QUALITY MANUAL - Kimberley Aboriginal Medical Services Council
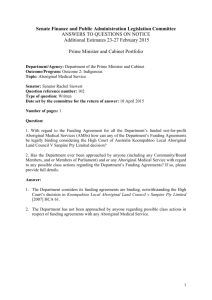
advertisement

KIMBERLEY ABORIGINAL MEDICAL SERVICES COUNCIL (KAMSC) ABN; 31 892339645 QUALITY MANUAL Contents 1. 1.1. Scope and exclusions 4 Scope .......................................................................................................................................................................... 4 1.2. Exclusions from iso 9001 2008 .................................................................................................................................. 4 1.3. Purpose of this document ........................................................................................................................................... 4 2. 2.1. Organisation profile 5 History ........................................................................................................................................................................ 5 2.2. Legal structure ............................................................................................................................................................ 5 2.3. Vision ......................................................................................................................................................................... 5 2.4. Mission ....................................................................................................................................................................... 5 2.5. Key priorities and strategies ....................................................................................................................................... 6 2.6. Clients ......................................................................................................................................................................... 7 2.7. Products and services.................................................................................................................................................. 7 2.8. Geographical reach of products and services.............................................................................................................. 8 2.9. KAMSC organisational chart ..................................................................................................................................... 8 3. 3.1. Definitions, documents and records 8 Definitions .................................................................................................................................................................. 8 4. 4.1. Quality management system 10 Overview of the quality management system ........................................................................................................... 10 4.2. Documentation requirements .................................................................................................................................... 14 4.2.1. General ..................................................................................................................................................................... 14 4.2.2. Quality manual ......................................................................................................................................................... 14 4.2.3. Control of documents ............................................................................................................................................... 14 4.2.4. Control of records ..................................................................................................................................................... 15 5. 5.1. Management responsibility 16 Management commitment ........................................................................................................................................ 16 5.2. Client focus ............................................................................................................................................................... 16 5.3. Quality policy ........................................................................................................................................................... 17 5.4. Planning .................................................................................................................................................................... 17 5.4.1. Quality objectives ..................................................................................................................................................... 17 5.4.2. Quality management system planning ...................................................................................................................... 18 5.5. Responsibility, authority and communication .......................................................................................................... 18 5.5.1. Responsibility and authority ..................................................................................................................................... 18 5.5.2. Management representative ...................................................................................................................................... 19 5.5.3. Internal communication ............................................................................................................................................ 19 5.6. Management review ................................................................................................................................................. 20 5.6.1. Review input ............................................................................................................................................................. 20 5.6.2. Review output ........................................................................................................................................................... 20 6. 6.1. Resource management 21 Provision of resources .............................................................................................................................................. 21 Document1_rev date 01/08/2013 Page 2 of 26 6.2. Human resources ...................................................................................................................................................... 21 6.2.1. General ..................................................................................................................................................................... 