT forms BNP in the Diagnosis of HF ANP/BNP elevated in • • • • • • • • Heart failure Systemic and pulmonary hypertension Hypertrophic and restrictive cardiomyopathy Pulmonary embolism COPD Cor pulmonale AMI Cirrhosis Renal Failure BNP in the Diagnosis of HF Higher levels of BNP correlate with • higher PCW pressures – in compensated and decompensated patients • larger LV volumes • lower ejection fractions – in symptomatic HF patients • BNP study (Circ 2002;106: 416-422) – BNP sensitivity 90% and specificity 73% for HF BNP Diagnostic Cut Points for CHF JACC 2001;37(2):379-85. BNP > 400 pg/L – acute CHF present BNP 100 pg/L – 400 pg/L • Diagnostic of CHF with – – – – Sensitivity 90% Specificity 76% Predictive accuracy 83% R/O pulmonary embolism, LV dysfunction without acute CHF or cor pulmonale BNP < 100 pg/L – 98% negative predictive accuracy Identify triggers Acute-sudden onset • Ischaemia • Arrhythmia • Infection • Pulmonary embolism • Acute valvular pathology Chronic-gradual onset • Anemia • Thyrotoxicosis • Non-compliance • Diet • Rx e.g. NSAID’s Non-Invasive Evaluation of the Heart Failure Patient-Implications of LV Ejection Fraction • To know where you are going you must know where you are coming from • Evaluate LV function clinical echo gated study Ejection fraction (obtain echo or LV gated study) • LVEF 40% = systolic dysfunction • LVEF 40-55% = mixed systolic and diastolic dysfunction • LVEF 55% = diastolic dysfunction identify triggers – treat underlying disorder (HPT/ischaemia/pericardial constriction/restrictive CM/infiltrative disorders) Echocardiographic Evaluation of CHF • LV function (EF),chamber size,wall motion • Segmental dysfunctioncoronary disease • MS-severity, valve area • AS- valve gradient, valve area • AR/MR severity • TR- RV systolic pressure = PA pressure • • • • RV function R/O IHSS, HCM R/O Pericardial Disease R/O rare causes e.g. myxoma, infiltrative disorders- restrictive cardiomyopathy • Diastolic function • Hyperdynamic states Diastolic Dysfunction • 30-50% of elderly HF patients have reserved LV systolic function • Diastolic dysfunction may induce dyspnea on exertion • Frank congestion usually has identifiable precipitant Clinical Implications of LV Dysfunction in Heart Failure • Calculated EF by echo unreliable in remodeled LV • Visual estimate of EF semi-quantitative • (CCN LV function scale) – – – – Grade I LV EF ≥50% Grade 2 LVEF 35-49% Grade 3 LVEF 20-34% Grade 4 LVEF< 20% LVEF Entry Criteria in ACE inhibitor and -blocker Trials – SOLVD treatment an prevention 35% – SAVE (post MI) 40% – U.S. Carvedilol HF Trials Program LVEF 35% – Merit-HF LVEF 40% – CIBIS II LVEF 40% Consider etiology • • • • Ischemic- Cardiomyopathy (CM) HPT-CM Valvular HD-CM (AS/AR/MR) Metabolic: / thyroid/hemochromatosis/ pheochromocytoma • Toxins: Anthracyclines/Etoh/cocaine/amphetamines • Viral CM • Idiopathic Dilated CM • Other: Treatment General Measures General measures: • Correct triggers and precipitants of acute and chronic HF • Low sodium diet • Fluid restriction • Regular exercise/ • Activity HR Rx • • • • Treat ischemia Control hypertension D/C Smoking Treat lipid abnormalities • Treat and control diabetes • Identify & Rx depression HF Management Algorithm Is it Heart Failure? Symptoms & Signs YES Diagnostic Tests: CXR/ECG/±BNP