Aspirin - Learnblock
advertisement

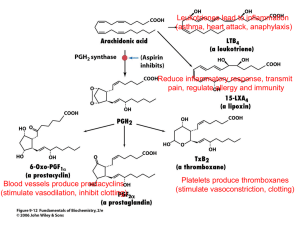
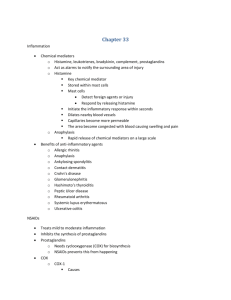
COMMONWEALTH OF AUSTRALIA Copyright Regulations 1969 WARNING This material has been copied and communicated to you by or on behalf of the University of Sydney pursuant to Part VB of the Copyright Act 1968. (The Act). The material in this communication may be subject to copyright under the Act. Any further copying or communication of this material by you may be the subject of copyright protection under the Act. Do not remove this notice. NSAIDs Thomas Grewal Ph.D. thomas.grewal@sydney.edu.au Room N518 (with kind permission of A/Prof Alaina Ammit) Lecture 1: NSAIDs – Mechanism of Action Lecture 2: NSAIDs – COX-1/2 vs COX-2 inhibitors Further reading Title: Foye’s Principals of Medicinal Chemistry Editors: D.A. Williams, T.L. Lemke Publisher: Philadelphia, Lippincott Williams & Wilkins, 2008 Edition: 6th ed. Lecture 1 NSAIDs – Mechanism of Action Learning objectives: • Nonsteroidal anti-inflammatory drugs: a definition • Inflammation in health and disease • Focus on prostanoids: – Role in inflammation – Structure and biosynthesis • COX enzymes – Role in production of prostanoids – Similarities and differences between isozymes COX-1 and COX-2 – Physiological role of COX-1 and COX-2 NSAIDs: Best Sellers • NSAIDs most commonly prescribed medication – 70 million prescriptions/year (US), $ 6.8 billion worldwide, – Use and cost is likely to increase with longer life expectancy • Approximately 50 NSAIDs available, among the most commonly prescribed drugs • UK - 18.5 million prescriptions are written for NSAIDs each year at a cost of £170 million (not including OTC) • Aspirin is consumed in very high amounts (worldwide production of > 50,000 tons/year) • US - COX-2 inhibitors, rofecoxib (Vioxx) and celecoxib (Celebrex), > US $4 billion in 2000 NSAIDs • NSAIDs do not reverse the course of disease, but treat the symptoms: pain, fever and inflammation in many inflammatory disorders • Heterogenous group of compounds to treat various conditions/diseases: – analgesics, antipyretic and anti-inflammatory • Focus on anti-inflammatory agents • Prototype: acetylsalicyclic acid (Aspirin) – Alternative: steroids as useful anti-inflammatory drugs: - inhaled corticosteroid for long-term treatment of persistent asthma - glucocorticoids, metabolic side effects - DMARDs (disease-modifying anti-rheumatic drugs) Nonsteroidal anti-inflammatory drugs (NSAIDs): a definition? • Heterogenous groups of therapeutic drugs to relieve pain, fever and inflammation • Approx 50 NSAIDs: - Similar pharmacological properties - use often limited to approved indications by the regulatory agencies • Considerable confusion in terminology, classification as NSAIDs is somewhat misleading: – Also antipyretic: Antipyretics cause the hypothalamus to override an interleukin-induced increase in temperature to reduce fever. – Also analgetic: Analgesic drugs act on the peripheral and central nervous systems to relieve pain • Should paracetamol be included in this group? Antipyretic and analgetic, but essentially devoid of anti-inflammatory actions Inflammation in Health and Disease • In health, inflammation is a normal and essential response: – Wound healing – Infection – Thrombosis • In disease states, inflammation is excessive: – Asthma – Atherosclerosis – Cancer – Rheumatoid arthritis Inflammation in Disease: Rheumatoid arthritis Classical model for NSAIDs Pathogenesis of Rheumatoid arthritis: 1. Unknown activation of cells in synovial joint 2. Causes production of immunoglobulins (IgG), forming immune complexes 3. Activates the complement system 4. Activates production of chemokines 5. Attracts Leucocytes which ingest the IgG complexes to become rheumatic arthritis cells. 