Definitions (Webster's) - The Center for Human Services, UC Davis
 - The Center for Human Services, UC Davis")
Humboldt County
Department of Health and Human Services
Fiscal Essentials for Children’s Services
Forum
November 2009
Update: 10/23/09
1
Humboldt County
Department of Health and Human Services
Presenters:
• Phillip R. Crandall, Director
• Barbara LaHaie, Assistant Director, Programs
• Karolyn Stein, Director, Mental Health Branch
• Katherine Young, Director, Social Services Branch
• Susan Buckley, Director, Public Health Branch
• Connie Beck, Program Manager, Social Services
Branch
• Rochelle Trochtenberg, Youth Organizer, HCTAYC
2
Vision: We Won’t Back Down….
Children and Families Are A
Priority For Integrated Services
And Supports In Humboldt County
3
Definitions (Webster’s)
•
Collaborate – to cooperate with the enemy
•
Parallel – extending in the same direction and at a constant distance apart, so as to never meet
•
Silo – an airtight pit or tower
4
Definitions (Webster’s)
•
Integrate – to bring parts together into a whole
•
Transform – to change the condition, character, or function
•
I.T. (Integrative Transformation) – “… to bring parts together into a whole
…to change the condition…or function.”
5
Transformation
How? That’s the hard part!
In a nut shell Humboldt County is working to build a developmental “road map” to effect system transformation through:
Holistic services across departments
Centralized administrative and program support
Decentralized, mobile, field or home based services approaches
Concurrent high/low system interventions
Outcome based programming approaches
Evidence Based Practices (EBP’s)/promising practice or Practice Based
Evidence (PBE) approaches
Integrated approaches to State Initiatives:
Mental Health Services Act (MHSA)
Child Welfare Services Outcome Improvement Project (OIP) (aka
CWS Redesign)
6
Integrated Transformation
The “3 by 5” Approach:
3
•
•
•
Primary Prevention (Universal)
Secondary Intervention
(Selective)
Tertiary Intervention (Indicated)
5
•
•
•
•
•
Children, Youth and Families
Transition Age Youth
Adults
Older Adults
Community
7
Philosophy - Humboldt
• Placement of children out of county and/or in group homes is not a system goal;
• Prevention, early intervention and least restrictive placement through holistic services and supports is a system goal.
8
Outcomes
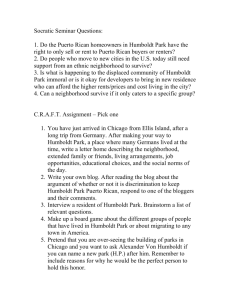
• The following 2 charts show the number of
Humboldt County children placed out of home in total and in group home settings each month by
CWS and Mental Health and associated monthly expenditures
• 23% decline in the total number of children placed Out of Home (OOH) and 28% decline in expenditures
• Reflects initiatives to maintain children in their homes or in the least restrictive safe environment
9
Total Out of Home (OOH) Placements & Expenditures
July 1997 to July 2009
(CWS & MHB)
350
300
250
200
150
100
50
0
$350
$300
$250
$200
$150
$100
$50
$-
Ju l-9
7
Ju l-9
8
Ju l-9
9
Ju l-0
0
Ju l-0
1
Ju l-0
2
Ju l-0
3
Ju l-0
4
Ju l-0
5
Ju l-0
6
Ju l-0
7
Ju l-0
8
Ju l-0
9
Total Out of Home Placements Total Expenditures
Source: Family Intervention Team Database, July 2009
10
Outcomes
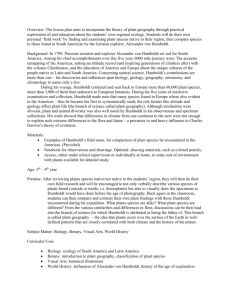
• Group home placements for DHHS have declined 94% from 16 youth in July 1997, to 1 youth in April 2009.