Additional Tests ±Specific Tx •Cath •CABG •Valve Sx YES Echo/RNA/MRI: Etiology/Severity Systolic HF: Medical±Sx/Device Life Style + Patient Education ± HF Clinics F/U Diastolic HF: Rx cause±Referral Primary Targets of Treatments in CHF Jessup, NEJM 2003 Symptoms Prognosis & Symptoms Assess LV Function (echo, gated RNA) •EF < 40%-systolic dysfunction •EF 40-55%-systolic/diastolic dysfunction •EF >55%-diastolic dysfunction Assess Volume Status Signs and Symptoms of Fluid Retention Loop Diuretic +/- Thiazide (titrate to euvolemic state) Add Digoxin for symptom control No Signs and Symptoms of Fluid Retention ACE inhibitor/ARB if ACE intolerant Combination Rx if HF, hospitalization or -blocker intolerant -blocker (NYHA II-IV) Spironolactone (NYHA Class III-IV CHF/EF<35%/Cr<200/K<5) Heart Failure Therapeutic Goal • Mild-Moderate Heart Failure – Primary goal = Reduce mortality – -blockers + ACE inhibitors – Prevent progression to symptoms – Prevent progressive LV dysfunction Heart Failure Therapeutic Goal • Moderate-Severe Heart Failure – Primary goal = Reduce symptoms – Improve quality of life (QOL) – Reduce hospitalizations – Prevent sudden death General Rx Strategies in HF Asymptomatic Mild/Mod Severe Refractory Inotropes, mitral repair, VAD, Tx Correct Cause: Arrhythmias Ischemia Pressure Load Tailored Rx Digoxin Diuretics (Spironolactone) Carvedilol/ -Blockers Angiotensin Converting Enzyme Inhibitors No Added Salt Activity as Tolerated Modified from Warner-Stevenson, ACC HF Summit 2 gm Na Customized Ex Training Symptomatic therapy Diuretics (see How to Adjust Your Diuretic) • Titrate to euvolemic state • Maintain Ideal Body Weight – (dry weight = JVP normal / trace pedal edema) • Furosemide 20 mg. – 80 mg OD-BID • HCT/Zaroxolyn for refractory congestion Digoxin • For persisting symptoms in NSR (systolic dysfunction) • or symptoms and rate control in Afib. Dose: 0.125 mg – 0.25 mg (Lower dose in elderly: 0.0625 mg) The Effect of Digoxin on Mortality and Morbidity in Patients with Heart Failure 1 Digitalis Investigation Group (DIG Trial) - a large simple, long-term trial Sponsored by the National Heart, Lung, and Blood Institute and Department of Veterans Affairs Cooperative Studies Program NEJM Volume 336:525-533 February 20, 1997 Number 8 DIG Trial 13 DIG: All Cause Deaths 50 50 40 40 Percent Event Percent Mortality 15 DIG: CHF Mortality or Related Hospitalizations 30 20 Placebo p = 0.80 10 Digoxin 30 Placebo 20 10 Digoxin 0 0 4 8 12 16 20 24 28 Months 32 36 40 44 48 p = 0.0001 52 0 0 4 8 12 16 20 24 28 Months 32 36 40 44 48 52 DIG Trial 16 DIG: CHF Mortality or Related Hospitalizations Harm Benefit EF Prev Dig Use CT Ratio < 0.55 > 0.55 NYHA Class • Reduced worsening heart failure deaths Yes No IHD Non-IHD • Reduced worsening heart failure hospitalizations I/II III/IV Overall 0.25 DIG: Conclusions • No effect on overall survival 25 -45 < 25 Etiology 20 0.5 0.75 (Risk Ratio: Active/Control) 1 1.25 • Small absolute excess in digoxin toxicity ACE Inhibitors are the Cornerstone of Rx in CHF CCS 2003 Consensus HF Update (draft) • ACE I Rx ASAP post MI – Continue indefinitely if EF < 40% or clinical HF – Rx for all asymptomatic patients with LVEF 35% – Rx for all symptomatic patients with LVEF 35% – Target dose use in clinical trials or max tolerated