6. These cells secrete hydrolases into the extracellular space 7. Hydrolases degrade extracellular tissue, e.g. collagen, which provokes an inflammatory response in rheumatoid joints (all of this induces cyclooxygenase expression) 8. Swelling of joints, low-grade fever, pain 9. Treatment strategy: inhibit production of inflammatory mediators (step 4, 7: e.g. histamine, serotonin, eicosanoids, prostanoids) NSAIDs: Mechanism of Action Cell membrane phospholipids NSAIDs X Prostanoids Prostanoids • Regulate/increase inflammatory response • Naturally occurring 20-carbon cyclopentano-fatty acid derivatives • Produced in mammalian tissue from polyunsaturated fatty acids in cell membrane phospholipids • The term "prostanoids" relates strictly to the products of the cyclooxygenase pathway: – Prostaglandin – Thromboxanes – Prostacyclin (also known as PGI2) • Found in essentially every compartment of the body • Many prostanoids exist, with diverse pharmacological properties General Structure Classified by the capital letters A, B, C, D, E, F, G, H, I, J, K depending on the nature and stereochemistry of oxygen substituents at the 9- and 11positions http://www.cyberlipid.org/prost1/pros0001.htm Subscripts • The number of double bonds in the side chain connected to the cyclopentane ring is designated by subscripts 1, 2 or 3 • Reflects the nature of the biosynthetic precursors: – Subscript 1, derived from 8,11,14-eicosatrienoic acid – Subscript 2, derived from arachidonic acid (5,8,11,14-eicosatetraenoic acid) plus additional cis bond at C-5, C-6 positions – Subscript 3, derived from 5,8,11,14,17-eicosapentaenoic acid plus additional cis bond at C-17, C-18 • Most common fatty acid in humans is arachidonic acid (AA), hence PGs of the 2 series play an important biological role PGs of the 2 Series are Derived from AA Arachidonic acid is derived from linoleic acid, diet, phospholipids (phosphatidylethanolamine, phosphatidylcholine) in cell membranes Phospholipase A2 Foye’s Principals of Medicinal Chemistry, 2002 Foye’s Principals of Medicinal Chemistry, 2002 Foye’s Principals of Medicinal Chemistry, 2002 The complexity of prostanoids: distinct prostaglandin receptors (GPCR’s) in different tissues Grosser T. Thromb Haemost. 2006 Oct;96(4):393-400. http://www.hosppract.com/issues/2001/03/ceper.htm COX-1/COX-2: Similarities • COX-1 and COX-2 are isoenzymes • COX-1 gene is located on chromosome 9, COX-2 gene is on chromosome 1 • Molecular weight is similar: COX-1 67 kDa (599 aa), COX-2 72 kDa (604 aa) • Both consist of a long narrow channel open at one end and with a hairpin bend at the other • In amino acid sequence, the isoforms are 65% identical • They are almost completely identical at their catalytic site to carry out similar enzymatic functions • AA is pulled into the COX's open end and fully formed prostaglandins leave the cell via facilitated diffusion European Journal of Medicinal Chemistry (2001), 36 (2) , 109-126 COX-1/COX-2: Differences • The differences between COX-1 and COX-2 are genetically determined and cause several amino acid changes • Position 523: valine in COX-2, bulky isoleucine in COX-1, causes a structural difference in the active site of the enzyme • Valine 523 in COX-2 creates an additional side pocket, which is a pre-requisite for COX-2 drug selectivity. Access to this side pocket is restricted in COX-1 • Valine 434 in COX-2 and Isoleucine 434 in COX-1, wider entry into the additional side pocket of COX-2, helps to establish COX-2 drug selectivity European Journal of Medicinal Chemistry (2001), 36 (2) , 109-126 NSAIDs: COX-1/COX-2 selectivity • Both COX-1 and COX-2 have arginine at position 120 of their amino-acid sequence • Non-selective NSAIDs bind Arginine 120 to block arachidonic acid uptake • Structural differences at Pos 523 (Val/Isoleucine) pharmacological targeting of either COX-1 or COX-2 permit selective • Valine, a smaller amino acid in COX-2 creates a side pocket that allows binding of COX-2-selective inhibitors (too bulky for COX-1) http://www.hosppract.com/issues/2001/03/ceper.htm NSAIDs: COX-1/COX-2 selectivity http://www.hosppract.com/issues/2001/03/ceper.htm