• Focusing on local, less restrictive placements has led to a 93% decrease in total group home expenditures for DHHS.
• Group homes have minimal positive outcomes for most youth.
• Goal: Zero DHHS group home placements.
11
Total Group Home (GH) Placements &
Expenditures July 1997 to July 2009
(CWS & MHB)
30
25
20
15
10
5
0
$120
$100
$80
$60
$40
$20
$-
Ju l-9
7
Ju l-9
8
Ju l-9
9
Ju l-0
0
Ju l-0
1
Ju l-0
2
Ju l-0
3
Ju l-0
4
Ju l-0
5
Ju l-0
6
Ju l-0
7
Ju l-0
8
Ju l-0
9
Total Group Home Placements Total Group Home Expenditures
Source: Family Intervention Team Database, July 2009
12
Outcomes
• Expanded Children’s Mental Health Services
Under Early Periodic Screening Diagnosis
Treatment (EPSDT) (Selective / Indicated)
• The following series of graphs reflect Humboldt
County’s commitment to increasing access to
Medi-Cal mental health services for children and families. All data reflect the most recent calendar year, 2008, and were extracted between January and April 2009.
13
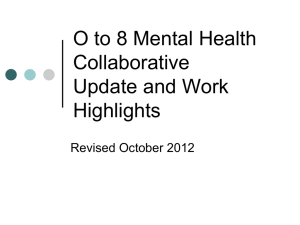
Medi-Cal Mental Health Penetration Rates for Foster Care
Calendar Year 2005 to 2008
Calendar Year 2005 to 2008
100%
80%
60%
66
.7
%
56
.3
%
59
.5
%
58
.3
7%
46
.5
%
48
.2
%
46
.0
%
49
.3
9%
53
.2
%
53
.9
%
55
.3
%
58
.1
1%
40%
20%
0%
Humboldt Small Counties Statewide
CY2005 CY2006 CY2007
Source: APS Healthcare, 2005-2009
CY2008
While there is room to improve, Humboldt exceeds Small
Counties and the State in terms of penetration of mental health services into the foster care population.
14
Medi-Cal Mental Health Penetration Rate for
Foster Care Low Intensity Services
Medi-Cal Mental Health Penetration Rate for Foster Youth in to Low Intensity
Calendar Year 2008
Humboldt County’s rates for
Linkage/Brokerage and Outpatient
Services are above statewide and small county percentages which may contribute to early treatment success in terms of reducing the need for more intrusive or restrictive services and placements, such as group homes or out of home care.
70%
60%
50%
40%
30%
20%
10%
0%
31
.5
%
26
.2
%
27
.1
%
Linkage/
Brokerage
57
.2
%
46
.6
%
Outpatient
Services
55
.3
%
16
.0
%
14
.4
%
19
.3
%
Medication
Support
Humboldt Small County Statewide
Source: APS Healthcare, 2009
15
Medi-Cal Mental Health Penetration Rates for
Foster Care High Intensity Services
Medi-Cal Mental Health Penetration Rate for Foster Youth into High Intensity
5%
4%
3%
2%
1%
0%
3.
52
%
0.
39
%
1.
25
% 1.
77
%
1.
56
%
0.
63
%
0.
99
%
1.
38
%
0%
24 Hour Services 23 Hour Services Day Treatment
2.
33
%
1.
20
%
2.
22
%
Therapeutic
Behavior Support
Humboldt Small County
Source: APS Healthcare, 2009
Statewide
This chart compares the percentage of foster care children and youth who receive high intensity inpatient and outpatient mental health services in Humboldt County with Statewide percentages.