dose ACE Inhibitors in CHF Study No. Males Age EF% Class Drug F/U V-HeFT 642 100% 58 30 II.III CONCENSUS 253 70% 70 NA IV HDZN/ ISDN Enalapril V-HeFT II 804 100% 61 29 II,III Enalapril SOLVD Treatment SOLVD Prevention 2569 80% 61 25 II,III Enalapril 4228 89% 59 28 I,II Enalapril 2.3 yrs. 188 Days 2.5 yrs. 41.4 mo. 37.4 mo. Mortality Reduction % 11 27 14 16 8 ACE Inhibitors Post MI Trial No. SAVE CONCENSUS II AIRE GISSI 3 ISIS 4 TRACE Chinese study SMILE 2231 6090 2006 20,000 60,000 1749 10,000 1556 Entry Criteria EF<40% ALL CHF All All LVD All AWMI Drug Captopril Enalapril Ramipril Lisinopril Captopril Trandolapril Captopril Zofenopril Initiation Period 3-16 days <24 hours 3-10 days < 24 hours 24 hours 3-7 days < 36 hours < 24 hours F/U Period 2-5 years 1.5-6 months 6-30 months 6 weeks 5 weeks 2-4 years 5 weeks 5 weeks Effect on Mortality + + + + + + + Overview of Long Term ACE Inhibitor Trials Showing Mortality Benefit Study SOLVD Number Criteria RRR % ARR % NNT Lives saved/1000 2569 LVEF 35% 16 4.5 22 50 SAVE 2231 19 4.2 24 45 AIRE 2006 LVEF 40% Clinical CHF 27 5.7 18 60 TRACE 1749 LVEF 35% 22 7.6 13 90 Treatment What’s New in Ace inhibition in HF Long Term Follow-up X-SOLVD Effect of Enalapril on 12-Year Survival and Life Expectancy in Patients with Left Ventricular Systolic Dysfunction X-SOLVD Investigators Philip Jong,* Salim Yusuf,* Michel F. Rousseau,** Sylvie A. Ahn,** Shrikant I. Bangdiwala*** *Population Health Research Institute, McMaster University - Hamilton, Canada **Division of Cardiology, University of Louvain - Brussels, Belgium ***Collaborative Studies Coordinating Center, University of North Carolina - Chapel Hill, USA SOLVD D LV Mortality SO X SOLVD Prevention SOLVD Treatment 0.5 2P=0.0072 at 4 years 30 HF Development 0.3 0.3 0.2 0.2 0.1 0.1 Relative Risk 0.63 (95% CI 0.56-0.72) p<0.001 at 4 years 35 0.4 Mortality 0.4 Development in Prevention Trial 40 0.5 2P=0.30 at 4 years Mortality D LV HF SO X in SOLVD Trials 25 20 15 10 Enalapril (n=399) Placebo (n=436) 0.0 Enalapril (n=299) Placebo (n=333) 0.0 0 1 2 3 4 Years after Randomization 0 1 2 3 4 Years after Randomization Adapted from: The SOLVD Investigators. N Engl J Med 1992;327:685-691 & N Engl J Med 1991;325:293-302. Enalapril (n=438) Placebo (n=640) 5 0 0 6 12 18 24 30 36 Months after Randomization Adapted from: The SOLVD Investigators. N Engl J Med 1992;327:685-691. 42 48 X-SOLVD D LV Cumulative 12-Year SO X in Prevention Trial Trial Termination 0.86 0.9 Enalapril Placebo 5-year 0.77 0.8 0.84 0.7 0.73 0.6 In-Trial Period 0.5 0.47 (n=319) 0.4 0.41 (n=297) 0.3 0.2 Enalapril Placebo 0.9 0.8 0.7 0.64 5-year 0.53 0.6 In-Trial Period 0.5 p=0.01 at 12 years 0.60 0.4 0.49 0.21 (n=153) 0.3 0.2 p=0.001 at 12 years 0.1 Survival Trial Termination 1.0 Proportion of Survivors 1.0 Proportion of Survivors D LV Cumulative 12-Year SO X in Treatment Trial Survival 0.20 (n=151) 0.1 0.0 0.0 0 1 2 3 4 5 6 7 8 9 10 11 12 Years after Randomization Number at Risk Enalapril 2111 Placebo 2117 1917 1901 1736 1664 1533 1457 Adapted from Jong et al. Lancet 2003;361:1843-1848. 1348 1252 0 1 2 3 4 5 6 7 8 9 10 Years after Randomization 11 12 Number at Risk 1010 935 319 297 Enalapril Placebo 1285 1284 1009 940 785 719 Adapted from Jong et al. Lancet 2003;361:1843-1848. 