21 6.2.2. Competence, training and awareness ........................................................................................................................ 21 6.3. Infrastructure ............................................................................................................................................................ 21 6.4. Work environment .................................................................................................................................................... 21 7. 7.1. Service delivery (product realisation) 22 Planning of product realisation ................................................................................................................................. 22 7.2. Client related processes ............................................................................................................................................ 22 7.2.1. Determination of requirements related to the product .............................................................................................. 22 7.2.2. Review of requirements related to the product ......................................................................................................... 22 7.2.3. Client communication............................................................................................................................................... 22 7.3. Design and development (exemption claimed)......................................................................................................... 22 7.4. Purchasing ................................................................................................................................................................ 22 7.4.1. Purchasing processes ................................................................................................................................................ 22 7.4.2. Purchasing information............................................................................................................................................. 23 7.4.3. Verification of purchased product ............................................................................................................................ 23 7.5. Production and service provision .............................................................................................................................. 23 7.5.1. Control of production and service provision ............................................................................................................ 23 7.5.2. Validation of processes for production and service provision .................................................................................. 23 7.5.3. Client property .......................................................................................................................................................... 23 7.5.4. Preservation of product ............................................................................................................................................. 23 8. 8.1. Measurement, analysis and improvement 24 General ..................................................................................................................................................................... 24 8.2. Monitoring and measurement ................................................................................................................................... 24 8.2.1. Client satisfaction ..................................................................................................................................................... 24 8.2.2. Internal audit ............................................................................................................................................................. 24 8.2.3. Monitoring and measurement of processes .............................................................................................................. 25 8.2.4. Monitoring and measurement of product .................................................................................................................. 25 8.3. Control of nonconforming product ........................................................................................................................... 25 8.4. Analysis of data ........................................................................................................................................................ 25 8.5. Improvement............................................................................................................................................................. 25 8.5.1. Continual improvement ............................................................................................................................................ 25 8.5.2. Corrective action....................................................................................................................................................... 26 8.5.3. Preventive action ...................................................................................................................................................... 26 Document1_rev date 01/08/2013 Page 3 of 26 1. SCOPE AND EXCLUSIONS 1.1. Scope The KAMSC Quality Management System relates to the management and provision of services and products. 1.2. Exclusions from ISO 9001 2008 Clause 7.3 (incorporating subclauses 7.3.1 to 7.3.7) relating to Design & Development Clause 7.5.3 Identification and traceability as unique identification of product and traceability is not required. These clauses are not applicable to KAMSC, it does not develop products or employ monitoring or measuring equipment to plan, deliver or evaluate its products or services. 1.3. Purpose of this document This Quality Manual describes the Quality Management System operated by KAMSC and the relevant roles and responsibilities of office bearers for overseeing and implementing its components. Document1_rev date 01/08/2013 Page 4 of 26 2. ORGANISATION PROFILE 2.1. History The Kimberley Aboriginal Medical Services Council (KAMSC) was established in 1986. The council was initially formed as a cooperative between the Broome Regional Aboriginal Medical Service (BRAMS) and the East Kimberley Aboriginal Medical Service (EKAMS) now the Ord Valley Aboriginal Health Service (OVAHS) with membership from the then developing, Halls Creek health service committee and Fitzroy Crossing community representatives. These communities saw the benefit of sharing pooled resources and collective effort in the region. Member services now include; 2.2. Broome Regional Aboriginal Medical Service (BRAMS) Ord Valley Aboriginal Health Service (OVAHS) Derby Aboriginal Health Service (DAHS) Yura Yungi Medical Service (YYMS) Kutjungka Clinical Services (KAMSC Remote Clinic) Beagle Bay Health Services (KAMSC Remote Clinic) Bidyadanga Community Clinic (KAMSC Remote Clinic) Legal Structure KAMSC is incorporated under the Western Australian (WA) Associations Incorporation Act 1987 and it adheres to the National Aboriginal Controlled Health Organisations (NACCHO) definition of Aboriginal health which means ‘not just the physical well-being of an individual but refers to the social emotional and cultural well-being of the whole community in which each individual is able to achieve their full potential as a human being, hereby about the total well-being of their community. It is a whole of life view and includes the cyclical concept of life-death-life’. 