MELIDIOSIS - Medico Tutorials
advertisement

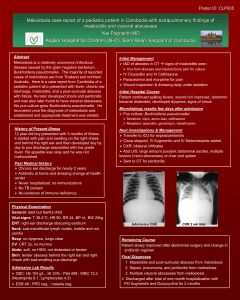
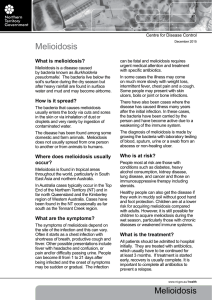
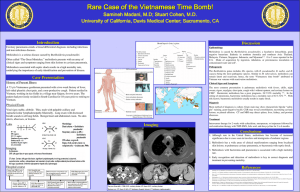
Melioidosis. Burkholderia pseudomallei Dr.T.V.Rao MD Burkholderia pseudomallei Melioidosis. Burkholderia pseudomallei causes an infectious disease called melioidosis. This bacteria is most commonly found in Southeast Asia, especially in Thailand and in Northern Australia. It was first discovered in Australia in far northern Queensland in 1962, but has now spread progressively to the west and south. What is Melioidosis? Melioidosis, also called Whitmore's disease, is an infectious disease caused by the bacterium Burkholderia pseudomallei. Melioidosis is clinically and pathologically similar to glanders disease, but the ecology and epidemiology of melioidosis are different from glanders. An environmental Bacteria Burkholderia pseudomallei is found in the soil, rice paddies, and muddy waters of these areas. Polluted and contaminate atmosphere contributes for spread Spread of B.pseudomallei Infections B.pseudomallei is a facultative intracellular pathogen. It is pathogenic because of its ability to invade, resist factors in serum, and survive intracellularly. It is easily contracted by inhaling dust containing the bacteria or by having contact between contaminated soil and cuts or scrapes of the skin How Melidiosis is spread Humans and animals, like sheep, goats and horses are believed to acquire the infection by inhalation of dust, ingestion of contaminated water and contact with contaminated soil especially through skin abrasions. Melioidosis can also spread from person to person by contact with the body fluids of an infected person. Human Infections initiated Human infections are initiated with contamination of skin abrasions. By Ingestion By inhalation. Morphology B.pseudomallei is a small, motile, aerobic Gram –ve Grows on standard bacteriological medium The colines vary from muciod and smooth to rough wrinkled. The color of the colonies vary from cream to orange. Grows at even 420c Can be Epizootic Infection Sheep, horses, Goats, swine, can harbor the infection However animals are unlikely to be primary reservoirs of infection It is a gram negative bacteria with a safety pin like appearance. Growth on Standard Medium Grows on Standard Bacteriological media, colonies become rough and wrinkled on prolonged incubation Colonies of B.pseudomallei on Ashdown media Ashdown's medium is a selective culture medium for the isolation and characterisation of Burkholderia pseudomallei. the medium contains crystal violet and Gentamycin as selective agents to suppress the growth of other bacteria. Colonies of B. pseudomallei also take up neutral red which is present in the medium, Ashdown's agar needs to be incubated for a minimum of 96 hours instead of 48 hours. Pathogenesis The disease can manifest as Acute, Sub acute, and Chronic disease Incubation may be as short as 2 – 3 days Latent infections can occurs after months to years Progress of Infection The infection starts with non specific lesion at the inoculum, where there can be break in the skin. Lead to septicemia Most common form is pulmonary infection Can lead to suppurative infection and bacterimia Respiratory Infection The most dangerous infection can be associated with respiratory infection Can lead to suppurative lesions. Consolidations of upper lobe of the lung Can mimic tuberculosis. Progressive illness can produce cavities Spreading lesions Systemic infections spread from the primary lesions on the skin. Can spread to lungs, Myocardium, Liver and Bone. Can present with unexplained systemic disease. Latent Infection in Melidiosis The latent infection can reactivate as result of immuno supression A high level of suscipicion in endemic areas is gratifying. Any unexplained clinical symptoms and signs should be explored for infections. Who are at risk Individuals with diabetes are at a higher risk for contracting melioidosis. About 40% of meliodiosis patients are diabetic. Other factors that may increase the risk of contracting meliodiosis are excessive alcohol consumption, chronic renal disease, and chronic lung disease. However, even though these factors do increase the risk of contracting melioidosis, cases of infection can still occur in healthy adults and children occasionally. Clues to Respiratory infection Pulmonary infection: This form of the disease can produce a clinical picture of mild bronchitis to severe pneumonia. The onset of pulmonary melioidosis is typically accompanied by a high fever, headache, anorexia, and general muscle soreness. Chest pain is common, but a nonproductive or productive cough with normal sputum is the hallmark of this form of melioidosis. Immuno supression can be leading cause Acute bloodstream infection: Patients with underlying illness such as HIV, renal failure, and diabetes are affected by this type of the disease, which usually results in septic shock. The symptoms of the bloodstream infection vary depending on the site of original infection, but they generally include respiratory distress, severe headache, fever, diarrhea, development of pus-filled lesions on the skin, muscle tenderness, and disorientation. This is typically an infection of short duration, and abscesses will be found throughout the body. Diagnosis Melioidosis is diagnosed by isolating Burkholderia pseudomallei from the blood, urine, sputum, or skin lesions. Detecting and measuring antibodies to the bacteria in the blood is another means of diagnosis Bacteriological Diagnosis Gram stain of the material from skin lesions, sputum. Small gram-ve bacilli with specific Bipolar staining can be leading clue. In all suspected cases staining with Wright's stain and methylene blue Serology Strains of B.pseudomallei are identified serologically by agglutination tests, rapid slide or tube agglutination Recently ELISA based on monoclonal antitoxin is avialble for rapid diagnosis in endemic areas of melioidosis. Treatment As the disease carries high mortality, a prompt and effective treatment is highly essential A surgical drainage of organized surgical lesions. Tetracyclnes, Sulfonamides, TrimethoprimSulphmethoxazole are effective. Ceftazidime is highly effective Duration of Antibiotic Treatment The duration of treatment should lost at least 8 weeks. The treatment lasting 6moths to 1 year are considered in immunosuppressive conditions. No Vaccines are available Bio Hazard and B.pseudomallei Human laboratory acquired infection with, B.pseudomallei and P.mallei is a hazard Both organisms are included in category A pathogen. Included in category 3 and to be handled with greatest care and strict and designated isolation conditions. Created for Medical and paramedical students in Developing world Dr.T.V.Rao MD Email doctortvrao@gmail.com