612 562 454 425 346 328 153 151 Optimal Dosing of ACE Inhibitors • General Guideline: • Start low and titrate to the target dose used in the clinical trials or the MAXIMUM TOLERATED DOSE (ATLAS trial) • Captopril 6.25-12.5 mg 50 mg BID-TID (SAVE) • Enalapril 2.5 mg BID 20 mg BID (SOLVD/X) • Ramipril 2.5 mg BID 5 mg BID (AIRE/EX) • Lisinopril 10 mg OD 30-40 mg OD (GISSI 3) • Trandolapril 1mg 4 mg (TRACE) Summary – ARBs in CHF # pts. ELITE II Val-HeFT VALIANT CHARM ARB vs ACEI ARB vs placebo ( ACEI BB) Captopril, Valsartan or Combination ARB vs placebo ( ACEI) 3,152 5,010 4909/4909/4885 7,601 Symptomatic HF Class II-III/ clinical or radiologic LV function/preserved LVF (added+alternative/preserved) HF Population Heart failure Heart failure Post MI with Endpoints 1o All-cause mortality, sudden death or resuscitated cardiac arrest: NS 1o All-cause mortality: NS 1o All-cause mortality: NS 2o CV Death, MI, or HF:NS 1o All-cause mortality: NS Valsartan noninferior to Captopril –ACEI+ARB = -15% 1o Combined M/M: ACEI+ARB = 13.2% ACE intolerant: -33% all cause mortality 2o CV death or HF hospitalization: •CHARM Added: •CHARM Alternative: –ARB = -30% •CHARM Preserved: NS Combined Morbidity/Mortality in Subgroups: Val-HeFT All Demographics < 65 65 Male Female Favors valsartan No. patients 5010 Favors placebo 2660 2350 4007 1003 Etiology/Co-morbidity IHD (yes) 2865 IHD (no) 2145 Diabetes (yes) 1276 Diabetes (no) 3734 Disease Severity NYHA II NYHA III/IV EF 27 EF < 27 LVIDD < 3.57 LVIDD 3.57 3095 1910 2623 2385 2505 2505 0.4 Cohn JN, et al: Val-HeFT NEJM December 2001 0.6 0.8 1.0 1.2 1.4 Mortality in SAVE, TRACE, AIRE, and VALIANT Hazard Ratio for Mortality SAVE TRACE Valsartan preserves 99.6% of mortality benefit of captopril, representing a 25% RR AIRE Combined VALIANT (imputed placebo) 0.5 Favors Active Drug Pfeffer M et al. N Engl J Med 2003;349:1893-906 1 Favors Placebo 2 CHARM Programme Mortality and morbidity All Cause Mortality 0.77 Alternative p=0.0004 0.85 Added p=0.011 0.89 Preserved Overall CV Death or CHF Hospitalisation p=0.118 0.91 p=0.055 0.7 0.8 0.9 1.0 1.1 1.2 Hazard ratio p heterogeneity=0.37 0.84 p<0.0001 0.6 0.7 0.8 0.9 1.0 1.1 1.2 Hazard ratio p heterogeneity=0.43 Evidence for Various ARBs Diovan (valsartan) Avapro (irbesartan) Cozaar (losartan) Atacand (candesartan cilexetil) Micardis (telmisartan) Teveten (eprosartan) -45% -6% -35% -30% N/a N/a Heart failure hospitalizations -27.5% (ValHeFT) N/a -8.1% (ELITE II) -17% (CHARM) N/a N/a CV outcome in CHF-treated patients -13.3% (ValHeFT) N/a +7% (ELITE II) -15% (CHARM) N/a N/a Positive CV outcomes in CHF Yes N/a No Yes N/a N/a Equivalent Efficacy to ACEi post MI Yes N/a No N/a N/a N/a Reduction in microalbuminuria with starting dose -Blocker Saves Lives in Heart Failure? –blocker is the most important progress in Heart Failure Rx in the last 5 years HF Trials Modulating receptors Trial US US Carvedilol Carvedilol Aus-NZ CIBIS II MERIT COPERNICUS COPERNICUS HF Pts II-III II EF<35% EF<40% EF<25% N Rx RR 1,094 Carvedilol 0.35 415 Carvedilol 0.74 2,647 Bisoprolol 0.66 3,991 Metopr-CR 0.66 2,289 Carvedilol 0.65 Background Rx = ACEi + Diuretics +/- Digoxin Number Need to Rx in HF TRIAL Therapy Enalapril vs. Plac Metoprolol MERIT vs. Plac Bisoprolol CIBIS-2 vs. Plac COPERN Carvedilol ICUS vs. Plac Spiro vs. RALES Placebo SOLVD