COX-1 (“Good”) vs. COX-2 (“Bad”): An oversimplification… COX-1 (“Good”) vs. COX-2 (“Bad”): • The thinking behind development of COX-2 selective NSAIDs… – COX-1 is constitutive, maintaining normal cell function within the mucosa of many organs – COX-2 is an inducible enzyme, it becomes abundant in activated macrophages and other cells at sites of inflammation – Underlying paradigm - selective COX-2 inhibitors would primarily target inflammation, with minimal disturbance of homeostatic COX-1 function Summary • Nonsteroidal anti-inflammatory drugs (NSAIDs) are antiinflammatory, analgesic and antipyretic • Inflammation plays a role in health and disease • Prostanoids, especially those derived from arachidonic acid, induce inflammation • NSAIDs act on COX enzymes to inhibit prostanoid synthesis • COX-1 and COX-2 are isozymes • Differences in COX enzyme structure can be exploited to make selective COX-2 inhibitors NSAIDs Lecture 2 Selective vs. Non-selective COX Inhibitors Learning objectives: • Review the drug discovery timeline for NSAIDs • role and structure of COX isozymes • structural basis of COX inhibition for commonly used NSAID drug classes: – Salicylates (e.g. aspirin) – Arylalkanoic acids » Aryl- and Heteropropionic acids (e.g. ibuprofen) » Aryl- and Heteroarylacetic acids (e.g. indomethacin, sulindac, diclofenac and nabumetone) – Selective COX-2 inhibitors (e.g. celecoxib and rofecoxib) • What went wrong? Timeline of Drug Discovery: NSAIDs • 1763 Edward Stone described efficacy of salicylate-containing plant extracts for the treatment of malarian fever and rheumatic complaints. • 1860 - salicylic acid was chemically synthesized by Kolbe • 1898 - acetylsalicylic acid used medicinally (aspirin - a from acetyl and spirin, an older name given to salicyclic acid (spiric acid)) • 1899 - acetylsalicylic acid was registered and introduced commercially as "aspirin" by Bayer (Germany). • 1940s – phenylbutazone (Arylalkanoic Acid; largest group of NSAIDs; 1950 - arthritis therapy) • 1950s - fenamates • 1960s – indomethacin by Shen (Merck, most potent Arylalkanoic Acid) • 1970s and 1980s - number of chemical abstracts dealing with potential inhibitors of the COX enzyme rose markedly ~ 2,500 per year 1970s – including the proprionates and the oxicams • 1980s – COX-2 discovered • 1990s – selective COX-2 inhibitors (1997 – 2000: celecoxib, rofecoxib, valicoxib) • 2002 – COX-3 discovered • 2004 – selective COX-2 inhibitors withdrawn from market NSAIDs: Common Structural Features • Acidic centre • Aromatic/heteroaromatic ring • Additional centre of lipophilicity (either an alkyl chain or additional aromatic ring) • Corresponds with carboxylic acids and double bonds of arachidonic acid 5,8,11,14-eicosatetraenoic acid Salicylates (e.g. aspirin) •Acidic centre •Aromatic ring Aspirin (Acetylsalicyclic acid) Salicyclic acid •Acetyl group Aspirin: Interaction with COX (I) • • • • Irreversible inhibitor of COX-1 and COX-2 Aspirin acetylates Ser-530 so that AA cannot reach the catalytic center Arg-120 in COX stabilizes the carboxylate group of aspirin The aromatic ring structure accommodated within the largely hydrophobic binding channel (Tyr-385) Aspirin: Interaction with COX (II) hydrophobic hydrophobic acetylates acetylates stabilizes carboxyl stabilizes carboxyl Nature Reviews Drug Discovery 2, 179-191 (2003) Aspirin (and other salicylic acids): Mechanism of action: inhibition of histamine release inhibition of hydrolase release inhibition of leucocyte accumulation inhibition of prostaglandin synthesis Aspirin is the only NSAID that covalently modifies COX-1/2 10-100 more potent to inhibit COX-1 than COX-2 rapid absorption upon oral administration, absorption highly dependent on gastric pH, aspirin binds to albumin (drug-drug interactions) Side effects: peptic ulcers in GI tract (lesion in the mucous membranes of the digestive tract, due to excessive damage to the mucosal cells that line the stomach, can become