2.3. Vision The vision for KAMSC includes many aspects of the improvement and management of Aboriginal health across the Kimberley region. By definition, the vision does not match the current context of Aboriginal health. Outstanding improvements are required in the provision of culturally safe and appropriate public health care. 2.4. Mission KAMSC exists as a responsible Aboriginal Community Controlled Council to improve Aboriginal health in the Kimberley region of Western Australia by providing continually improving, essential, cooperative services along with a unified voice and representation for existing and developing comprehensive primary health care services and community health services. In achieving its mission KAMSC will; Document1_rev date 01/08/2013 Page 5 of 26 2.5. Provide Aboriginal Community Controlled Health Services (ACCHS) essential services which are not otherwise available to them. Contribute to policy development and representation at a community (community clinic), district (ACCHS), regional (KAMSC), state (AHCWA) and national (NACCHO) level. Regularly monitor, evaluate and report on its achievements in improving Aboriginal health. Provide a single and accepted voice that represents all of its Kimberley Aboriginal constituents. Be accountable in all of its dealings with its co-operative of Board members and other stakeholders. Key priorities and strategies Ongoing and improved Aboriginal community control of health services for Aboriginal people in the Kimberley. KAMSC has a high level of acceptance and status amongst its member organisations, throughout the region and beyond. Larger Aboriginal community controlled health services, continue to be involved with public hospitals with ongoing work outside the hospital system. ACCHS have a strong focus on preventive approaches rather than largely curative medical models. Comprehensive holistic primary health care services are available, including dental, aged care, social support suicide prevention and management services. Specialist services including dialysis training are available through the central health service. Drug problems have been addressed by Aboriginal and Torres Strait Islander peoples. Self management by Aboriginal people of health and other primary services is recognised and accepted as legitimate at regional, state and national levels. Aboriginal people own and control their health policy, resources, and research and public health services. Aboriginal people are supported to take primary responsibility for their own health by health services in the region. Aboriginal communities are proud, happy and healthy and strongly involved in managing their own health and determining their own health needs. Aboriginal culture plays a strong role in managing the health of Aboriginal people. Aboriginal people throughout the Kimberley are healthy and there are no inequities in with an equal standard of health across all Kimberley people. Chronic diseases such as diabetes, renal failure, rheumatic fever and chronic lung disease have been dramatically reduced or eliminated. There is no longer death associated with hepatitis b and HIV. Access is improved, particularly during the wet season. Environmental determinants of health status (e.g. housing, sanitation, food security) are recognised and improved Aboriginal young people are supported through a scholarship scheme to become involved in education in health related fields. Encouragement and assistance is provided to Aboriginal people from the Kimberley region to become clinicians Document1_rev date 01/08/2013 Page 6 of 26 2.6. Clients KAMSC has identified 4 client groups as follows; 2.7. Funding bodies Member services - Aboriginal Community Controlled Health Services (ACCHS). Patients attending the KAMSC clinics KAMSC staff Products and services KAMSC (Kimberley Aboriginal Medical Services Council) is a regional Aboriginal Community Controlled Health Service (ACCHS), providing a collective voice and regional level support services for a network of member ACCHS from towns and remote communities across the Kimberley region of Western Australia. The Broome Regional Aboriginal Medical Service (BRAMS) was the first Aboriginal Community Controlled Health Service (ACCHS) established in the Kimberley in 1978, and was followed by the East Kimberley Aboriginal Medical Service (EKAMS, in Kununurra) in 1984. The vision for a unified voice, to provide centralised resources and collective advocacy for the sector, achieved reality in 1986 with the establishment of KAMSC. Today, the KAMSC collective represents four independently incorporated ACCHS – the Ord Valley Aboriginal Health Service (OVAHS, previously EKAMS), the Derby Aboriginal Health Service (DAHS), Yura Yungi Medical Service (YYMS in Halls Creek), Broome Regional Aboriginal Medical Services. KAMSC Governing Council is made up of one representative from each of its independent member services and one representative from the community councils of Beagle Bay and Bidyadanga, where independent ACCHS are not yet established. KAMSC general meetings are held quarterly in different locations across the region. KAMSC provides a wide range of regional services to support member ACCHS, with business units including: Population Health Social and Emotional Well Being Business Support Health Promotion Information Communications Technology Pharmacy support and training Corporate Services including payroll support, HR, stores, accounting and administrative services Accredited health training and education Research Regional renal services including dialysis Remote Area Clinics Together KAMSC and its member ACCHS’s are a major employers in the Kimberley, with Aboriginal people representing more than 70% of its 300+ strong workforce. KAMSC is a member of the Aboriginal Health Council of WA (AHCWA) and of the National Aboriginal Community Controlled Health Organisation (NACCHO) 2.8. Geographical reach of products and services KAMSC (Kimberley Aboriginal Medical Services Council) is a regional Aboriginal Community Controlled Health Service (ACCHS), providing a collective voice and regional level support services for a network of member ACCHS from towns and remote communities across the Kimberley region of Western Australia. 