Lee, Liu, Packer Annual Annual Absolute NNRx/year Mortality- Mortality- Risk to Save Placebo Treatment Reduc’n One Life 12.5% 11.2% 1.3% 77 11.0% 7.2% 3.8% 26 13.2% 8.8% 4.4% 23 18.5% 11.4% 7.1% 14 22.5% 15.8% 6.7% 15 -adrenergic Blocking Agents • Titrate to target dose – Bisoprolol 1.25 -10 mg OD – Carvedilol 3.125 - 25 mg BID – Metoprolol 12.5 - 50 to75 mg /BID • If unable to tolerate high dose -blocker maintain highest tolerated dose • Continue indefinitely Patient Selection for Successful - Blocker Initiation • • • • Stable symptoms Stable background heart failure medications No recent CV hospitalization Stable CV status (no hypotension or bradycardia) • Euvolemic status • Start low and titrate slowly Patients With Heart Failure Who Should Not Be Started on -blockers • General Contraindications – Bronchospastic pulmonary disease – Severe bradycardia, high degree AV block, sick sinus syndrome • Heart Failure Considerations – Congestive symptoms at rest (NYHA Class IV) – Patients who require intravenous therapy for HF – Unstable symptoms or recent changes in background medications – Hospitalized patients (especially for worsening HF) RALES Trial • Spironolactone 12.5-25 mg OD added to ACE-inhibitor/diuretic/+/- digoxin in stable Class III-IV CHF/LVEF 35%/CR<220/K<5.0 • 30% RRR in death from progressive HF and sudden cardiac death • 35% reduction in hospitalization for worsening HF • NEJM Volume 341:709-717 Number 10 RALES Caveats • With aldosterone antagonist follow K/Cr in 3-7 days – furosemide to avoid azotemia • Inadequate follow-up can lead to increased rates of hospitalization for hyperkalemia and associated mortality – NEJM Volume 351:543-551 Number 6 • Caution: – – – – – Diabetics Renal disease Elderly NSAIDS COX-2 inhibitors Severity of Heart Failure Modes of Death NYHA II 12% 24% 64% NYHA III CHF CHF Other 26% Sudden Death 59% 15% n = 103 Other Sudden Death n = 103 NYHA IV CHF 33% 11% Other 56% Sudden Death n = 27 MERIT-HF Study Group. LANCET 1999;353:2001-07. Therapies Provided by Today’s Dual-Chamber ICDs Atrium AT/AF tachyarrhythmia detection Antitachycardia pacing Cardioversion Ventricle Atrium & Ventricle VT/ VF detection Bradycardia sensing Antitachycardia pacing Bradycardia pacing Cardioversion Defibrillation Evaluate for Implantable Devices Consider EPS Referral VT: • Symptomatic sustained or non-sustained ventricular arrhythmia (LVEF 30-40%) AICD: • Prior MI/CAD (LVEF 30% with IVCD 0.12 sec: MADIT II) or both CRT/AICD(NYHA III-IV;QRS 0.12:COMPANION). • CHF: (NYHA II-III & LVEF < 35% SCD-HeFT) Cardiac Resynchronization Therapy (CRT): • (NYHA Class III-IV with reduced ejection fractions; LVEF < 35% • QRS duration 0.13 with IVCD or LBBB: MIRACLE / MUSTIC) Sudden Cardiac Death-Heart Failure SCD-HeFT Hypothesis and Primary Endpoint • To determine, by intention-to-treat analysis, if amiodarone or a conservatively programmed shock-only single lead ICD reduces all-cause mortality compared to placebo* in patients with either ischemic or non-ischemic NYHA Class II and III CHF and EF < 35%. • Good background Therapy – ACE or ARB 87% – -blocker 78% Bardy G et al. NEJM 2005; 352:3 Sudden Cardiac Death SCD-HeFT Heart Failure Trial *Double-blind for drug therapy Enrollment Scheme DCM + CAD and CHF EF < 35% NYHA Class II or III 6 minute walk, Holter