16
Approved Medi-Cal Mental Health Claims for
Foster Children 0-5 Years
Approved Medi-Cal Mental Health Claims for Foster Children 0-5 Years Calendar
Calendar Years 2005 to 2008
$12,000
$10,000
$8,000
$6,000
$4,000
$2,000
$0
$
9,
76
2
$
7,
75
2
$
3,
03
3
$
3,
80
4
$
3,
05
5
$
2,
74
8
$
3,
27
9
$
3,
43
0
$
3,
45
4
Humboldt Small County Statewide
CY2006 CY2007 CY2008
Source: APS Healthcare, 2009
17
Approved Medi-Cal Mental Health Claims for
Foster Children 6-18 Years
Calendar Years 2005 to 2008
Years 2005 to 2008
$18,000
$15,000
$12,000
$9,000
$6,000
$3,000
$0
$
13
,7
23
$
8,
62
8
$
10
,2
47
$
6,
62
7
$
6,
25
3
$
7,
10
5
$
7,
24
5
$
7,
56
7
$
7,
85
3
Humboldt Small County Statewide
CY2006 CY2007 CY2008
Source: APS Healthcare, 2009
18
Medi-Cal Mental Health Penetration Rate for Transition
Medi-Cal Mental Health Penetration Rate for Transition Age Youth in Foster Care
Aged Youth in Foster Care (Ages 16-25)
Calendar Year 2008
120%
100%
80%
60%
40%
20%
0%
96.72%
69.55%
77.69%
Humboldt Small County Statewide
Source: APS Healthcare, 2009
Humboldt County served 20% more of the TAY foster care population than the statewide average and 28% more than the small counties average.
19
$12,000
$10,000
$8,000
$6,000
$4,000
$2,000
$0
Medi-Cal Mental Health Approved Claims for TAY Foster Youth (16-25)
Approved Claims for TAY Foster Youth CY2008
Calendar Year 2008
$9,387
$7,114
$7,897
Humboldt Small County
Source: APS Healthcare, 2009
Statewide
Humboldt had
16% and 24% more approved claims for Medi-
Cal mental health services than the statewide or small county average, respectively.
20
In Review
Humboldt County uses the following service approaches that demonstrate promise:
• Holistic (e.g. involve Social Services, Behavioral
Health, Public Health, Community, Stakeholders)
• Home and/or Community Based
• Involve concurrent low/high end approaches
• A mix of Promising Practices, EBP’s, PBE
• Linked in terms of launch sites and services
21
22
FISCAL STRATEGIES
Humboldt County Department of Health and
Human Services has a long history of braiding funding streams and integrating to better serve Children and Families.
23
Title XIX
• In 1996 Social Services and Public Health began collaboration utilizing Title XIX funds in the Alternative Response Team
(ART).
– Skilled Professional Medical Persons (SPMP) claiming in Social Services County Expense
Claim
– Target Case Management (TCM) and Medi-
Cal Administrative Activities (MAA) through
Public Health.
24
Title XIX (continued)
• Through the Mental Health Branch,
EPSDT is utilized to expand services to children and families by integrating specialty mental health services in existing children’s programs.
25
Non-Federal Foster Care
• In 1998, Humboldt became the first county to utilize non federal foster care funds in addition to
EPSDT claiming for the SB163 Wraparound
Services program using public agency model.
• Humboldt County’s Child Welfare Services,
Mental Health and Probation collaborated to provide Wraparound Services to children in high level placement or at risk of such placement.
26
State Children’s Trust Fund,
Title IV E, Promoting Safe and
Stable Families
• In 2004/2005, Humboldt was one of 11 counties which were implementing
Differential Response and received allocations from State Children’s Trust
Fund, Title IVE, and Promoting Safe and
Stable Families.
27
State Children’s Trust Fund,
Title IV E, Promoting Safe and
Stable Families continued.
• In 2005/2006, Humboldt County submitted a county plan that was approved through
Child Welfare Services Outcome
Improvement Plans to increase system improvement.
28
Prop 63 –
Mental Health Services Act
• In 2005, Humboldt received Mental Health
Services Act (MHSA) Funds to expand programs for children and families and to further integrate mental health services in existing programs.