2.9. KAMSC organisational chart Whilst KAMSC delivers a comprehensive range of services and programs, it operates within a simple line management structure with all managers having direct accountability and reporting responsibilities to the CEO. The CEO reports directly to the board of directors. Over-riding responsibility and accountability for the KAMSC Quality Management System (QMS) rests with the board of directors. Within the KAMSC organisational structure, responsibility has been delegated by the board of directors. Within the KAMSC organisational structure, responsibility has been delegated by the board of management to the CEO as its representative to progress our quality policy and quality objectives. As the quality manager, the CEO has delegated authority and responsibility to the Quality Coordinator and management team for maintenance of the QMS. KAMSC Board Chairperson Medical Director HR Executive Assistant Corporate Services Population Health CEO Remote Area Services - Resourcing - Administration - Remuneration - OH&S - Industrial Relations - Information Services - Population Health - Asset Management - Health Promotions - Policy Development - Professional Dev - Admini - Reception - Executive Office - Research -Remote Area Services - Beagle Bay - Bidyadanga - Kutjungka - Clinical G’vnce - Clinical Support 3. DEFINITIONS, DOCUMENTS AND RECORDS 3.1. Definitions Renal Services CAPTER - KSDC - Derby Dialysis - Cultural Training - Fitzroy Dialysis - AHW Training - Kununurra Dialysis - Rural Clinical School - KRSS; kidney disease prevention - GP Registrar Training - UWA/KAMSC Research - Home Therapies SEWB - Headspace - Workforce Support Unit - Kimb/Pilbara Projects Financial Services - AMS Accounts - Accounts - Payroll - Risk Management - Travel - Business Dev - Agreement Audits The following terms and definitions are generally defined within ISO 9001:2008 Quality management systems – Requirements and have been adapted to our organisation. Audit refers to a systematic, independent and documented activity aimed at verifying that the organisation’s policies and procedures are being fulfilled. Client refers to a client, Client, patient or person or organisation that is provided with a product or service. (client) Contract refers to agreed requirements between us and our partners and funding bodies. These may be also be MOU’s and Service Level Agreements. Continual improvement refers to both corrective action and preventive action that is taken to correct or address a (corrective and preventive action) problem and make change in the organisation that improves service delivery or our operations. Corrective action generally involves making changes to policies or procedures to respond to an idea or incident. Preventive action generally involves taking action before a negative event (or non-conformance) occurs to reduce the chances of a negative event occurring. Non-conformance refers to a deficiency in characteristic, measured quality, documentation, or procedure that renders a service, program or product unacceptable to specified requirements. Procedure refers to a document that specifies the purpose, scope, responsibilities, actions and methods for a quality related activity. Process refers to a task or activity that involves staff or other resources to provide a service or conduct our operations. Quality refers to circumstances where all characteristics conform to requirements. Quality Management refers to a set of coordinated activities aimed at controlling an organisation with regards to quality. Quality Project Plan refers to a document that specifies the resources, activities, and methods necessary to control a specific project, service, product or contract. Quality Review Group Refers to the internal staff committee chaired by the CEO to conduct management review Quality system refers to a planned and documented set of policies, procedures, resources, methods, and actions aimed at fulfilling our quality and service delivery objectives Services (Product) refers to the products and services delivered to meet our aims. Service delivery (product realisation) refers to product realisation or the fulfilment or achievement of a plan or objective to deliver a service or product. Supplier refers to an individual or organisation that provides any services, materials or products that form part of the product supplied to the Client. This may include those otherwise referred to as subcontractors. Validation refers to evidence or proof that the product meets requirements, and is fit for its intended purpose. Verification refers to confirmation that a product or action conforms to specified requirements. Document1_rev date 01/08/2013 Page 9 of 26 4. QUALITY MANAGEMENT SYSTEM 4.1. Overview of the quality management system The purpose of our Quality Management System is to support our operations so that our services and products consistently and effectively meet Client expectations, applicable regulatory requirements and to provide a mechanism for continual improvement. The Quality Management System provides a framework from which our staff, subcontractors and partners can make appropriate decisions whilst ensuring that applicable minimum standards are met. The Quality Management System applies to all activities of the organisation, and has been developed in accordance with ISO 9001:2008. The Quality Management System is fully documented and structured in three levels. The diagram below is a representation of this structure. Level 1 Quality Manual & Quality Policy Level 2 Processess and Systems Level 3 Procedures, Forms, Templates etc Level 4 Records Quality System Elements Level 1: Quality Manual and Quality Policy – The Quality Manual describes the scope of the quality management system, the processes and documented procedures established to operate the quality management system and the interactions between these processes. The Quality Policy describes <org name>’s commitment to implementing, maintaining and continually improving the quality management system. Level 2: Processes and Systems – The systems deployed across the