R Bardy G et al. NEJM 2005; 352:3 Sudden Cardiac Death SCD-HeFT Heart Failure Trial Placebo Amiodarone ICD Kaplan-Meier Estimates of Death from Any Cause Sudden Cardiac Death SCD-HeFT Heart Failure Trial Bardy G et al. NEJM 2005; 352:3 Kaplan-Meier Estimates of Death from Any Cause: Ischemic CHF Sudden Cardiac Death SCD-HeFT Heart Failure Trial Non-Ischemic CHF Bardy G et al. NEJM 2005; 352:3 Hazard Ratios for the Comparison of Amiodarone and ICD Therapy with Placebo Sudden Cardiac Death SCD-HeFT Heart Failure Trial Bardy G et al. NEJM 2005; 352:3 SCD-HeFT: Primary Conclusions 1. In class II or III CHF patients with EF < 35% on good background drug therapy, the mortality rate for placebo-controlled patients is 7.2% per year over 5 years 2. Simple, single lead, shock-only ICDs decrease mortality by 23% 3. Amiodarone, when used as a primary preventative agent, does not improve survival Sudden Cardiac Death SCD-HeFT Heart Failure Trial Bardy G et al. NEJM 2005; 352:3 Cardiac Resynchronization Therapy (CRT) • Atrial-biventricular stimulation • Electrical synchronization narrower QRS • Mechanical synchronization reverse remodeling Resynchronization/Defibrillation for Advanced Heart Failure Trial RAFT Hypothesis: In patients with LV Dysfunction (EF 30%) and QRS duration 120 ms with moderate to severe CHF symptoms, the addition of Cardiac Resynchronization Therapy (CRT) to Implantable Cardioverter Defibrillator (ICD) and optimal medical therapy reduces the combined end point of mortality and CHF hospitalization. RAFT - Design • Randomized Controlled Trial: – ICD vs CRT/ICD • Blinding – Patient, HF Care (Blinded) – Device care (Un-blinded) • Patients randomized to a 1:1 proportion to: – ICD (Single or Dual) or – CRT/ICD • Stratified for: Center & AF & Single/Dual ICD indication RAFT Inclusion Criteria • NYHA Class II or III • QRS duration 120 ms or Paced QRS 200 ms • LVEF 30% by MUGA or LVEF 30% and LVEDD > 60mm by echocardiogram within 6 months of randomization • ICD indication: 1° or 2° prevention • Optimal Heart Failure Pharmacotherapy • Normal sinus rhythm or Chronic persistent atrial tachyarrhythmia with resting ventricular Heart Rate of ≤ 60 bpm and ventricular rate ≤ 90 bpm during a 6 minute hall walk or Chronic persistent atrial tachyarrhythmia with resting ventricular Heart Rate of >60 bpm and ventricular rate > 90 bpm during a 6 minute hall walk and booked for an AV junction ablation *NYHA Class II: Slight limitation of physical activity. Comfortable at rest, but ordinary physical activity results in fatigue or dyspnea ** NYHA Class III: Marked limitation of physcial activity. Comfortable at rest, but less than ordinary activity causes fatigue or dyspnea. RAFT Exclusion Criteria • In-hospital patients who have an acute cardiac or noncardiac illness that requires intensive care • Intra-venous inotropic agent 4 days prior to randomization • Expected to undergo cardiac transplantation within one year (status I) • Coronary revascularization (CABG or PCI) < 1month • Acute coronary syndrome(including MI) < 4 weeks • Patients with an existing ICD (Patients with an existing pacemaker may be included if the patient satisfies all other inclusion/exclusion criteria) • Uncorrected or uncorrectable primary valvular disease • Restrictive, hypertrophic or