29
CalWORKs
• In 2007, Humboldt County started the
Linkages Program utilizing CalWORKs funding to provide services for children and families linked by Child Welfare
Services and the CalWORKs Program.
30
TANF Emergency Contingency
Fund
• American Recovery and Reinvestment Act
(ARRA) of 2009
• Utilizing this funding in several program areas with eligible target populations.
31
32
Integrated Transformation
The “3 by 5” Approach:
3
•
•
•
Primary Prevention (Universal)
Secondary Intervention
(Selective)
Tertiary Intervention (Indicated)
5
•
•
•
•
•
Children, Youth and Families
Transition Age Youth
Adults
Older Adults
Community
33
Universal Approaches:
Examples
• ATOD prevention
• FRC partnerships
• Healthy Kids Humboldt
34
Selective Approaches:
Examples
• Incredible Years
• Nurse Family Partnership
• Adolescent Family Life Program
35
Indicated Approaches:
Examples
• Functional Family Therapy
(FFT)
• Parent Child Interaction
Therapy (PCIT)
• Aggression Replacement
Therapy (ART) / Regional
Facility (RF)
• HCTAYC
• Family Intervention Team (FIT)
• Family Finding (HOPE)
• Team Decision Making (TDM)
• Differential Response (DR)
• Independent Living Services
• Children’s Shelter
• Wraparound
• Intensive Mental Health Case
Management
• Therapeutic Behavioral
Services
• Multiple Assistance Center
• Many services in the list include integrated DHHS services as well as partnerships with Probation,
Education, or FRC’s
36
37
Family Resource Center Initiative
38
The supports and resources offered by the seventeen Centers in Humboldt County vary depending on community needs, geographic location and funding. This chart illustrates the types of services offered in FRCs and how many centers provide each type.
Services available through FRCs and Number of
FRCs Offering Each Service
Number of FRCs Providing Service
12 14 0 2 4 6 8 10
Adult ed. classes
After school
Anger management
Childcare referral
Com. service/vol.
Dental clinic services
Drop in services
Emergency needs
Employment/job ready
English
Family/ comm. events
Family support
Food distribution - reg.
Health education
Home visits
Information and
Life skills
Medical Clinic
Meeting rooms
Mental health -counsel
Mentoring
Nutrition/fitness ed.
Parenting classes/res.
Play groups
Recreation programs
School to home
Student peer groups
Substance abuse
Summer recreation
Supervised
Technology access
Transportation assist.
Tutoring (academic)
Source: Healthy Start & Schools Partnership records, July 2009
39
16
Family Resource Centers:
Fiscal Strategies
• Child Welfare Services Outcome
Improvement Funds
• CalWORKs
• SPMP
• TCM/MAA
• TANF ECF – Short term non-recurrent benefit
40
Mobile Engagement Fleet
(Universal / Selective / Indicated)
Decentralizing and Integrating DHHS Services
41
Why Decentralize?
• The County has a total area of
3,573 square miles
• In response to the Department of Health and Human Services
Strategic Plan
• Transportation opportunities to
Eureka are very limited
• For example, only 45%
CalWORKs recipients live in
Eureka – the rest are distributed throughout the length of the county
42
Three vehicles, each with its own design, will provide services to the outlying areas of Humboldt.
Social Services Behavioral Health Public Health
– CalWORKs/
Welfare-to-Work
– Employment
Training Division
– Food Stamp and
Medi-Cal Outreach
Services
– Child Welfare and
Welfare-to-Work
Linkages opportunities
– Assessments
– Case Managers
– Medication
Support
– Mobile Crisis
Response
– Alcohol and Other
Drug Services and Referrals
– Homeless
Outreach
– Support to local communities in keeping with community values
– Health Education on Topics
Including:
• Nutrition
• Physical Activity
• Tobacco
Cessation
• Post-Partum
Depression
– Access to WIC
Nutrition Program
Information
– Suicide Prevention
43
Services we will be able to take to our clients
– and communities wherever they live.