organisation to support the management of critical processes. Level 3: Procedures, Forms, Templates - These documents describe the actual process, and controls applied, to all activities concerned with the attainment of a quality assured services and programs. Level 4: Records - These documents demonstrate evidence of activity. Document1_rev date 01/08/2013 Page 10 of 26 Quality Management System Process Map The Quality Management System Process Map below provides a high level description of our quality management system. Document11_rev date 01/08/2013 Page 11 of 26 Document11_rev date 01/08/2013 Page 12 of 26 Quality Management System Functional Specification The diagram below describes a set of specific electronic management systems (registers) used for initiating, actioning, monitoring and evaluating key business processes within the organisation. It should how our systems map to the ISO 9001:2008 standard. Resources we need to do our work Staff and subcontractors Equipment and Facilities Training/Licensing Register Repairs Register OHS Register Suppliers register Clients and Stakeholders Client and stakeholder requirements The work we do and how we do it How well we do our work Contracts and MOU’s Project plans and specifications Legislative requirements Electronic feedback forms Plans Policies and procedures Forms, checklists, templates Evaluations Audits Reports Contract Register Compliance Register Feedback Register Document Register Audit Register Quality Records Register Improvement Clients and Stakeholders Learnings How we improve Client and stakeholder satisfaction Ideas for improvement based on reviews, evaluations, audits, feedback and staff ideas Surveys Feedback Continual Improvement Register Feedback Register Quality Management System Functional Specification Document11_rev date 01/08/2013 Page 13 of 26 4.2. Documentation requirements 4.2.1. General Our quality management system documentation comprises: A quality manual including quality objectives A quality policy Documented procedures and policies Documents relating to client requirements and statutory requirements Documents relating to planning of operations and product realisation (service delivery) Records required by recognised standards and by the organisation Documented procedures relating to 4.2.1c of the ISO 9001 Standard 4.2.2. Quality manual A Quality Manual (this document) has been created that describes our quality management system and other operational management processes. The Quality Manual also includes a quality policy, quality objectives, and references to the required procedures in 4.2.1c of the ISO 9001 Standard. 4.2.3. Control of documents Documents as referred to in 4.2.3 of the ISO 9001:2008 Standard are stored electronically in the Document Register. The Document Register holds key data about a document such as version, date last reviewed, location, and the deadline for the next review of the document. The Document Register provides an index of all controlled documents held by our organisation and provides hyperlinks to those documents. QMS Document Register (example data only) All documents on the Document Register carry a unique reference number and each document is authorized by a designated approving officer. Formal documents produced by the company are reviewed, modified and authorized, as part of this document control procedure. The Document Register displays and provides access to key documents, such as policies, procedures, templates and forms that have been approved for use in the organisation. The Document Register is used to: Upload, approve and view quality system documents eg. policies, procedures, forms and templates Set and manage the timely review of quality system documents Print reports on the documents stored on the system Document1_rev date 01/08/2013 Page 14 of 26 4.2.4. Control of records Records as referred to in 4.2.4 of the ISO 9001:2008 Standard are stored electronically in the Quality Records Register and in physical files located in the organisation. The Records Register primarily holds audit reports, program evaluations and minutes of the senior Management Team and Clinical Review Committee. The Records Register provides an index of these records held by our organisation and provides hyperlinks to those records. QMS Records Register (example data only) All records on the Record Register carry a unique reference number and each record must be authorized by a designated approving officer to appear of the Register. An audit trail of such approvals is kept by the system. The Control of Records Procedure provides details of the location, retrieval, retention and disposition of records held by KAMSC including those required by the ISO 9001:2008 Standard. Document1_rev date 01/08/2013 Page 15 of 26 5. MANAGEMENT RESPONSIBILITY 5.1. Management commitment The process of managing the business is performed by the Directors who define the overall strategy of the business and the CEO who is responsible for the day-to-day management of the organisation. The CEO carries out this function in collaboration with subcontractors and staff as available. The Directors and CEO have leadership responsibility for the Quality Management System and associated processes. This includes ensuring availability of resources, establishment and review of the Quality Policy and Quality Objectives, and implementation and continual improvement of the Quality Management System. The Directors and CEO also have the responsibility to communicate the importance of meeting Client, client, statutory and regulatory requirements. The KAMSC Quality Policy is posted in a prominent location and in public view at the KAMSC Office and is available on the KAMSC website at www.kamsc.org.au/ In 2012 KAMSC Directors implemented the quality management system so described in this manual. 