malignant) Salicylates (aspirin) inhibit prostaglandin synthesis, in particular PGE, which normally inhibits gastric acid secretion---gastric mucosa cell damage plus inhibition of platelet aggregation---bleeding Non-selective NSAIDs: Dual Insult Arylalkanoic Acids – Largest group of NSAIDs – All non-selective – Center of acidity: carboxylic, enolic or hydroxamide function,sulfonamide or tetrazole ring; relates to carboxylic acid of arachidonic acid – Consist of: » Aryl- and Heteroarylacetic acids, e.g. • indomethacin • sulindac • diclofenac • nabumetone » Aryl- and Heteropropionic acids, e.g. • ibuprofen • flurbiprofen Indomethacin: Interaction with COX (I) • Non-selective COX inhibitor, causes slow, time-dependent inhibition of COX-1 and COX-2 • Chlorobenzoyl group is stabilized by hydrophobic interactions • The acidic function of indomethacin associates with Arg-120 of COX-1/2 • One of the most potent NSAIDs • More potent antipyretic and analgetic effects compared to aspirin • Potent inhibitor of prostaglandin synthesis Sulindac • Sulindac is a prodrug, aimed to reduce GI side effects of indomethacin • Converted to a metabolite ~ 8X more effective than aspirin Sulindac active sulphide metabolite 8-fold more potent than aspirin Diclofenac • Unique amongst NSAIDs: 1. Potency (3-1000 x more potent than other NSAIDs – strong decrease in prostaglandins, thromboxanes) 2. Inhibits lipoxygenase –decreased leukotrienes (e.g. LKB4) 3. Inhibits AA release and stimulates AA re-uptake – reduced AA availability 4. Most widely used NSAID Nabumetone: a non-acidic NSAID • Non-acidic - no primary insult; • poor ability to inhibit COX in gastric mucosa - minimum secondary insult • Nabumetone is metabolized to 6MNA (6-methoxy-naphthalene-2acetic acid) • 6MNA is an effective inhibitor of COX in joints • Classic pro-drug approach in drug design Aryl- and Heteropropionic Acids • Class name “profens” • Substitution of a methyl group on the carbon atoms separating the acid centre from the aromatic ring (increased anti-inflammatory activity) • Examples include: » ibuprofen » flurbiprofen • Reversible, competitive inhibitors of COX-1 and COX-2 (S) (+)-isomer is biologically active COX-1 (“Good”) vs. COX-2 (“Bad”): An oversimplification… • The thinking behind development of COX-2 selective NSAIDs… – COX-1 is constitutive, maintaining normal cell function within the mucosa of many organs – COX-2 is an inducible enzyme, it becomes abundant in activated macrophages and other cells at sites of inflammation • Underlying paradigm - selective COX-2 inhibitors would primarily target inflammation, with minimal disturbance of homeostatic COX-1 function • An oversimplification… Selective COX-2 Inhibitors: celecoxib (Celebrex) and rofecoxib (Vioxx) COX-1 (“Good”) vs. COX-2 (“Bad”): An oversimplification… COX2-hypothesis Selective COX2 inhibitors (‘coxibs’) are molecules with side chains which fit into the hydrophobic pocket, but are too large to block COX1 with equal affinity Hypothesis 1) GI-toxicity of NSAIDs is due to inhibition of COX1-mediated production of PGE2 and TXA2 in gastric epithelium and platelets 2) COX2 is induced at inflammatory sites and the major source of pain and inflammation mediating PGs But: COX1 is also induced with inflammation COX2 is constitutively expressed in many non-inflamed tissues COX-1 (“Good”) vs. COX-2 (“Bad”): An oversimplification… Increased COX2 selectivity increases cardiovascular risk: withdrawn worldwide after detection of increased CVD events of risk patients Grosser T, Thromb Haemost, 2006, 96, 393-400 COX2 inhibitors: marked reduction in PGI2, a potent inhibitor of platelet function and vasorelaxing agent - Loss of a local inhibitor of prothrombotic stimuli; patients with pre-existing risk factors for thrombosis are at risk; even partial inhibition of PGI2 increases thrombotic process COX-2 inhibitors depressed the biosynthesis of PGI2 without a concomitant effect on thromboxane or platelet aggregation