• One-stop application for all DHHS services, for example:
● Food Stamps/Medi-Cal
● CalWORKs/Welfare-to-Work
● Mental Health Services Act programs
● Healthy Moms
● Healthy Kids/Healthy Families
● Women, Infants and Children Nutrition Program
● California Children’s Services ● Children’s Health and Disability Prevention Program
• Eligibility maintenance and case management for DHHS services
● Creation of individual employment development plans
● Vocational counseling and employment training
● Life skills classes
● Development of Welfare-to-Work employment opportunity sites
• Community Outreach opportunities
● Job Fairs
● Healthy lifestyle promotion
● Drug, alcohol and tobacco prevention outreach
● Employment Training Division Targets of Opportunity
● And others as identified
44
Expected Outcomes
• An increase of the number of people living in remote areas accessing DHHS services and supports, resulting in:
– The ability of more children and families to access social services, mental health, alcohol and other drug and public health services (Universal / Selective / Indicated)
– Increased participation by CalWORKs recipients in the
Welfare-to-Work program
• Increased integrated services with our community partners:
– Family Resource Centers
– Local public and private non-profits
– Local business organizations
– Stakeholders
45
Mobile Engagement Vehicle:
Fiscal Strategies
• CalWORKs Single Allocation
• EPSDT/Title XIX
• SPMP
• TANF ECF
• MHSA
46
47
Team Decision Making
48
Team Decision Making (TDM)
(Indicated)
• Involving not just foster parents and caseworkers, but also birth families and community members in all placement decisions to ensure a network of support for the children and for the adults who care for them.
49
Team Decision Making (TDM)
CWS and Probation
Team Decision Making (TDM) meetings, a component of the Family to Family Initiative, are held for all decisions that affect a youth's placement in foster care and involve:
• Birth Families
• Youth
• Support Systems
• Foster Families
• Case Workers
• Community Members
• Clinicians
• Nurses
50
Team Decision Making
Team Decision Making meetings are based on the beliefs that:
A group is more effective in making good decisions than an individual
Families are the experts on their needs
Community members are natural allies to the family as well as experts on the community's resources. DHHS has increased collaboration with FRCs overall and they currently participate in TDMs if appropriate.
51
Total Team Decision Making Meetings Per Month
Total Team Decision Making Meetings Per Month
September 2006 to May 2009
30
25
20
15
10
5
0
Se p-0
6
D ec-0
6
Ma r-0
7
Ju n-0
7
Se p-0
7
D ec-0
7
Ma r-0
8
Ju n-0
8
Se p-0
8
D ec-0
8
Ma r-0
9
Total TDM Meetings per Month
Source: Social Services Branch TDM Data Base, 6/17/09
This chart shows the number of TDM meetings held each month
September 2006 through April 2008. The numbers vary, depending on how many children are considered for placement or placement change each month.
52
by Meeting Purpose
September 2006 to May 2009
September 2006 to May 2009
600
500
400
300
200
100
0
Se p-0
6
Ja n-0
7
Ma y-0
7
Se p-0
7
Ja n-0
8
Ma y-0
8
Se p-0
8
Ja n-0
9
Ma y-0
9
Accumulative Reunification
TDM Meetings
Accumulative Placement
Change TDM Meetings
Accumulative Emergency
Placement TDM Meetings
Accumulative Imminent
Risk TDM Meetings
Source: Social Services Branch
TDM Data Base, 6/17/09
This chart illustrates the accumulative total of TDM meetings held through each month by each of the four conditions: Reunification,
Emergency Placement, or Imminent Risk of Removal Placement
Change. Team Decision Making was phased in over time. Full implementation began in early 2007 and was recently made mandatory for all placement decisions meeting TDM criteria.