5.2. Client focus Statutory and regulatory requirements of Clients and stakeholders are documented in the Contracts Register. QMS Contracts Register (example data only) The compliance requirements related to the contractual and statutory obligations are scheduled in the Compliance Register in our quality management system. Document1_rev date 01/08/2013 Page 16 of 26 QMS Compliance Register (example data only) QMS Compliance Register (example data only) 5.3. Quality policy The following Quality Policy describes our commitment to quality and continual improvement and how the policy relates to our Clients’ requirements; Doc099_KAMSC Quality policy_v1_rev date 01/08/2013 5.4. Planning 5.4.1. Quality objectives The Quality Objectives of KAMSC support our Quality Policy, goals and aims. The following table outlines our Quality Objectives and how the organisation’s performance against these objectives will be measured. Quality Objective Performance Measure Target result 1. Governance; maintain an effective Quality Management System compliant with ISO 9001:2008 and driving improvement across the company QMS implemented Quality Coordinator go-live in the organisation by June 2012 QMS compliance with ISO 9001:2008 Certification achieved by May 2013 Audit program implemented Audit program implemented by February 2013. >90% of scheduled audits completed in timeframe Improvement actions implemented >90% of approved corrective or preventive actions completed within required timeframe Document1_rev date 01/08/2013 Page 17 of 26 Quality Objective 2. Deliver high quality services that meet or exceed our clients’ expectations. Performance Measure Target result Management review Senior Management Team and Clinical Review Committee meeting minutes show regular meetings and compliance against QRG procedures Credentialing, registration, education and training of staff. All staff will be appropriately credentialed /registered / licensed to undertake the role for which they have been employed. Minutes of CRC show evidence of credentialing processes. >90% of staff undertaken mandatory training e.g. emergency management, CPR, manual handling as appropriate. 3. Effective resource management Provision of adequate resources (human, ITC, infrastructure) Departmental internal audit program implemented by February 2013. Availability and utilisation of current best practice standards/local guidelines. Minutes of SMT and CRC evidence that all clinical and organisational policies/procedures/guidelines/standards etc, are reviewed and updated as appropriate (at least every 3 years). Patient outcomes, e.g. as measured in the OCHRE streams report. Data supplied to funding bodies. >90% of funding body reporting requirements completed within the required timeframe. Customer feedback (complaints/compliments/suggestions etc) >90% of approved continual improvement suggestions actioned within required timeframe. Staff satisfaction survey undertaken every 3 years. Compliance with financial /contract management statutory requirements and reporting. >90% of financial/contract reporting requirements are completed within the required timeframe. Review of financial management processes through internal audit committee. Internal financial audit committee to be established by Dec 2012, minutes show regular meetings and compliance against ORG standards. Quality Objectives 5.4.2. Quality management system planning Planning and review of all aspects of the KAMSC quality management system is undertaken by the KAMSC Quality Coordinator, the KAMSC management representative (CEO) and agreed at the SMT on an annual basis. 5.5. Responsibility, authority and communication 5.5.1. Responsibility and authority All staff have a shared responsibility to contribute to the effective management of quality safety and risk and all staff share the authority and responsibility to identify non-compliances and possible improvements, and record these instances in order for corrective or preventive action can be taken. All staff are given the authority to perform their allocated responsibilities and these authorities are detailed in the relevant duty statements. Document1_rev date 01/08/2013 Page 18 of 26 Specific responsibilities have been identified to key roles to help ensure compliance with statutory and quality related requirements. Responsibility Directors Management Staff Quality Management Representative Compliance with contractual and regulatory obligations CEO Approval of Quality Management System Monitoring effectiveness of Quality Management System Service delivery planning and implementation Supplier selection and purchasing Internal Audit Document control Continual improvement Contract management and control Processing of invoices Purchasing Planning Control of Finance and Accounts New service and product identification IT planning and management Staff responsibilities 5.5.2. Management representative The KAMSC CEO is the management representative for the company. The management representative will: 5.5.3. ensure that processes needed for the quality management system are established, implemented and maintained report to top management on the performance of the quality management system and any need for improvement ensure the promotion of awareness of Client requirements throughout the organization Internal communication The SMT and CRC meetings are minuted, scheduled in the Meetings Register (below), and are supported by standard agendas. The minutes of the SMT and CRC are held in the Quality Records Register in the Quality Coordinator QMS and the Director’s meeting minutes are held on the CEO’s office. KAMSC also holds a range of team meetings with minutes of these meetings held in the administration office. These meetings are scheduled on the Meetings Register. 2020 Meetings Register Document1_rev date 01/08/2013 Page 19 of 26 5.6. Management review Management review of the suitability and effectiveness of the quality management system takes place annually through the SMT meetings. During the review meetings, actions are allocated and minuted to record the development of the organisation's quality management system. The objectives of Management Review are: To establish that the quality (management) system is achieving the expected results and meeting the company’s requirements, continuing to conform to the Standard, continuing to satisfy Client needs and expectations, and functioning in accordance with established operating procedures. To identify weaknesses and evaluate possible improvements to the system. To review the effectiveness of previous corrective actions, and to review the adequacy and suitability of the management system for current and future operations of the organisation. To review any complaints received, identify the cause and recommend corrective action if required. To review the findings of internal/ external audits and identify any areas of recurring problems or potential improvements. To review the reports of nonconforming items and trend information to identify possible improvements. A terms of reference exists to control and communicate the purpose of the meeting. 