reversible form of cardiomyopathy RAFT Exclusion criteria cont’d • Patients with a life expectancy of less than one year from noncardiac cause. • Patients included in other clinical trial that will affect the objectives of this study • Unable or unwilling to provide informed consent • History of noncompliance of medical therapy • Severe primary pulmonary disease such as cor pulmonale • Tricuspid prosthetic valve Heart Failure Management Issues • • • • • • • High Mortality High re-admission rates Poor understanding of disease Poor Rx adherence On-going symptoms Reduced Quality of Life Dose Adjustments in the Elderly Adherence Gap • • • • • • • Cost of medications Complacency-patient and physician Side effects Lack of understanding Infrequent monitoring intervals Lack of reinforcement Lack of feedback Adherence Strategies • • • • • • Patient education materials Medication monitoring strategies Pharmacy patient surveillance Follow-up protocols Role of Public Health nurses Patient Awareness Initiatives – Out-patient Heart Failure Education Programs CHF Implementation Targets • Heart Failure Specialists • General Cardiologists – Academic/Community • Internists – Academic/Community • • • • • Family Physicians Hospital Nursing staff Public Health Nurse Residents & Housestaff General Public How can we amplify the impact of HF therapy? Inotropes,Devices Transplant 4º Specialist/Cardiologist HF Clinic 2º & 3º Dosing Optimization- Family MD & Specialist 1º & 2º Recognition-Initial TherapyFamily MD Primary Care Physician Community Based Awareness/Understanding HF Awareness Program/PHN Heart Failure Network • • • • • • • Apically connected tertiary centres Vertically integrated local networks Laterally integrated at all levels Regional centres linked to local specialist Hubs of resources dissemination Shared resources/minimize duplication Common denominator is primary care physician/patient base Heart Failure Networks Lateral Integration Role of Heart Failure Clinics • 4º and 3º Heart Failure Clinics – – – – – – Pre-transplant work-up Out-patient parenteral inotropic therapy Patient education High risk rehabilitation programs Regional hubs- national Heart Failure Network Co-ordinating centre-Heart Failure Network data-base Role of Heart Failure Clinics • 2º hospital based and community based Heart Failure Clinics/Disease Management Programs – – – – – – Patient identification and risk assessment Patient education Rx titration and fluid status monitoring Low risk and intermediate risk exercise programs Primary care liaison, education Long term follow-up Role of Primary Care Physician • • • • Patient identification Assess etiology Assess LV Function Initial stabilization of acute HF – Rx initiation and titration (diuretics/ACEinhibitor/digoxin) • Optimize ACE inhibitors • Rx -blocker if comfortable with Rx • Patient education • Treatment integration • Long term follow-up Role of Public Health Nurse • • • • Patient education Patient monitoring Adherence Follow-up Role of the Public • • • • • Awareness Initiate contact Understanding Lifestyle & diet modification Compliance Goals & Outcomes • Improve symptoms • Improve quality of life • Prevent progression of LV dysfunction • Reduce hospitalization and morbidity • Reduce mortality – Progression of HF – Sudden death