53
Recommendations Resulting from CWS TDM Meetings
Conducted for the Primary Purpose of Placement
Conducted for the Primary Purpose of
N = 309
September 2006 to May 2009
120
100
80
60
40
20
0
92
73
96
48
Maintain
Current
Placement
Change to
Lower
Level
Placement
Change to
Same
Level
Placement
Change to
More
Restrictive
Placement
Source: Social Services Branch TDM Database (6/17/09)
Since TDM was implemented in
Humboldt County,
53% of the meetings for placement changes resulted in recommendations to maintain the child in the same out-ofhome placement or a less restrictive level of care. These recommendations result in increased stability for the child.
54
TDM meetings are held for four primary purposes:
– Imminent risk of removal from home
– Emergency placement
– Placement change
– Reunification / Exit from placement
55
Total Youth Involved in TDM Meetings Compared to
TDM Meetings Compared to
Total Age Appropriate Youth Who Attended
40
30
20
10
0
Se p-0
6
Ja n-0
7
Ma y-0
7
Se p-0
7
Ja n-0
8
Ma y-0
8
Se p-0
8
Ja n-0
9
Ma y-0
9
Total Youth Involved
Total Youth Attended
Source: Social Services Branch TDM Data Base, 6/17/09
This chart shows how many youth were the focus of TDM meetings compared to how many youth attended the meetings. (Youth age 10 and over are considered “age appropriate” to participate in TDMs.)
56
Summary of TDM Meetings
September 1, 2006 through July 31, 2009
A total of 586 TDM Meetings have been held for 799 youth for the following purposes:
• Imminent Risk of Placement
• Emergency Placement
• Placement Move
• Exit from Placement
114
208
324
56
57
TDM Recommendations
Imminent Risk of Placement TDM Recommendations :
•Leave youth at home
•Place youth in out-of-home placement
76%
24%
TDM Results Following Initial Immediate Removal
(Emergency Placement):
•Youth returns home
•Youth remains in out-of-home care
38%
62%
58
Team Decision Making:
Fiscal Strategies
• Walter S Foundation Grant funds
• Outcome Improvement Funds
• CWS Basic Allocation
• EPSDT
59
60
Launching of the Children’s
Mental Health Foster Care
Initiative
61
Goals
To stabilize and maintain youth in the least restrictive placement setting
– Every youth in foster care is assessed for behavioral and physical health services.
Emergency requests are referred the same day for immediate intervention.
Urgent requests are scheduled within two working days.
Intermediate and lower level requests are scheduled within 5 days.
– If assessed to need behavioral health services, a treatment plan is developed by a mental health clinician which may include:
• Individual, group and/or family counseling
• Case management services
• Referral to an Evidence based practice
• Medication evaluation and support services
• WRAP around services
• Therapeutic Behavioral Services
– Permanent connections for all youth transitioning out of foster care.
62
Transforming a System
• Who are the partners?
– Humboldt County Transition Age Youth
Collaboration (HCTAYC)
– Children Youth and Family Services, Mental
Health Branch
– Foster Care Nursing, Public Health Branch
– Child Welfare Services, Social Services
Branch
63
How did we do it?
• DATA TRACKING
– Youth in the Permanency Planning (PP) Units were cross referenced in both the
CYFS and CWS/CMS electronic data management systems and a single data tracking tool was developed.
– Program Managers and Supervisors from all three branches continue to meet weekly to review the PP unit caseload and to identify youth in need of either a MHST and/or assessment. Public health needs were also reviewed to insure that youth are receiving medical and dental care.
• INTEGRATION
– The Program Managers from CYFS and CWS met to identify youth in the PP units who were in need of an assessment.
– Processes were reviewed to streamline referrals and the data tracking tool was expanded to include public health information.
• POLICY and PROCEDURES
– Policy and Procedures for referring youth from CWS to CYFS were reviewed and distributed to all integrated staff cross discipline.