5.6.1. Review input A standard template guides the meeting purpose. The input into the SMT includes: 5.6.2. Follow-up actions from previous management reviews Results of audits Analysis of data relating to Client feedback Analysis of data relating to process performance and extent to which <org name> services meets Client requirements Status of preventive and corrective actions (continual improvement) Recommendations for improvement Status report on the Audit Register Status report on the Document Register Status report on staff training and professional development Status report on occupational health and safety Status report on compliance management Review output A standard template ensures consistent and comprehensive documentation of the outputs of the meeting. The outputs of the SMT shall include: Recommendations and actions related to improvement of services related to Client requirements Recommendations to improve the quality management system in relation to document control, internal audit, continual improvement and compliance management Document1_rev date 01/08/2013 Page 20 of 26 6. RESOURCE MANAGEMENT 6.1. Provision of resources The Directors of KAMSC enter into funding contracts to ensure adequate financial resources are available to legally operate the business, implement the quality management system and meet Client requirements. The CEO is responsible for managing processes to obtain self-generated income from other sources. 6.2. Human resources 6.2.1. General KAMSC follows its staff recruitment procedure when appointments are made. These procedures support comprehensive, consistent and transparent assessments of adequacy. 6.2.2. Competence, training and awareness Staff positions define the competencies required for staff to perform their work. The CEO consults with staff to determine training needs and in some cases KAMSC supports staff to access and attend formal and informal training. Training is documented in the Training Register. Required licences and registrations are documented in the Licensing Register. 6.3. Infrastructure Infrastructure planning is discussed on a needs basis and is formally reviewed on an ongoing basis at Director and staff meetings. Vehicle leases are signed off by Directors. KAMSC uses the Repairs Register in the QMS to record infrastructure maintenance requirements. Infrastructure planning is also undertaken prior to executing contracts that may have impacts on facilities and staffing. 6.4. Work environment Facilities, including workstations and associated equipment, shall be maintained in an appropriate state of order, cleanliness, and repair for their use. All work areas must comply with established safety, regulatory and environmental standards and codes. Staff have responsibility for providing cleaning services at the KAMSC offices. Regular environmental safety audits and compliance checks (see Audit and Compliance Register) are conducted, documented on the QMS and reviewed at SMT meetings. Regular fire and safety staff briefings are scheduled in the QMS. Document1_rev date 01/08/2013 Page 21 of 26 7. SERVICE DELIVERY (PRODUCT REALISATION) 7.1. Planning of product realisation The methods and materials used for planning for product realisation differ depending on the service under consideration. All service planning is discussed at both the SMT and CRC and the KAMSC Board meeting as appropriate. 7.2. Client related processes 7.2.1. Determination of requirements related to the product Requirements specified by our Clients can be in any of the following forms; 7.2.2. Formal contracts Memorandum of Understanding Service Level Agreements Funding body specified requirements Review of requirements related to the product Client requirements are reviewed every three years or sooner as required as part of the strategic planning process. 7.2.3. Client communication KAMSC maintains a website at www.kamsc.org.au, produces a ‘quality’ newsletter and produces brochures promoting its products and services. Client feedback is recorded on the Client Feedback Register and complaints are managed in accordance with operational procedures. 7.3. Design and development (exemption claimed) 7.4. Purchasing 7.4.1. Purchasing processes Purchases for equipment are generally made against a written quote from the supplier which specifies the details of the product. Purchase orders for services e.g. electrical maintenance at housing owned by KAMSC are supported by a print out of the job specification held in the QMS Repairs Register. All requests for maintenance are recorded in the QMS repairs register. Suppliers are evaluated and once approved will appear on the Suppliers Register. The criteria for evaluation is determined by top management and specified in the Suppliers Register. Regular review of suppliers occurs and is documented in the Suppliers Register. Issues arising from supplier reviews are recorded in the Continual Improvement Register. The supplier management process is structured to: identify and select suppliers with the capability to meet operational needs establish criteria for selection, evaluation, qualification, and certification of suppliers ensure continuity of supply ensure that critical materials and services are purchased only from qualified sources monitor and provide feedback on supplier performance. Document1_rev date 01/08/2013 Page 22 of 26 The supply process incorporates supplier assessment, order placement, receipt and where required inspection of goods, control of non-conforming goods and the authorisation of payment to suppliers and contractors. 7.4.2. Purchasing information Purchasing of subcontractor services is controlled through purchase orders. The purchase process is documented and structured to meet the following requirements: 7.4.3. ensure that purchasing documents clearly describe the product ordered ensure that purchased products conform to purchase requirements communicate to suppliers the appropriate product, quality, and delivery requirements ensure that purchased materials and services used meet government, safety, and environmental regulations ensure that the finished product and packing materials meet the provisions of regulatory and Client requirements Verification of purchased product Goods received are managed in accordance with procedures which ensure the goods are cross-checked against purchase order. Payment for goods and services is made only after cross-checking statement/invoice against proof of delivery. Non-conforming goods are managed in accordance with the Control of Non-Conforming Product procedure. 7.5. Production and service provision 7.5.1. Control of production and service provision The control of service provision is managed though the operational procedures and operational plans located on the QMS Document Register. Validation of processes for production and service provision Validation of services delivered by KAMSC is determined by ongoing funding and support received from government stakeholders, commitment of community volunteers to act as the Board of Directors, and through feedback received from clients. Disputes are managed in accordance with our complaints policy or through the provisions in contractual agreements. KAMSC retains appropriate public liability and workers compensation insurances to assure against damages claimed as a result of service delivery. 7.5.2. Identification and traceability (exemption claimed) 7.5.3. Client property Client property left unintentionally at KAMSC premises is managed in accordance with the KAMSC lost property procedure. 7.5.4. Preservation of product Equipment relating to the delivery of our services is maintained through maintenance schedules on the Compliance Register or through repair requests through the Repairs Register. Document1_rev date 01/08/2013 Page 23 of 26 8. MEASUREMENT, ANALYSIS AND IMPROVEMENT 8.1. General KAMSC measurement and analysis and improvement processes includes: internal and external audits, client surveys, assessment of statistical data and records, and review of client, staff and stakeholder feedback. Related improvements (corrective and preventive actions) actions are recorded and monitored in our Continual Improvement Register. 8.2. Monitoring and measurement 8.2.1. Client satisfaction KAMSC maintains a register of feedback about client and stakeholder satisfaction. Processes in place to gathering this information include: feedback reported at staff meetings, client suggestion boxes located throughout the organisation and community events. Satisfaction of funding bodies is assessed through the ongoing offers of financial support. 8.2.2. Internal audit Internal audits of the Quality Management System are regularly undertaken to confirm that the operation concerned conforms to organisational procedures. The Internal Audit Procedure details our audit process. Audits are undertaken by staff auditors who are trained in auditing and not directly responsible for the functions being audited within the organisation (where possible). Non-conformance observed is brought to the attention of the person responsible, and is recorded, documented and subject to timely corrective action to ensure full rectification. Audit reports are kept on the QMS Quality Records Register and related corrective and preventive action is to ensure full rectification. The Audit Register displays audits that have been scheduled or completed, and the action taken, as part of the organisation’s audit program. Audit Register The Audit Register is used to: Schedule internal and external audits Delegate tasks to a staff member to carry out or oversee audits View all current and past audits recorded and any associated action taken Print reports on the audit schedule Document1_rev date 01/08/2013 Page 24 of 26 8.2.3. Monitoring and measurement of processes The Audit Register contains scheduled audits to examine the effectiveness of the QMS and internal operational procedures. The Quality Coordinator QMS also produces a report providing statistics on activity within the electronic QMS. The SMT monitors and assesses the effectiveness of the QMS on a annual basis. 8.2.4. Monitoring and measurement of product The Audit Register contains scheduled audits to examine the effectiveness of service delivery. Service delivery is also measured through client feedback and approval from funders for ongoing financial support for the services provided. 8.3. Control of nonconforming product Non-conforming product can mean any process, service or product that is considered not to conform with agreed specifications, policies sand procedures. Non-conformances may be determined through incident, observation, client feedback or internal audits. This includes: Incoming goods from suppliers Services to the organisation provided by external sources Processes being carried out by the organisation that do not conform the stated policies or procedures Details of non-conformances are entered into the Continual Improvement Register and categorised as either corrective of preventive action. The QMS provides statistics on related non-conformities created as a result of supplier non-conformance, audit findings, client feedback, equipment failure and OHS incidents. The Control of Non-conforming Product Procedure details our processes. 8.4. Analysis of data Data relating to audit findings, program evaluations, compliance monitoring, client feedback, OHS incidents, equipment maintenance, and suppliers are recorded in the QMS which automatically reports the matter to management for decision and action. Statistics regarding how effectively the organisation is responding to this data is provided in statistical reports generated by the QMS. These statistics are provided as inputs to the SMT and CRC as per our agenda and reporting templates. 8.5. Improvement 8.5.1. Continual improvement Continual improvement is an ongoing activity through which opportunities for improvement are identified and actions are generated. This process is managed through the use of our Continual Improvement Register located in the Quality Coordinator Software. The Continual Improvement Register is used to: Record issues relating to non-conformance and suggestions for improvement from staff or from outside the organisation Delegate tasks to a staff member to carry out corrective or preventive action View all current and past client improvement suggestions and any associated action taken Print reports on continual improvement suggestions Document1_rev date 01/08/2013 Page 25 of 26 8.5.2. Corrective action Corrective action is determined and delegated by management through the Continual Improvement Register in our QMS. The Continual Improvement Register displays the background issue, suggestions for improvements to service delivery or business processes, and the action determined. 8.5.3. Preventive action Preventive action is determined and delegated by management through the Continual Improvement Register in our QMS. The Continual Improvement Register displays the background issue, suggestions for improvements to service delivery or business processes, and the action determined. Continual Improvement Register Pre-set categories within the Continual Improvement Register allow for the source of action to be identified eg audit finding, staff suggestion etc. Statistics can be generated to provide for analysis of the source of improvement actions and the occurrence of corrective and preventive actions within the organisation. Document1_rev date 01/08/2013 Page 26 of 26