– Training on the need for mental health services, for youth in foster care, was provided across disciplines to insure that coordinated support was provided to every youth in care
• STAFFING (Initial)
– 10 Case Managers, 2 Mental Health Clinicians and a Supervising Clinician were assigned to the project 64
What We Have Learned
Through 11/3/2009
Looking at various points in time, as predicted in literature, over 80% of our youth in care experience a Serious Emotional
Disturbance.
65
Foster Care Behavioral Health Expansion
Mental Health Services Snapshot
August 6, 2009
Permanency
Planning Unit
Family
Reunification
Unit
Family
Maintenance
Unit
17 55 86 Total children per unit, age 12+ mo.
MH Services – MHB Only 19 21 17
MH Services - MHB + Provider
MH Services – Provider Only
Assessed
– No diagnosis
Assessment pending
9
13
15
15
6
18
3
4
1
14
2
8
Assessment declined
Pending closure to CWS
Assessed
– refusing services
4
1
1
3
0
0
4
0
0
66
Foster Care Behavioral Health Expansion
Mental Health Services Snapshot
August 6, 2009
Receiving Services at MHB
Permanency
Planning Unit
Family
Reunification
Unit
Family
Maintenance
Unit
Therapy 24 19 17
Case Management
Medication Support
Therapeutic
Behavioral Services
Hospitalized in the last 6 Mo.
0
0
20
7
4
1
19
2
2
0
15
1
67
Foster Care Behavioral Health
Expansion:
Preliminary Outcomes – How
• 67 youth tracked to date
• Reviewed the number of placement changes between the two evaluation periods
– Pre-project implementation: 1/1/08 to 7/31/08
– Post-project implementation: 1/1/09 to 7/31/09
68
Foster Care Behavioral Health Expansion:
Preliminary Outcomes - Results
Number of Placements
Post Implementation (Jan. 1 - Jul. 31, 2009) vs.
Pre Implementation (Jan. 1 - Jul. 31, 2008)
Number of
Youth
(Percentage)
Decrease or no change in # placements 58 (86%)
• No change in # placements*
• Decrease in # placements
37 (55%)
21 (31%)
Increase in # of placements 9 (13%)
*32 youth had no placement changes in either reporting period
69
Strategies / Successes:
Children’s Mental Health
Medi-Cal Mental Health Penetration Rate for
Foster Care
Calendar Year 2007
100%
77.3%
80%
64.3%
60%
27.7%
40%
18.6%
20%
0%
0-5 yrs 6-18 yrs
Humboldt Statewide
Source: DMH Approved Claims and MMEF Data,
Prepared July 2008
This chart shows the percent of
Foster Care children and youth who receive mental health services in Humboldt
County vs. the statewide percentage.
70
Next Steps
• Comprehensive mental health assessments for all youth in the Family Reunification Unit are also being provided to ensure that all youth needing behavioral health services are receiving them. Children new to care are being screened and referred for mental health assessments as an “urgent” referral with assessments provided within two working days of the referral whenever possible.
• Data collection of outcomes: clinical scales, placement stability, frequency of placement changes, successful completion of high school, transition to independence.
• Develop specialized services for those who are not in a natural home setting.
• Assess and expand effective behavioral health approaches
(e.g. Trauma-Focused Cognitive-Behavioral Therapy).
71
Foster Care Expansion:
Fiscal Strategies
• EPSDT/Title XIX
• CWS Basic, OIP
• SPMP
• TCM/MAA
• TANF ECF
• MHSA
72
73
Humboldt County Transition Age
Youth Collaboration (HCTAYC)
Teaching Old Dogs New Tricks
74
Humboldt County
Transition Age Youth Collaboration
• Like every county in California, Humboldt County includes a population of transition age youth who, because of a lack of family or other support, are vulnerable and in need of county system assistance.
• Demonstrating commitment to serve these youth in the best possible ways, Humboldt County began a five year process in 2008 to increase transition age youth (TAY) input and genuine engagement in systems delivery and improvement.
75
Purpose:
• Humboldt County DHHS is committed to better engaging youth to improve systems and service delivery to transition age youth, including, among others, homeless youth, former foster youth and youth with behavioral health needs.
• Humboldt County youth from California Youth Connection
(CYC) and the emerging statewide mental health youth advocacy organization Youth In Mind (YIM) are eager to improve and increase their participation in the local systems change process.
• Youth have additionally expressed interest in receiving capacity building and leadership development to further enhance and increase their contributions.
76
2008-2009 Summary:
• A group of committed individuals and existing youth development organizations engaged in a one year planning and project development process to improve services to transition aged youth over a five year period.
– Y.O.U.T.H. (Youth Offering Unique Tangible Help)
Training Project
– California Youth Connection
– Youth In Mind
– Humboldt County DHHS
– Humboldt County TAY
• Policy recommendations were developed and delivered to DHHS for the Children’s Center, Sempervirens, Crisis
Hotline and Psychiatric Emergency Services.
77
2008-2009 Summary continued:
• A Youth Advisory Board of Humboldt youth was formed.
These youth, ages 16-30, were compensated for their commitment to serve for at least the first year of the project.
• A HCTAYC office was opened in the Independent Living
Skills office.
• Three leadership development trainings were offered to
Humboldt County TAY on the following topics:
– Developing Policy Recommendations
– Facilitation Skills
– Public Speaking
78
2008-2009 Summary continued:
• Humboldt youth attended various conferences on the topics of mental health, independent living skills, and foster care improvement.
• Humboldtyouth.org, a website dedicated to HCTAYC and improving services offered to TAY in Humboldt
County, was launched.
• A Digital Storytelling workshop was organized, and 10
Humboldt youth developed documentaries about their experience with systems of care in Humboldt County, and their recommendations for improvement.
79
80
2009-2010 Goals:
• Continue recruiting and compensating youth to serve on the Youth Advisory Board.
• Continue working with DHHS departments on the policy recommendations made in the first year to assist with implementation and developing ongoing methods of feedback.
• Prepare and present a new round of policy recommendations on TAY services in foster care, housing and homelessness.
• Offer another Digital Storytelling workshop for Humboldt youth to tell their story in their own way.
81
2009-2010 Goals continued:
• Plan for a TAY center in Humboldt County. This meeting place for youth will be developed with the input of youth, county employees, professionals in TAY fields, and community partners.
• Continue offering professional development trainings to Humboldt TAY.
• Develop ongoing mechanisms for youth concerns and recommendations to be made on various Humboldt County TAY services.
82
Communication:
– Project staff and Youth Advisory Board continue to participate in state and nationwide conferences and events sharing the success of the initiative.
– Best practices and recommendations are being developed for other projects to reproduce the success of the collaboration.
– Documentation of all work is done on a regular basis allowing for academic and professional publishing opportunities to be pursued.
83
Evaluation Plan:
• Lisa Korwin of Korwin Consulting has led the program and training evaluations for the Y.O.U.T.H.
Training Project since 2002.
– Korwin Consulting developed a qualitative evaluation to track the collaboration’s success in initiating systems change in Humboldt County
– The evaluation also tracked the successes (and challenges) of the collaborative process
• This evaluation process will be continued in
2009-2010.
84
HCTAYC:
Fiscal Strategies
• Mental Health Services Act (prop 63)
• Child Welfare Services Outcome
Improvement (SCTF, Title IV E, PSSF)
85
86
Other Components of Integration
• Direct Mental Health, Public Health, and FRC integration into the CWS Differential Response process
• Family to Family: resource family recruitment, development, and support
• Integrated Team Decision Making
• New Horizons Regional Facility
• Evidence Based Practices
• Youth Transition Action Team
• California Connected by 25 Initiative
• HOPE (Humboldt Offers Permanency for Everyone)
• Independent Living Program
• THP/THP+
• MHSA Programs
87